
Abstract
OBJECTIVE: Analyze the variability of anatomic relations between the sigmoid sinus and other surgical landmarks within the mastoid cavity to establish a classification of sinus location to facilitate surgical planning.
STUDY DESIGN: A descriptive study of surgical landmarks using 96 temporal bones from the Temporal Bone Laboratory at the Department of Otorhinolaryngology, Valle University at Cali, Colombia.
METHODS: A dissection simulating a canal wall-up mastoidectomy extended to include exposure of the facial recess, epitympanum, and sigmoid sinus was performed on 96 adult disease-free temporal bones. Seven standard measurements were taken on each bone between the sigmoid sinus and other structures in the mastoid cavity. All data were analyzed using Epi-Info 2000.
RESULTS: This parametric study was consistent with three classes of anatomic variations in the location of the sigmoid sinus (type 1, type 2, and type 3) based on a Gaussian distribution of the seven variables.
CONCLUSIONS: Variability in the anatomic location of the sigmoid sinus in the mastoid cavity is common and has surgical relevance.
SIGNIFICANCE: This classification will help to rapidly identify the sigmoid sinus relationship within the mastoid cavity and to use the sigmoid sinus as a landmark during ear surgery in those cases in which traditional landmarks, such as the posterior auditory canal wall or the semicircular canals, are destroyed by a pathologic process.
The SS is a venous space between the endosteum of the occipital bone and the dura and possesses an endothelium lining without valves or muscle in its walls. 1 The SS originates at the junction of the transverse and the superior petrosal sinuses at the superior border of the petrous bone, from this point on changes direction in the vertical plane toward the medial portion of the mastoid cavity carving a deep canal in an S form and terminates anteriorly at the jugular bulb. 2,3
The sino-dural angle is formed at the junction of the SS and superior petrosal sinus. The SS forms the posterior limit of Trautmann's triangle. An anterior location of the SS will limit access to the internal auditory canal via a translabyrinthine approach. 4,5 Also, an anterior or a medial location of the SS limits access to the endolymphatic sac near the posterior semicircular canal. 6
Although variability in the location of the SS is well known, a parametric study has not been performed to date of the location of the SS in relation to other surgical landmarks such as the semicircular canals or spine of Henle.
MATERIALS AND METHODS
Ninety-six adult temporal bones from individuals with no history of ear disease at the Valle University Department of Otorhinolaryngology Temporal Bone Laboratory at Cali, Colombia were employed. Each bone was dissected simulating a canal wall-up mastoidectomy with extension to expose the facial recess, epitympanum, and SS. 7,8 Fifty-one dissections were performed by the senior author (P.B.S.) and 45 were performed by the coauthor (F.G.E.). After completion of each dissection, standard measurements were done by the two authors independently.
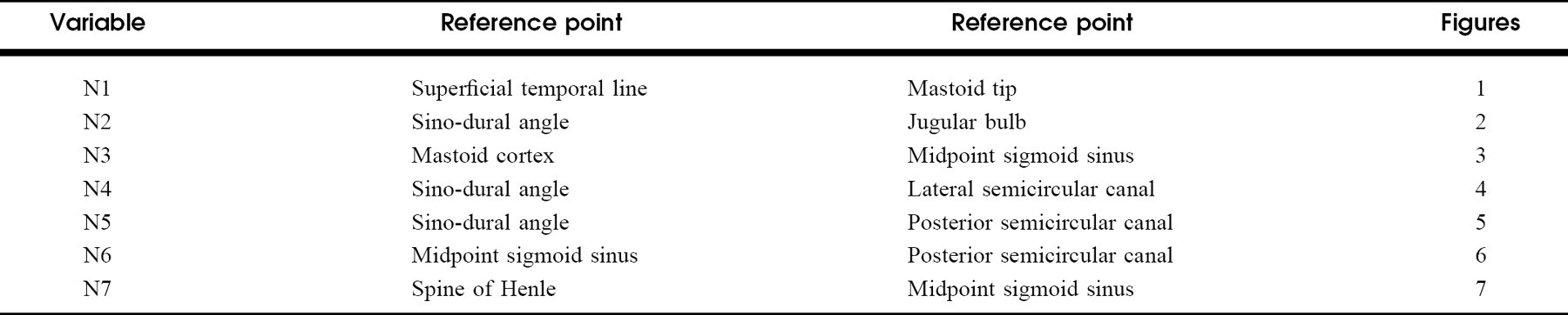
Measurements were performed using a standard compass (Faber Castell ref 174246), a standard 20-cm ruler (Faber Castell ref 814-20), and a precision compass (Faber Castel ref 174220) for measures less than 1 cm. Seven variables (N1-N7) were measured for each temporal bone and are presented in Table 1. Statistical analysis was completed using Epi-Info 2000 (Version 1.1.2 released November 2, 2001 from Centers for Disease Control and Prevention, Atlanta, GA) and are presented in Table 2.
