
Abstract
OBJECTIVE: To compare the quality-of-life (QOL) benefit received from cochlear implants (CIs) and hearing aids (HAs) among hearing-impaired adults.
STUDY DESIGN: Health-related questionnaire.
METHODS: Twenty-seven CI users compared to control group of 54 HA users, both older than 49. Questionnaires for the pre-rehab state (without HA or CI use) and post-rehab state (after HA or CI for 12 months) were mailed 2 weeks apart.
RESULTS: Twenty-six (96.3%) CI and 30 (55.6%) HA users responded (P < 0.001, chi-square). Compared to HA patients, CI users showed twice as much overall QOL improvement (P = 0.082, multiple linear regression) as HA users. Multivariate analysis of variance showed greater QOL benefit in CI than HA users across the physical, psychological, and social subdomains (P = 0.03).
CONCLUSION: Cochlear implants provide at least comparable benefit for those with profound hearing loss as hearing aids bring for those with less severe hearing loss.
Auditory rehabilitation can reverse the adverse affects of and dysfunction from hearing loss. Hearing aids can improve the overall quality of life (QOL) in hearing-impaired adults. 7,8 For patients who receive no benefit from hearing aids (HAs), cochlear implants (CIs) provide improved audiologic performance and improvements in QOL. 9–11
This study compares the functioning, with respect to QOL, of CI patients with an average group of HA patients. By evaluating the QOL benefit from CIs with that of HAs in hearing-impaired adults, the impact of auditory intervention on the functional gap between CI and HA candidates is assessed. Specifically, the degree that CIs raise deaf patients' QOL toward levels enjoyed by HA patients can be determined. Such an analysis may bring further insight about how each intervention impacts patients' lives.
MATERIALS AND METHODS
Approval for the study was obtained from the Institutional Review Board. Thirty-three cochlear implant (CI) patients who were implanted at age 50 or older and had their implant for a minimum of 12 months were identified. Patients who did not have a current mailing address were excluded, leaving 27 CI patients in the experimental group. From the same audiology clinic, a random sample of 65 HA patients who began using aids at age 50 or older, had bilateral hearing loss, and had used aids for at least 12 months were selected. Patients without current mailing addresses were excluded, leaving 49 HA patients in the control group.
Demographic, medical, and audiological data were collected from patient records. The number of chronic medical problems, current age, age at intervention (first hearing aid use or cochlear implantation), length of hearing loss, time since intervention, race, and marital status were collected for each person. Education was obtained on survey responders and defined as less than or equal to high school or greater than high school. For CI users, sentence recognition scores with and without lip reading (Central Institute for the Deaf, CID, or Hearing in Noise Test, HINT, for patients not receiving CID sentences) and length of deafness prior to implantation were obtained. For HA users, the number and type of HAs used, speech discrimination score in the better ear, and pure tone average at 500, 1000, and 2000 Hz in the better ear were also recorded.
