
Abstract
The lymphoid follicles at the base of the tongue can be detected when examining the pharynx of adults, but the presence of large follicles, denoted “severe” hypertrophy of the base of the tongue (HBT) is rare. The objective of the present study was to identify severe HBT cases and their symptoms and to correlate them with the presence of pharyngolaryngeal signs and esophageal symptoms of gastroesophageal reflux (GER) in patients seen at a laryngology clinic. Severe HBT was considered to be present when the follicles prevented the view of the epiglottis or were massively distributed through the pharynx and larynx. Five cases of severe HBT were detected among 306 patients submitted to videolaryngoscopy over a period of 2 years, corresponding to 1.6% (5/306) of the total sample studied. However, this index markedly increases to 4% (4/101) among patients with pharyngolaryngeal signs of GER and reached 7.5% (4/53) among patients presenting GER symptoms such as heartburn, regurgitation, retrosternal burning feeling, and dysphagia. The complaints due to severe HBT were noisy respiration, hoarseness, throat clearing, dry cough, globus pharyngeus, and nasal voice. We conclude that the frequency of hypertrophied follicles is increased in the presence of signs and symptoms of GER and those HBT symptoms are confused with those of GER, except for nasal voice and noisy respiration.
The lingual tonsils, which are part of the immunological barrier, are structures on each side of the tongue covered with squamous epithelium immersed in the lymphoid tissue of their crypts. The crypts are constantly washed by secretions of the mucosal glands, an action that prevents the deposition of food particles and even of microorganisms, thus reducing the risk of infection. As is also the case for the palatine tonsils, some lymphoid nodules with diffuse lymphoid cells and perifollicular germinal centers exist in the lingual tonsils. These centers harbor B lymphocytes responsible for the cognitive and effector functions of the humoral immune system. The immunological response is normally activated when an antigen or a substance with antigenic ability penetrates the squamous epithelium of the crypt close to the germinative centers of perifollicular tissue. This is the site where antigen recognition occurs and specific B lymphocytes are activated to perform their immunological function. 2
In daily clinical practice, some adult individuals are found to have hypertrophy of the lymphoid nodules at the base of the tongue with no apparent cause. According to Dundar et al, 3 this fact was observed by Vesalius as far back as in 1543. It is known that lymphoid tissue is increased in size at birth, gradually decreasing with age. Zharikova 4 and Kamata 5 observed that the lingual tonsils acquire functional activity later than the remaining lymphoid follicles, i.e., during the first or second decade of life, and reach greater immunological activity during the fourth and fifth decades. The literature has reported that these hypertrophies may be responsible for important symptoms and may even endanger life. Cases of sleep apnea, globus sensation in the throat and respiratory difficulties have been reported to be caused by HBT. 6,7
The objective of the present study was to identify cases of “severe” HBT in adults as well as the symptoms of this condition and to correlate the latter with the presence of pharyngolaryngeal signs and GER symptoms.
MATERIALS AND METHODS
The sample consisted of 306 consecutive patients submitted to videolaryngoscopy as a result of various indications, over a period of 2 years. The procedure was performed in the laryngoscope service of a University hospital using a 70° Hopkins lens, with the patient sitting and with the tongue projected outside the mouth. During videolaryngoscopy, the lymphoid follicles at the base of the tongue were observed and classified and patients with severe HBT were identified. Patients were considered to have severe HBT when these follicles prevented the view of the epiglottis and when they were disseminated through the pharynx and larynx (Fig 1). In the latter situation, the view of the vallecula was decreased and lymphoid follicles would have to be present inside the larynx. Five such patients were identified and became the subjects of this study.

Hypertrophy of the base of the tongue before surgery.
Pharyngolaryngeal signs of reflux were identified by videolaryngoscopy and the presence of GER symptoms was identified on the basis of clinical history. Interary-tenoid thickening, edema, and hyperemia of the posterior commissure of the larynx were considered to be pharyngolaryngeal signs of GER, and heartburn, regurgitation, retrosternal burning feeling, and dysphagia were considered to be symptoms of GER.
Surgical treatment consisted of removal of the follicles responsible for the symptoms using a punch and a laser beam (Fig 2). Data were analyzed statistically by Fisher exact tests on a 0.05 base.

Hypertrophy of the base of the tongue after surgery.
RESULTS
The study population included 101 patients with pharyngolaryngeal signs of reflux (posterior laryngitis) and 53 with typical complaints of GER at the esophageal level. Among the 306 cases studied, 123 were found to have HBT, with 5 of them (1.6%) having severe HBT. “Severe” HBT was present in 4% (4/101) of the patients with pharyngolaryngeal signs of GER and in 7.5% (4/53) of the patients with symptoms of GER (statistically significant, P = 0.0423 and 0.0036, respectively).
All patients with severe HBT were females, and were an average of 45.6 years of age (range, 22 to 59 years). Of the 5 patients, 4 were smokers (20 to 30 cigarettes a day) and 1 had been submitted to adenotonsillectomy during childhood.