Variable number and reference point for each measurement
Gaussen distribution of values for seven measurements (mm) taken from 96 adult temporal bones
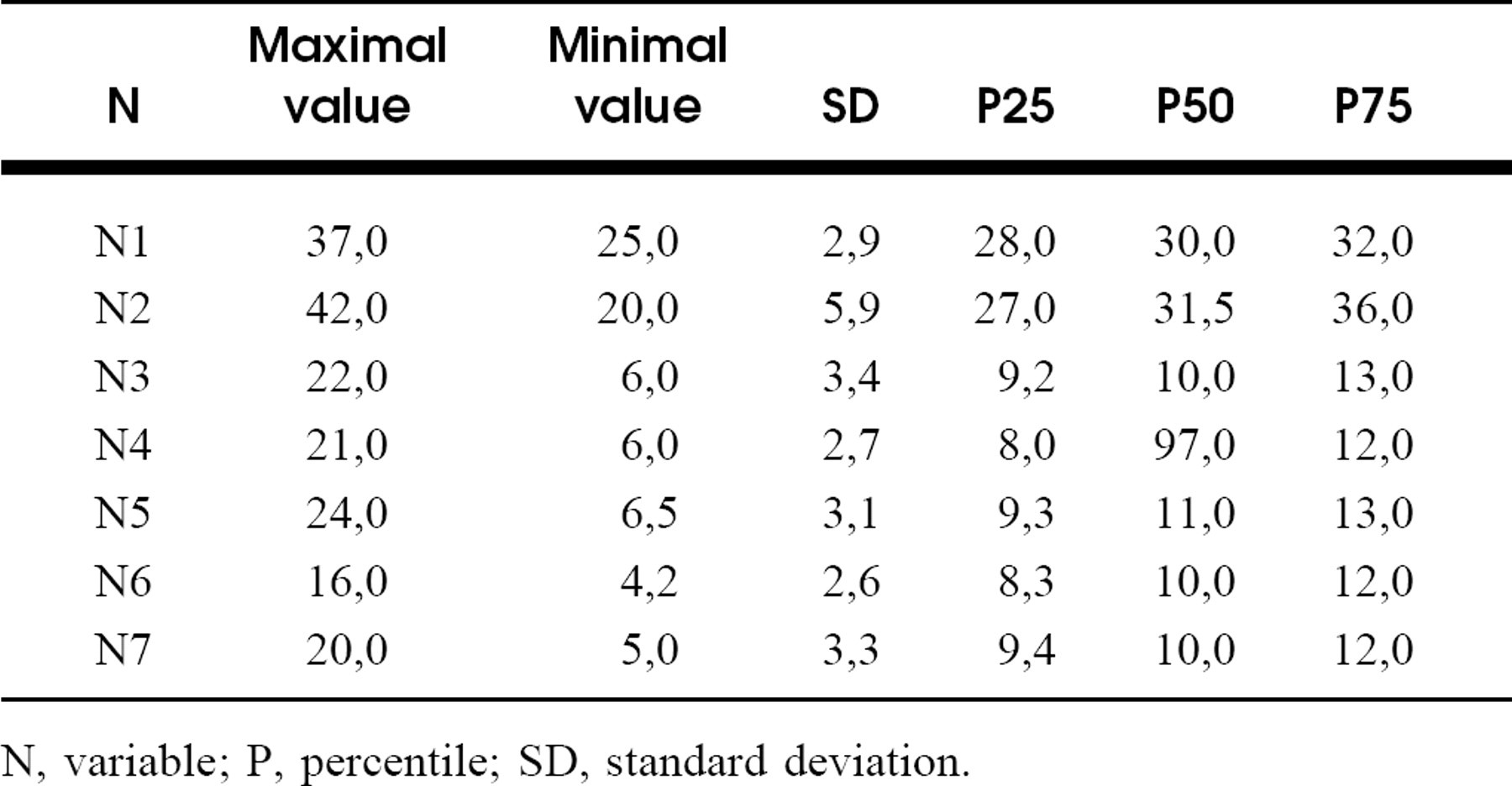
N, variable; P, percentile; SD, standard deviation.
RESULTS
The data for each of the seven variables (N1-N7) are shown in Table 2 (Figs 1–7). A Gaussian distribution was found for each variable. The mode in all variables was most common between percentile 25 and percentile 75. Hence, this was considered as the normal anatomic range (NAR) for each measurement. The values below percentile 25 and above percentile 75 were considered as deviations from the NAR (Table 3). Three distinct anatomic variations in the location of the sigmoid sinus in the mastoid cavity were found: type 1 (22.3%), type 2 (57.5%), and type 3 (20.2%; Figs 8–10 and Table 3).
In type 1, the location of the sigmoid sinus was posterior, enlarging Trautmann's triangle. In type 2 (the most common), the SS was located anteriorly diminishing the size of Trautmann's triangle. In type 3, the SS was medially displaced which also reduced the area of Trautmann's triangle.
DISCUSSION
Anatomic variations of the SS are well known. However, classification of the location of the SS in relation to other surgical landmarks has not been done previously. Shatz and Sade 9 measured the distance from the lateral sinus to the external auditory canal and found it to be significantly smaller in patients with sclerotic mastoids, a finding that they interpreted as supporting a hereditary theory for chronic otitis media (COM). 10 In our study, in 96 temporal bones without COM, this finding was present in 78% (57.2% type 2, and 20.2% type 3). Paparella and Sajjadi 11 described an anteriorly displaced and medially displaced lateral sinus and the consequent tightening of the Trautmann's triangle in patients with Meniere's disease. 8 According to our study with disease-free temporal bones, this finding was present in 78% of the mastoids examined, as previously described.