Sensitivity analysis of responders and nonresponders∗
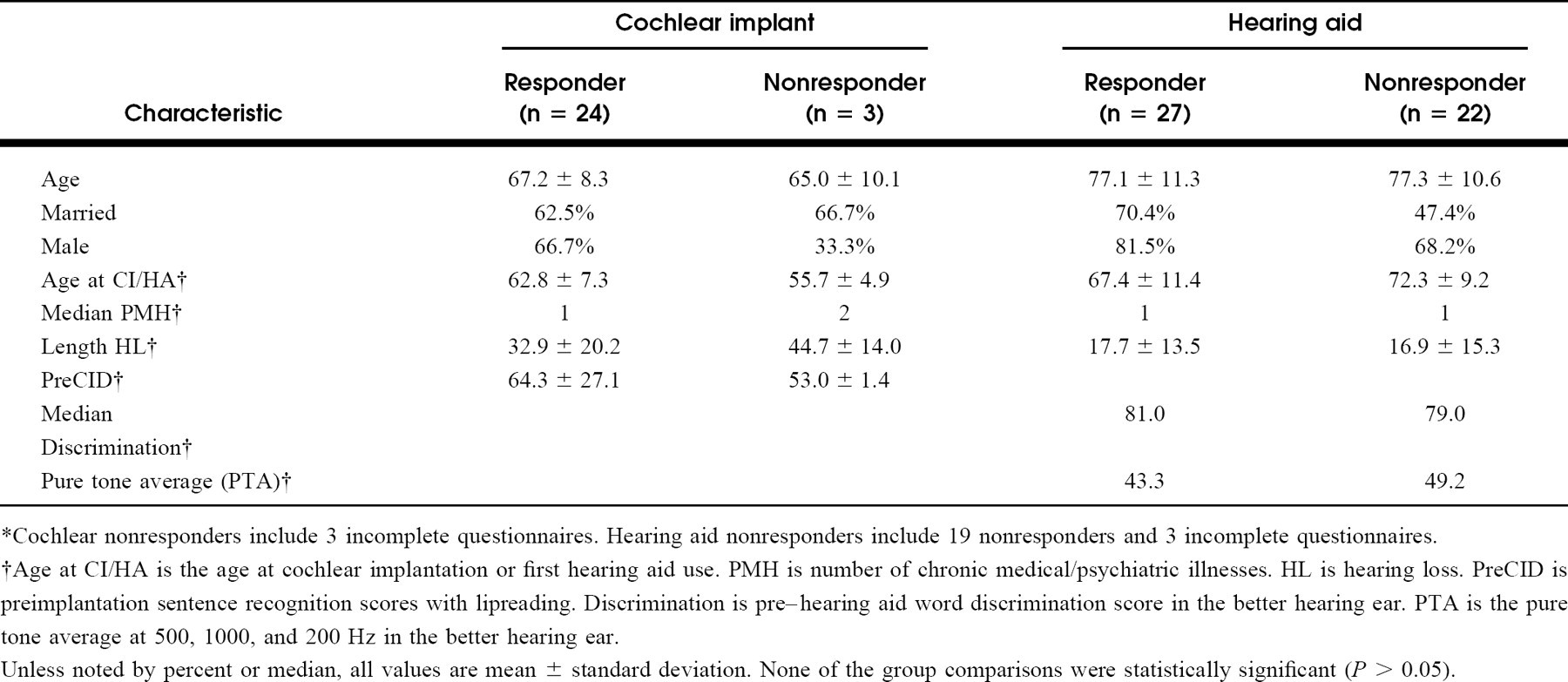
Cochlear nonresponders include 3 incomplete questionnaires. Hearing aid nonresponders include 19 nonresponders and 3 incomplete questionnaires.
Age at CI/HA is the age at cochlear implantation or first hearing aid use. PMH is number of chronic medical/psychiatric illnesses. HL is hearing loss. PreCID is preimplantation sentence recognition scores with lipreading. Discrimination is pre–hearing aid word discrimination score in the better hearing ear. PTA is the pure tone average at 500, 1000, and 200 Hz in the better hearing ear.
Unless noted by percent or median, all values are mean ± standard deviation. None of the group comparisons were statistically significant (P > 0.05).
To assess QOL, the Nijmegen Cochlear Implant Questionnaire, a health-related QOL questionnaire recently designed and validated, was used. 12,13 This questionnaire is composed of 6 subdomains: basic sound perception, advanced sound perception, and speech production comprise the physical domain; self-esteem is the psychological domain; activity limitations and social interactions encompass the social domain. 12 Both CI and HA patients were separately mailed 2 copies of the questionnaire. The first version was for the pre-rehab state (ie, without the CI or HA) and the second version for the post-rehab state (ie, with the CI or HA). They were mailed at least 2 weeks apart and were returned anonymously. Follow-up phone calls were made to ensure receipt of the questionnaire.
The questionnaire was scored as described by Hinderink et al. 12 Questions phrased in a negative format were recoded to allow scoring similar to the positive questions. Responses were scored as 0, 25, 50, 75, 100, and the response “not applicable” and unanswered questions were treated as missing values. Questionnaires with more than 3 missing values in a subdomain were excluded from analysis. Subdomain scores were obtained by adding the score for each question and dividing the sum by the number of specific subdomain questions completed. Total QOL scores were calculated by adding the score of each question and dividing the sum by the total number of questions completed. The difference between the post-rehab and pre-rehab state served as the benefit score.