The complaints reported by these patients were hoarseness, throat clearing, globus pharyngeus, nasal voice, noisy respiration, and dry cough. The symptoms did not disappear or decrease in 3 of the 5 patients submitted to treatment with prokinetic agents and an H2 antagonist. Four of the 5 patients presented posterior laryngitis and were submitted to esophagoscopy, and 2 showed an inflammatory process in an esophageal biopsy. Of the 5 patients, 4 presented associated diseases such as hiatus hernia (2), rheumatoid arthritis (2), arterial hypertension (2), ulcers (2; duodenal in 1 case and gastric in the other), diabetes mellitus (1), diffuse goiter (1), intestinal diverticulum (1), obesity (1), sinusitis (1), and subglottic stenosis (1) (Table 1).
Patients complaints, treatment, and results
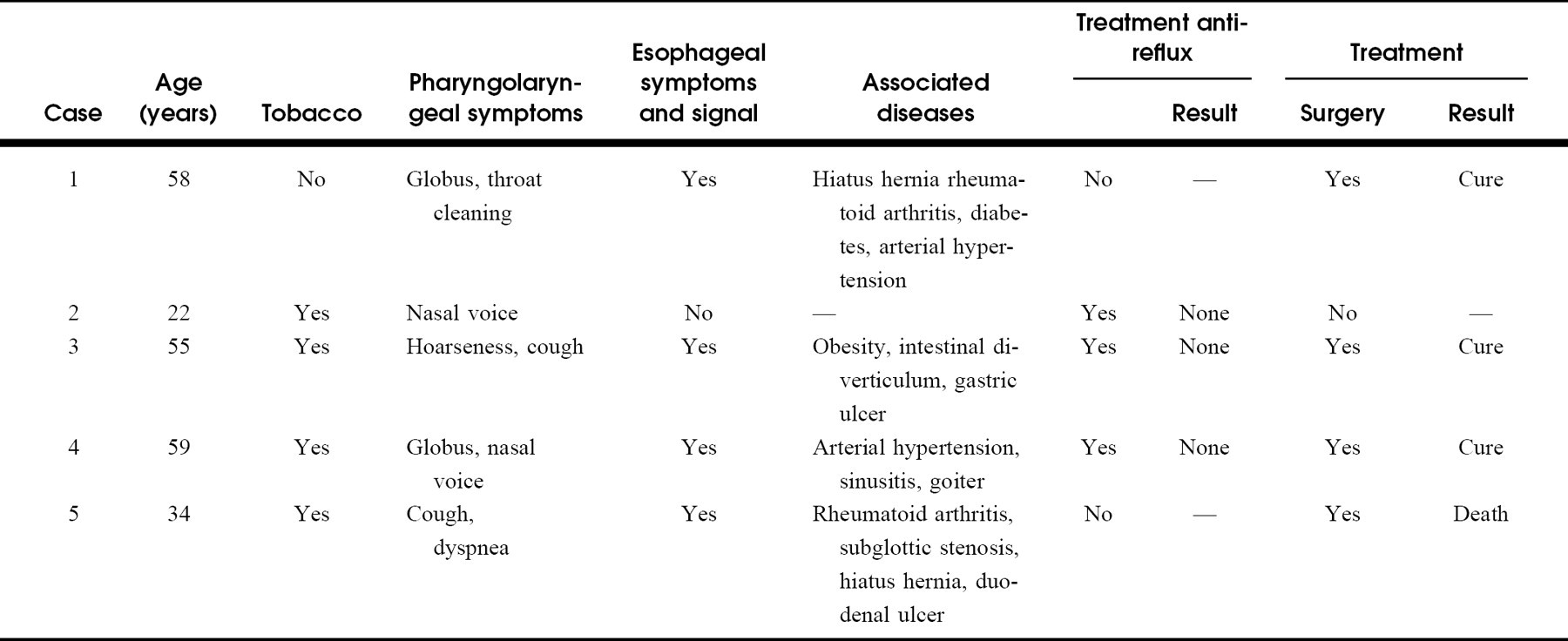
Four of the patients with severe HBT agreed to endoscopic resection of the lymphoid follicles with a punch until the view of the vallecula and a laser beam. One patient died during anesthesia induction, 2 were submitted to follicle removal from the base of the tongue, and the fourth was submitted to follicle removal from the inside of the larynx only. After surgery, all symptoms disappeared over a follow-up of more than 2 years. The patient who died presented follicles inside the larynx and subglottic stenosis.
DISCUSSION
It is known that among adults and older persons free from inflammatory processes there is a reduced activity of immunoglobulin production 8 and that in these situations the lymphoid follicles practically disappear from the pharynx. Thus, the Waldeyer ring, consisting of lymphoid tissue in the rhinopharynx and oropharynx, is exuberant at birth and tends to disappear among the elderly. However, there are situations in which the lymphoid follicles at the base of the tongue become hypertrophied for no apparent reason, forming saliencies in the oropharynx and possibly causing unpleasant symptoms or even pose a risk to the life of these patients. Exuberant lymphoid tissue, when present at the base of the tongue, appears as a surface with rounded saliencies of pink-white color of ill-defined contours, which tends to prevent the view of the vallecula and at times even of the epiglottis.