Classic anatomic descriptions 1–3,10 define the sigmoid sinus as the posterior limit of both the mastoid cavity and Trautmann's triangle. A large Trautmann's triangle was the exception rather than the rule because it was found in only 22.3% of the temporal bones (type 1). In fact, the distance from the SS to the mastoid cortex (N3), was highly variable because of the space occupied by the retrosigmoid cells in the mastoid (6–22 mm).
Whether the location of the SS in the mastoid cavity has any significance in the pathogenesis of pathologic processes such as COM or Meniere's disease remains controversial, because the anatomic variations of the sigmoid sinus mentioned in these diseases are similar to those found in our study, 78% of temporal bones with no evidence of ear disease. This suggests that the location of the sigmoid sinus found by Paparella and Shatz is also common in disease free mastoids. 9,11,12
From the data shown in Table 2, we found a significant correlation between the sinus length (N2), the mastoid length in the vertical plane (N1), and the sinus location in the mastoid cavity. This was used as the main determinant for the classification proposed in this study (Table 3). Turgut and Tos 13 measured the shortest distance between sigmoid sinus and external auditory canal as a parameter of the SS location in the mastoid and compared this measurement with the degree of mastoid pneumatization and mastoid length. They found that the length of the mastoid process was significantly shorter in specimens with poor pneumatization compared with those with good pneumatization. However, there was no significant effect of pneumatization on the location of the SS. These results differ from those presented here. However the findings of Turgut and Tos 13 are based on 60 temporal bones and a single anatomic parameter (the shortest distance between the SS and the external auditory canal wall).
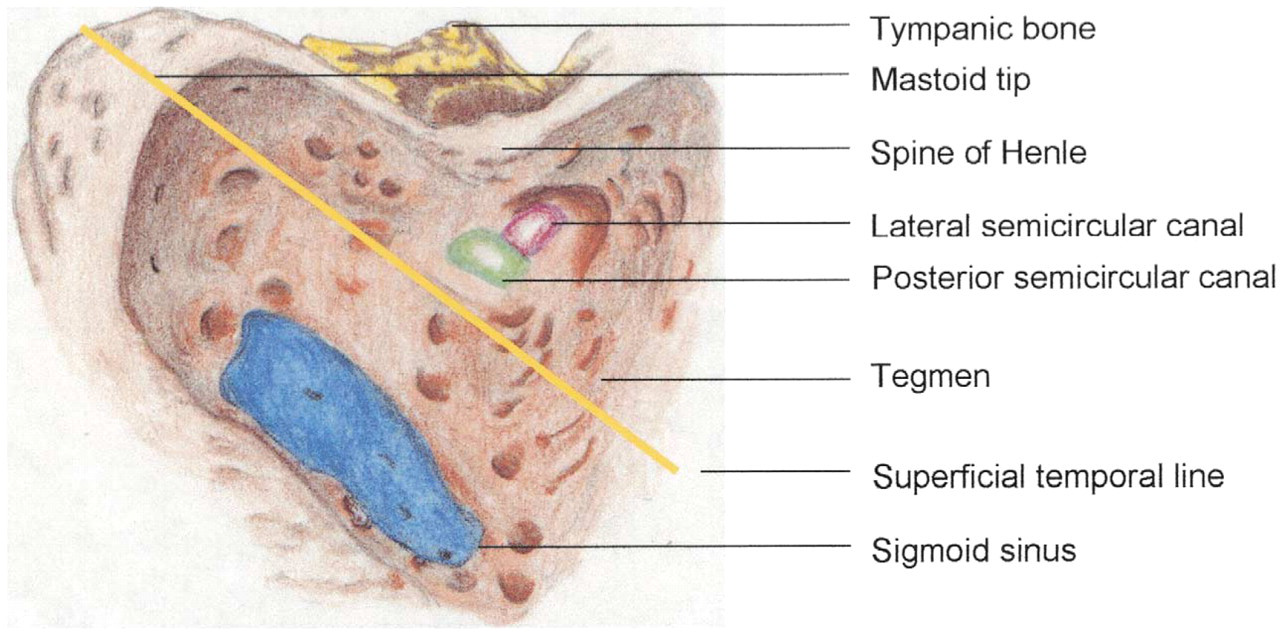
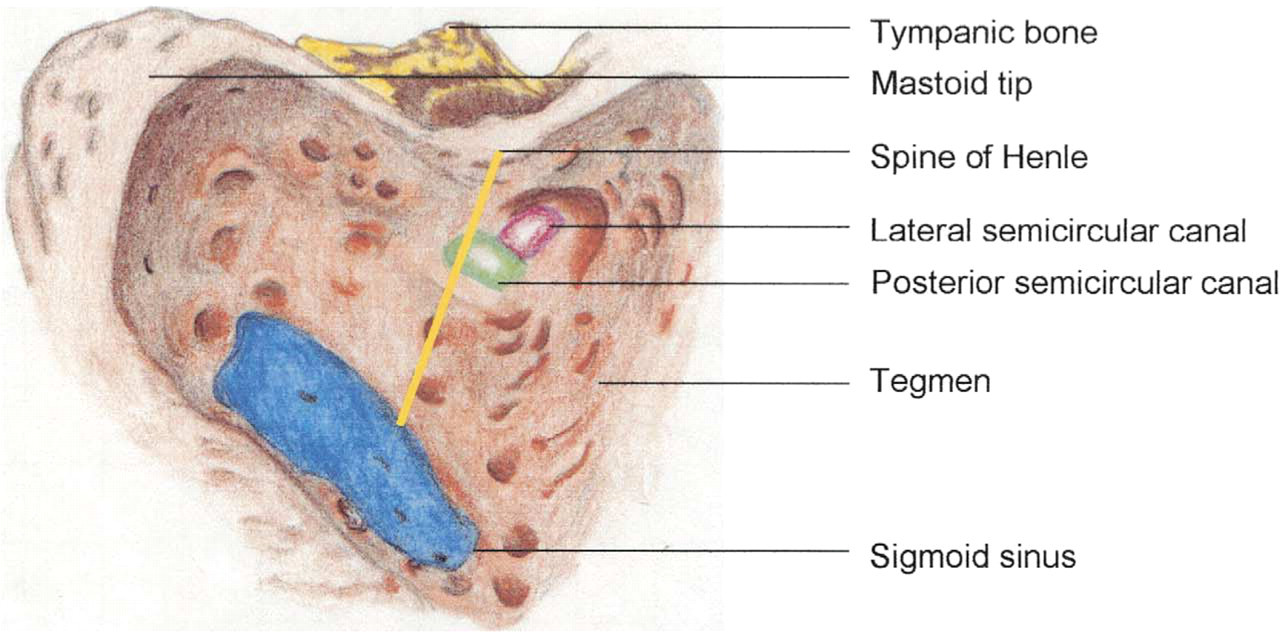
Variable N1 (yellow line), mastoid length in the vertical plane.
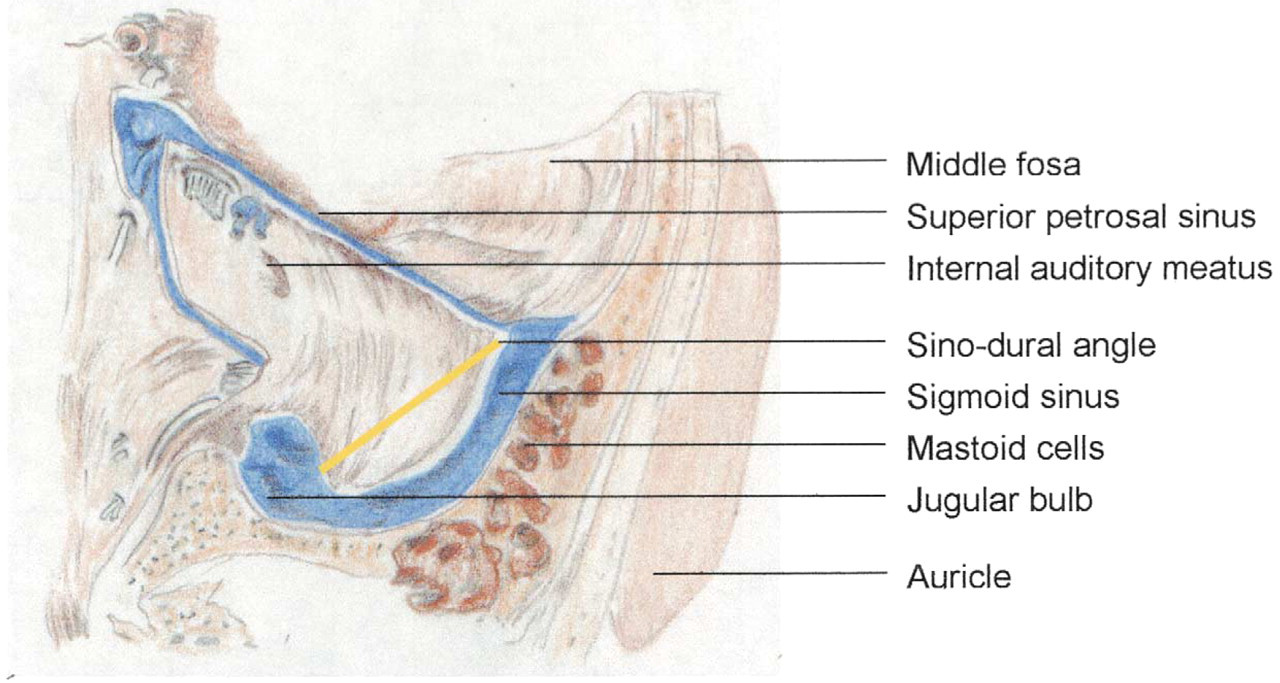
Anterior wall diagram of the posterior fossa from a suboccipital view. Variable N2 (yellow line), sigmoid sinus length.