Statistical analysis was performed with SigmaStat and SPSS software (SPSS Inc., Chicago, IL, USA). Repeated-measure analysis of variance was used to determine if group (CI vs HA), time of evaluation (pre- vs post-intervention), or interaction between group and time were associated with QOL benefit. Subsequent analysis of QOL benefit and potential confounding variables was performed. If the assumptions of normality were not met, tests were conducted using nonparametric tests. Multiple linear regression assessed the association between QOL benefit and group while adjusting for identified confounding variables. To control for multiple tests, analysis of the 6 QOL subdomain benefit scores was conducted using multivariate analysis of variance and covariance of group differences (CI vs HA). Given a statistically significant multivariate finding, subsequent analysis of covariance procedures were conducted on each QOL subdomain benefit score while adjusting for confounding variables.
RESULTS
One hundred percent of the CI users (27/27) and 30 of the 49 HA users (61.2%) returned both questionnaires (P ≤ 0.001, chi-square). Three CI and 3 HA users had incomplete questionnaires, leaving 24 CI and 27 HA users available for analysis. No statistically significant differences were noted in the CI users with incomplete questionnaires and CI users with complete surveys (Table 1). Likewise, no statistically significant differences in demographic and audiologic variables were seen between the HA users not in the analysis (3 with incomplete questionnaires and 19 nonresponders) and HA users returning complete surveys (Table 1). All CI patients were post-lingually deafened.
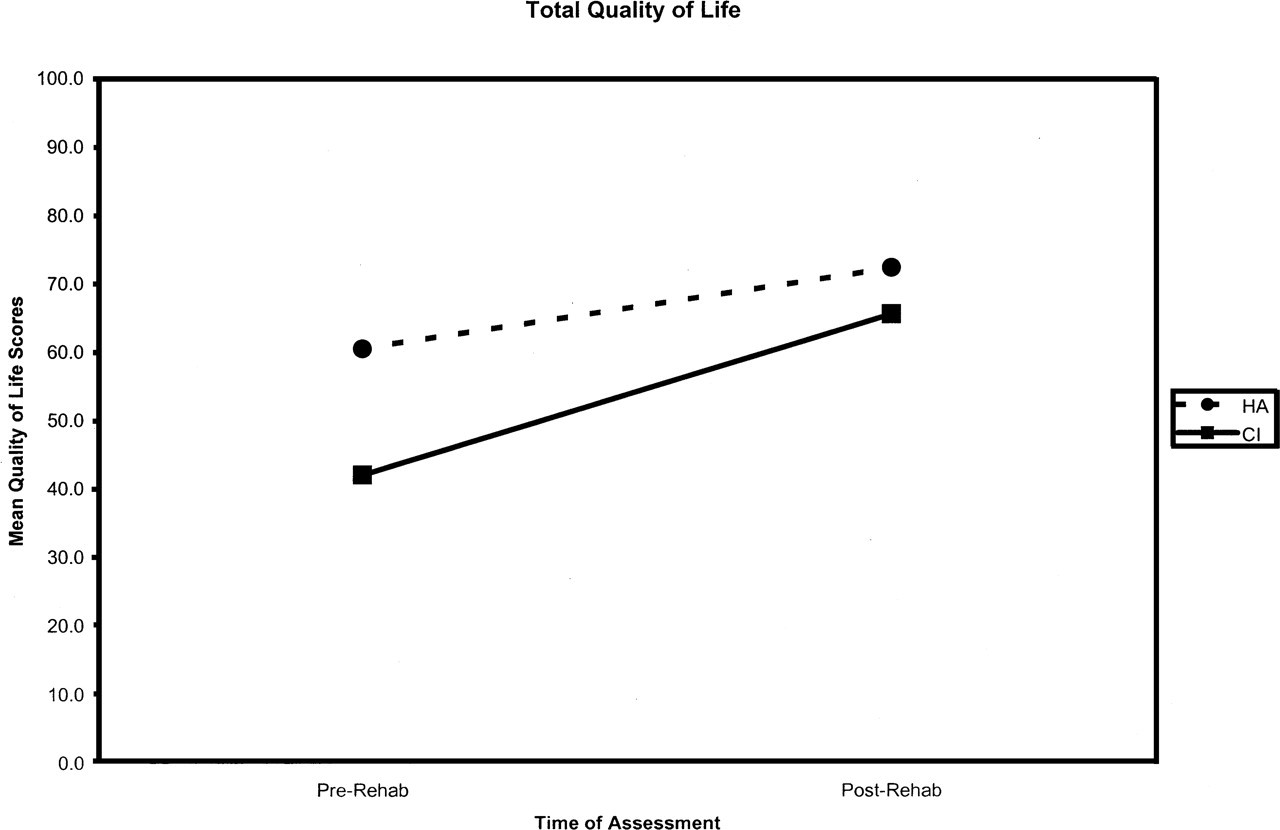
Change in total quality-of-life scores for cochlear implant vs hearing aid patients.