According to Schantz et al, 9 Joseph et al, 10 and Elia, 11 HBT is frequently caused by compensatory lymphoid follicle hyperplasia occurring after adenotonsillectomy. In the present study, however, only one of the patients with severe HBT had been submitted to adenotonsillectomy in childhood. Joseph et al 10 also pointed out the possibility that HBT is due to allergic processes, chronic infections or the use of alcohol and tobacco. It may be that tobacco smoking is an important causative factor of HBT because four of our patients were intensive smokers.
In the present study, patients with severe HBT with follicles preventing a view of the epiglottis complained of throat clearing, globus pharyngeus, nasal voice, noisy respiration, and dry cough, whereas patients with HBT whose follicles prevented a view of the vallecula presented no symptoms unless they had lymphoid follicles inside the larynx, when hoarseness was the most important manifestation. The nasal voice and noisy respiration can be explained by narrowing of the air column caused by HBT, causing air strangulation and shifting air to the nose. Throat clearing and a dry cough are a result of the presence or attrition of follicles inside the larynx. 12 The globus pharyngeus in this disease is a sensation of discomfort, aching or swelling in the oropharynx, or of a fishbone or a ball stuck in the throat. According to Olson, 13 it is not clear whether globus pharyngeus is a result of neuromuscular dysfunction, acid reflux, or tissue growth. This sensation in HBT cases is probably because of the follicles touching the posterior wall of the pharynx. The sensation is increased during fluid swallowing and may disappear for a few moments when solid food is swallowed, causing these patients to eat all the time and to become obese.
Another symptom reported to be linked to HBT is sleep apnea, although this relationship is rare, especially among adult patients, because the oldest patient cited in the literature as having sleep apnea as a result of HBT was only 13 years old. 14
Upon palpation, bulging of increasing consistency is felt at the base of the tongue of patients with HBT, although without localized or generalized hardening. Exuberant lymphoid tissue at the base of the tongue should be differentiated from ectopic thyroid, carcinomas, sarcomas, infectious pharyngitis, and benign tumors (adenomas, cysts, papillomas, and salivary gland tumors).
Some of the symptoms cited earlier are also usually attributed to patients with GER, such as dry cough, hoarseness, throat clearing, and globus pharyngeus, so that the true etiology is impossible to identify in patients with HBT and GER. The surgical treatment of these patients consists of removal of the lymphoid follicles responsible for the symptom, i.e., those at the base of the tongue (nasal voice, globus pharyngeus) and those of the larynx (hoarseness).
In the present study, severe HBT was more frequent in patients with GER symptoms. Previously reported data have shown a high frequency of lymphoid tissue in patients with signs of GER (62.4%), indicating that the presence of gastric juice in the pharyngolaryngeal region may be important in the etiology of HBT. 15 Despite this relationship, the severe HBT present in 1.6% of our patients did not regress with the antireflux treatment used (prokinetics and H2 inhibitors), leading us to agree with Chodosh 16 when he states that HBT may be the cause, rather than an effect, of GER. According to Chodosh, GER is provoked by the presence of air in the stomach due to the aerophagia caused by HBT. However, on the basis of this theory, all patients with reflux should have HBT, which is not what actually occurs. We believe that a patient with HBT due to the presence of pharyngogastric reflux for many years may not respond to antireflux agents applied for a short period of time. Furthermore, today we know that the antireflux agents used for the present patients are not those most indicated for cases of reflux with repercussions at the pharynx-larynx level. 17,18
According to the data observed in the present study, both HBT and GER can produce the sensation of globus pharyngeus, suggesting that patients with this symptom should be examined for the presence of both HBT and GER. In the presence of GER symptoms, especially pharyngolaryngeal symptoms, or of clinically suspected severe HBT, it is imperative to perform videolaryngoscopy. This is particularly important for patients who must be intubated and submitted to general anesthesia because the presence of hypertrophied tissue at the base of the tongue or of lymphoid tissue inside the larynx may cause difficulties in locating the larynx during intubation, with life-endangering consequences for the patient, as observed in 1 of our cases.
Finally, the present findings open the possibility for future investigations about the etiology and aggressiveness of cancer of the base of the tongue. Cachin, 19 in 1989, first attempted to correlate cancers of the base of the tongue with the presence of lymphoid follicles, but in 1995, Mamede et al 20 described the characteristics of the carcinomas that develop on lymphoid tissues and stated that they differ from those at the base of the tongue but with the absence of lymphoid tissue by being more undifferentiated, of faster growth, and of fulminating course. In view of these observations, we may ask whether these characteristics are a result of the fact that the tumor originated close to the lymphoid follicles or was influenced by GER.
CONCLUSIONS
On the basis of the present data, we conclude that (1) severe HBT was present in 1.6% of the patients submitted to videolaryngoscopy, with its frequency increasing in the presence of signs and symptoms of GER (statistically significant) and (2) the symptoms of severe HBT were throat clearing, globus pharyngeus, dry cough, and hoarseness that are confused with those of GER, and nasal voice and noisy respiration.