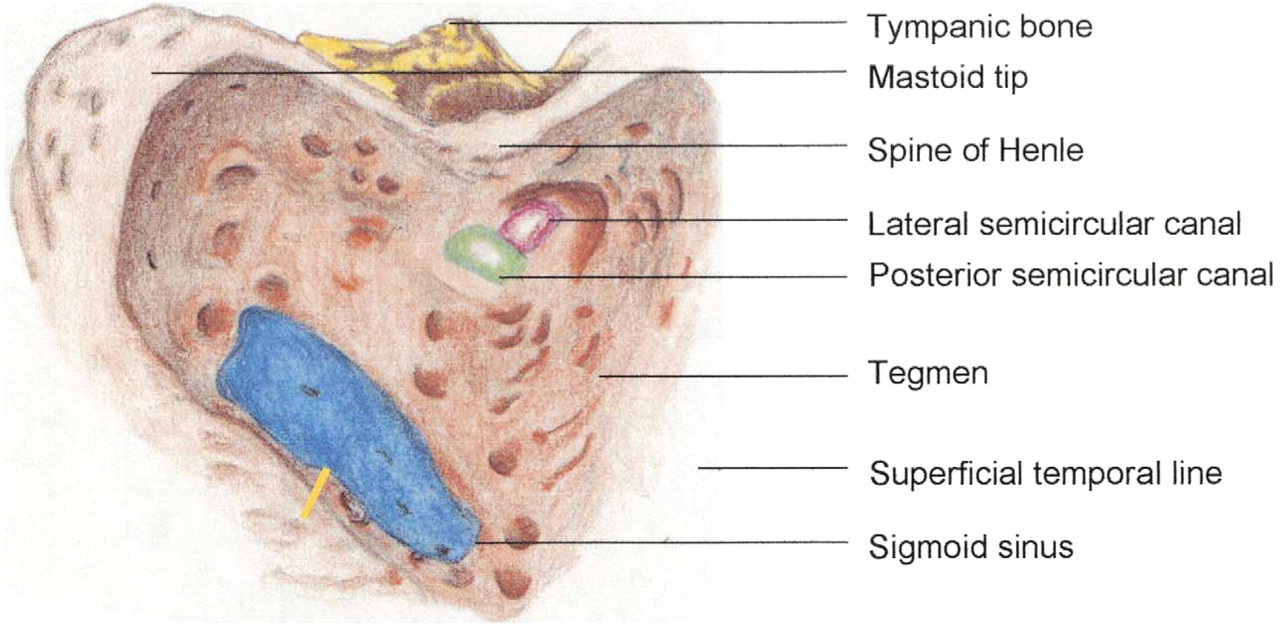
Variable N3 (yellow line).
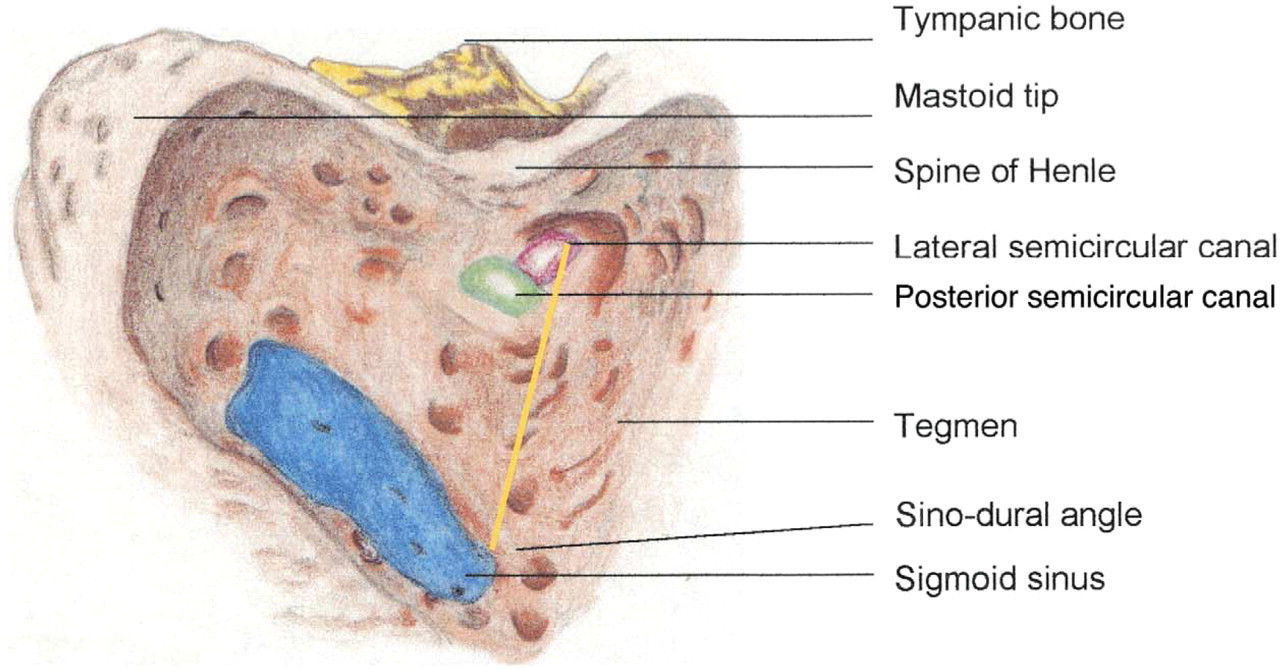
Variable N4 (yellow line).