Descriptive statistics for quality of life (QOL) benefit scores by study group
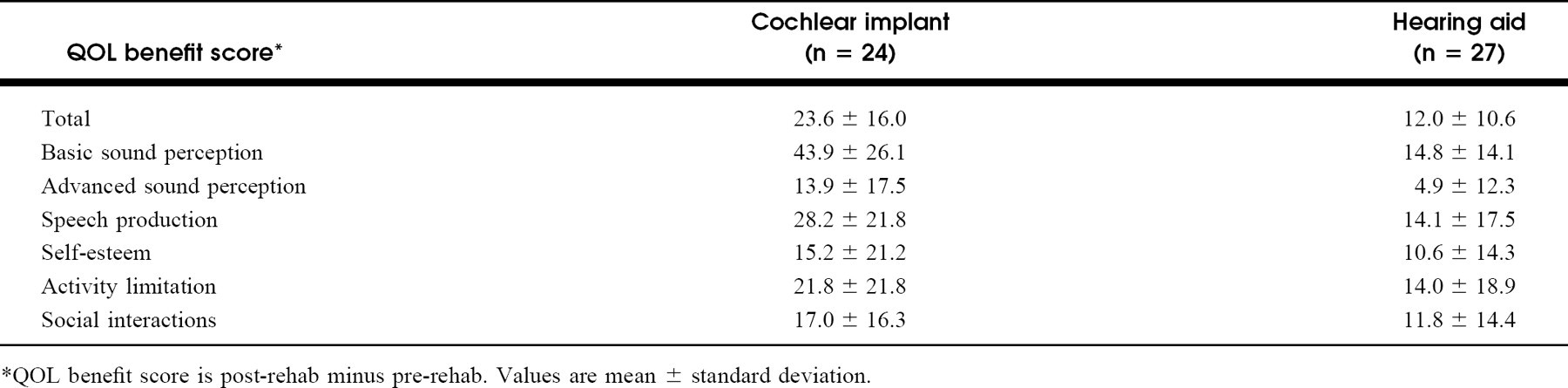
QOL benefit score is post-rehab minus pre-rehab. Values are mean ± standard deviation.
Among HA users, the mean length of HA use was 120.6 months, range: 12 to 360 months; among the CI patients, the mean length of implant use was 53 months, range: 12 to 156 months, (P = 0.003, t test). In the HA patients, the median speech discrimination score in the better ear was 81.0%, and median PTA in the better ear was 43.3. The mean sound-only sentence recognition scores for the CI patients was 5.4% ± 10.4%. All HA patients had bilateral hearing loss, and 85.2% had binaural auditory input with bilateral HAs. The CI patients all had bilateral hearing loss, but only 14.3% had binaural auditory input with one CI and contralateral HA (P ≤ 0.001, chi-square).