Because the location of the SS is highly variable, its relationship with other surgical landmarks is also variable, as can be seen for the NAR of variables N3-N7. However, the sigmoid sinus is the only constant structure in the mastoid that is not subject to modification by pathological processes. Understanding the possible anatomic variations of the SS can be extremely useful for an experienced surgeon. For example, in our experience in cases of osteomas and cholesteatomas that have destroyed traditional landmarks such as the posterior auditory canal wall or the semicircular canals, using the SS as a landmark has been of great assistance in preventing otologic complications.
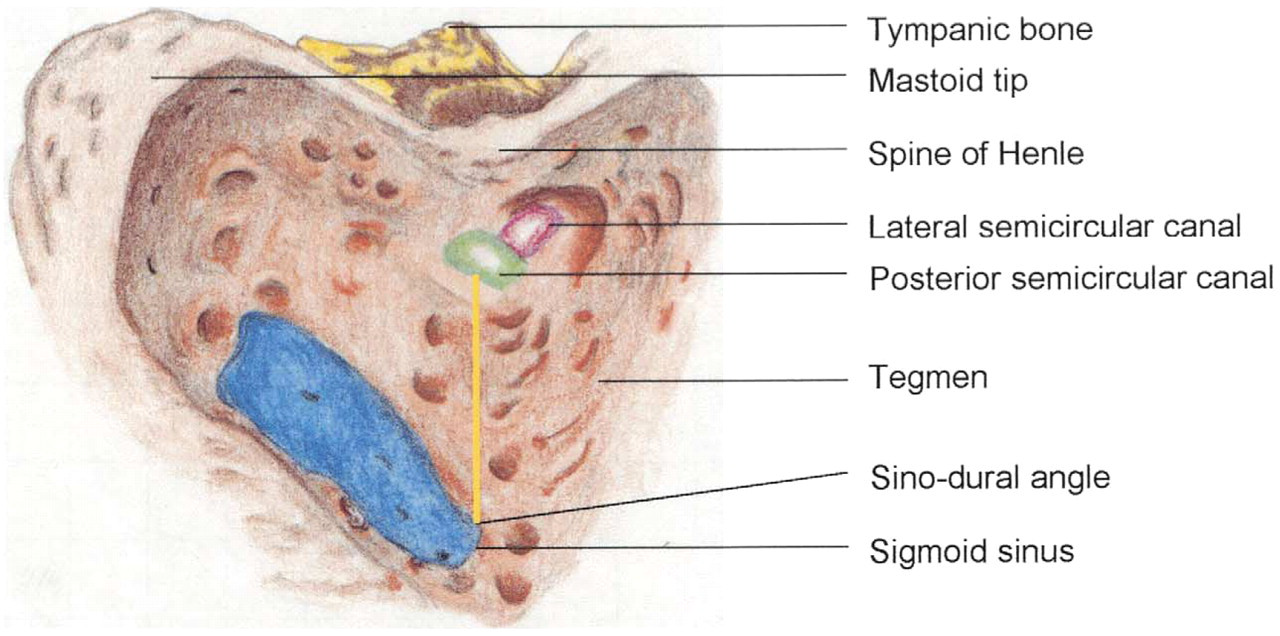
Variable N5 (yellow line).
Variable N5 (yellow line).
CONCLUSION
This surgical classification of variations in the anatomy of the sigmoid sinus has demonstrated significant anatomic variations in the area of Trautmann's triangle (types 1 and 3). The detailed anatomic information provided by this will be helpful to avoid inadvertent trauma to the sigmoid sinus and to use the SS as a landmark in cases were the mastoid anatomy is altered by pathological processes. 3,5,7,8
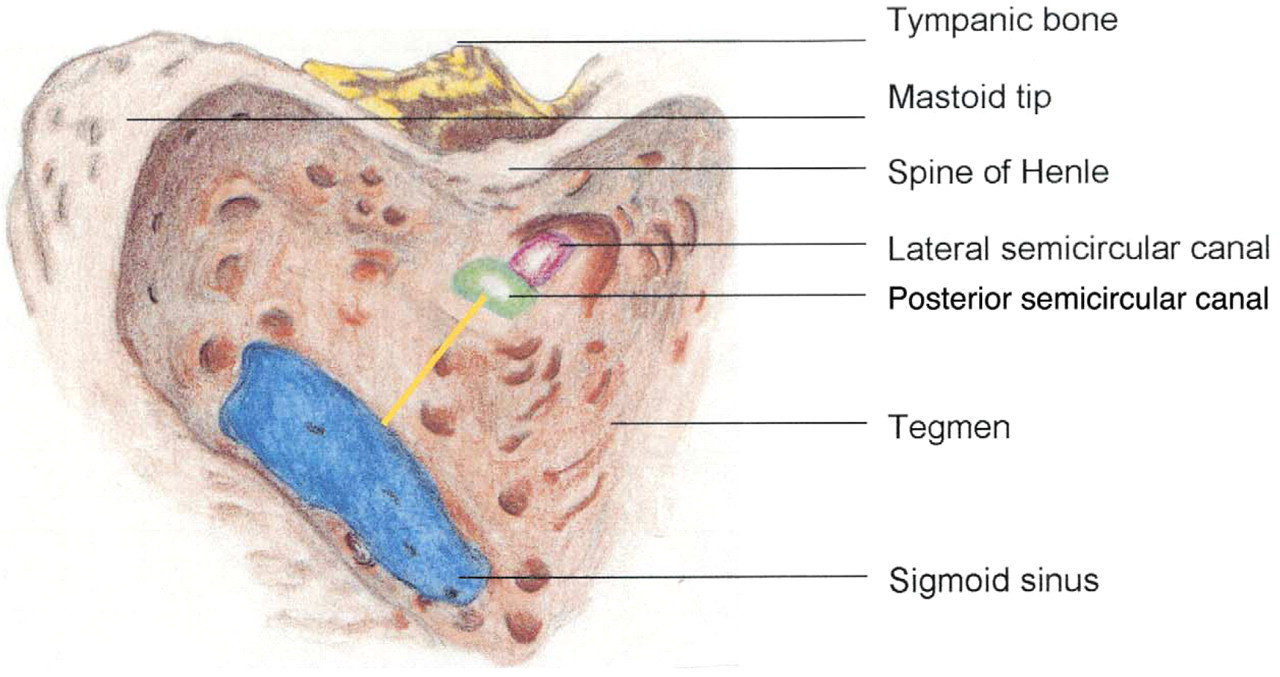
Variable N7 (yellow line).
Classification of the position of the sigmoid sinus and anatomic relationships

N, variable; P, percentile.
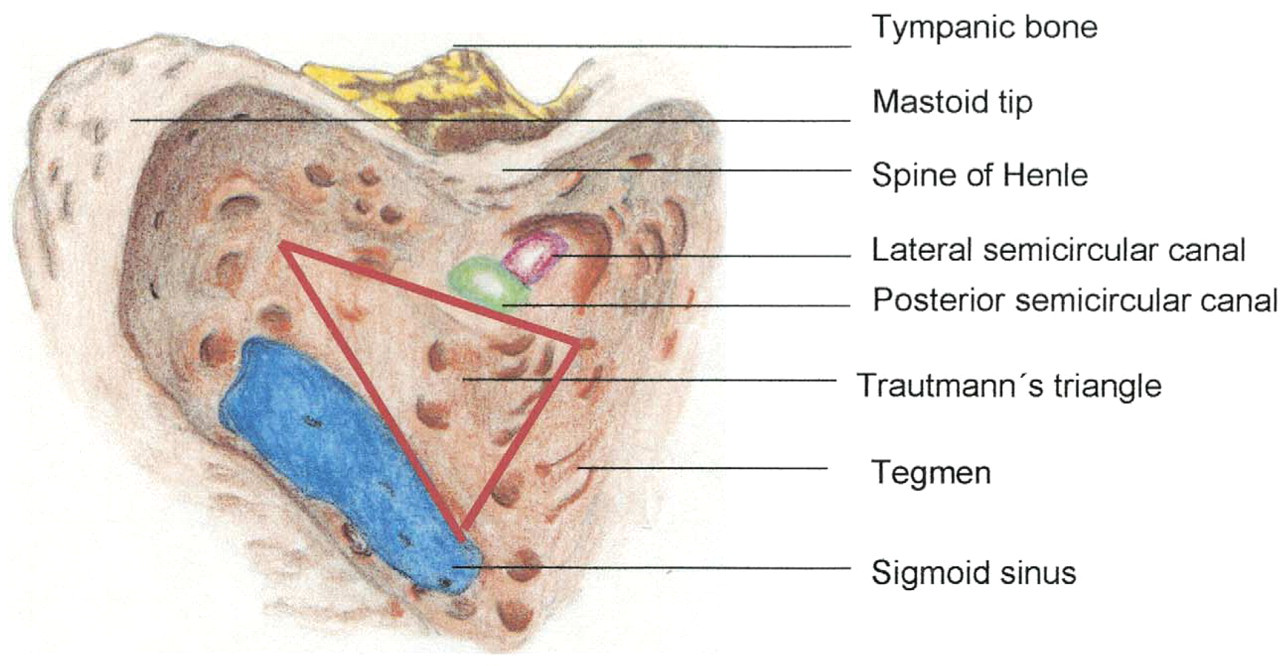
Sigmoid sinus type 1, posteriorly displaced (large Trautmann's triangle).
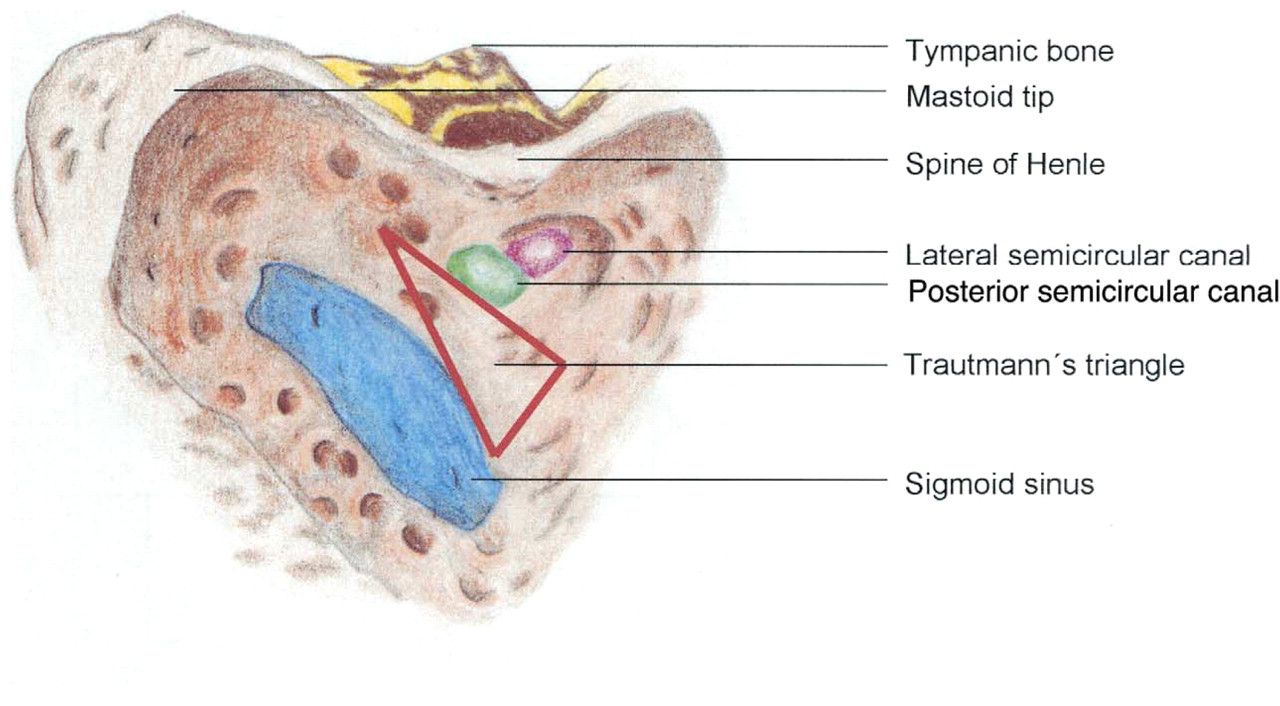
Sigmoid sinus (type 2, anteriorly displaced (right Trautmann's triangle).
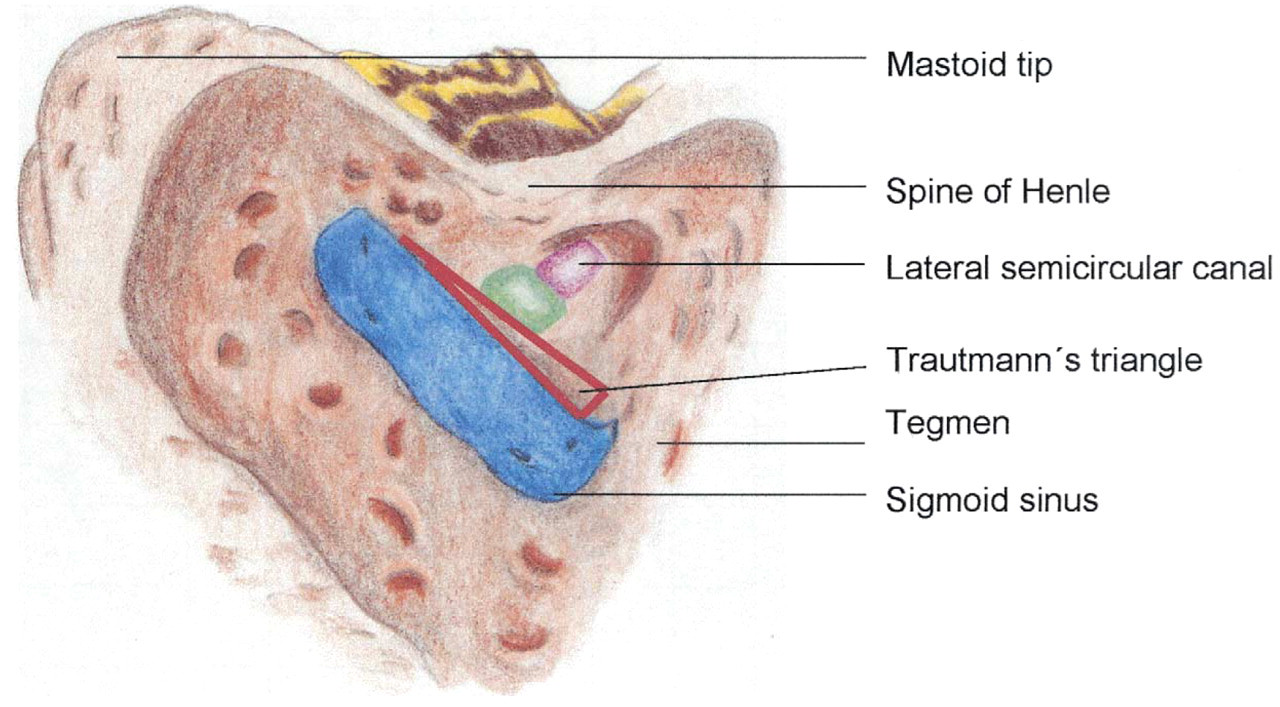
Sigmoid sinus type 3, medially displaced (Trautmann's triangle heavily tightened).
We thank Dr. Joseph Nadol, professor and chairman of the Harvard Medical School, MEEI, Department of Otolaryngology for his outstanding contribution editing this manuscript.