Relationships were seen between objective audiologic studies and the QOL measure. Within the HA patients, those with lower pre-rehab speech discrimination scores had lower pre-rehab QOL scores (r = 0.41, P = 0.05, Spearman correlation). In the CI group, mean sound-only sentence recognition scores increased from 5.4% ± 10.4% to 65.7% ± 33.1% (t = 7.13, P ≤ 0.001, paired t test). Improvements in overall QOL scores correlated with increases in sound-only sentence recognition scores (r = 0.56, P = 0.03, Spearman correlation).
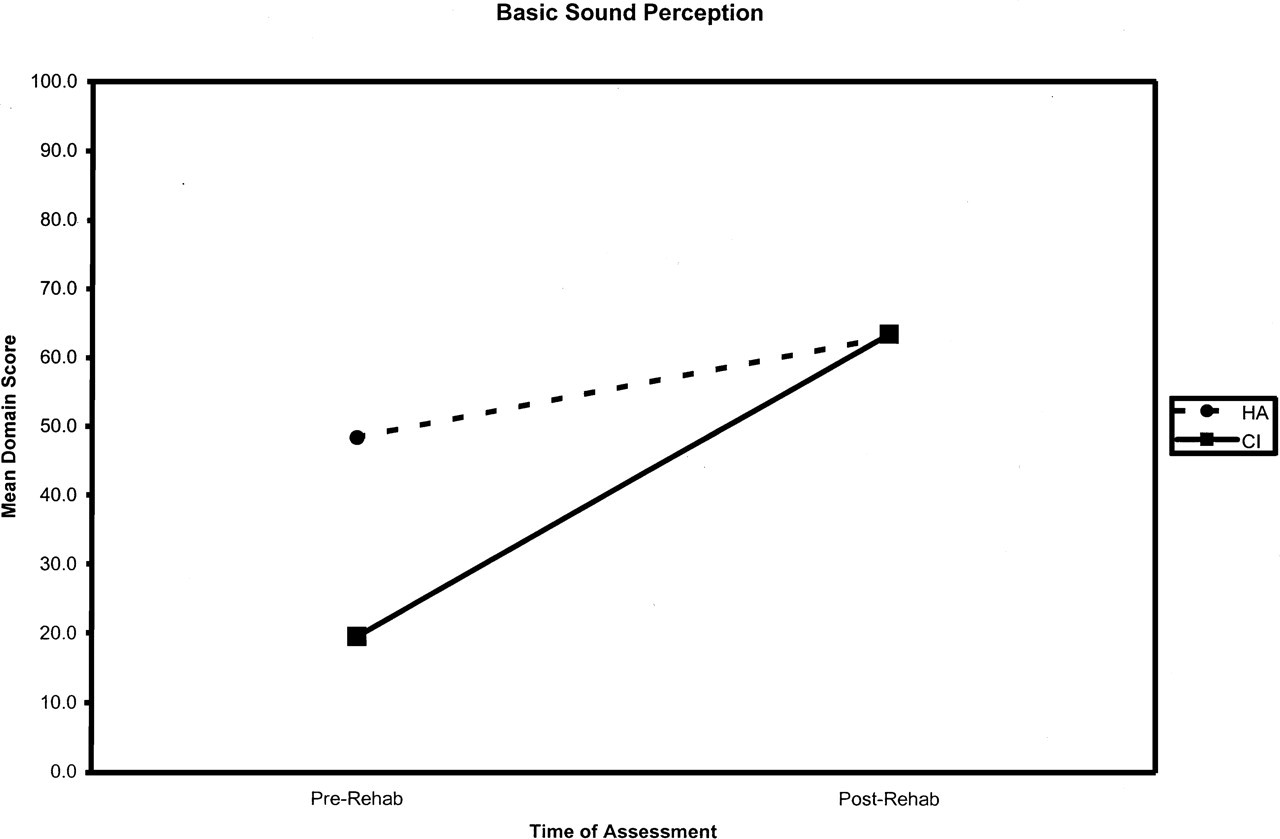
Change in basic sound perception quality-of-life scores for cochlear implant vs hearing aid patients.
Multiple linear regression
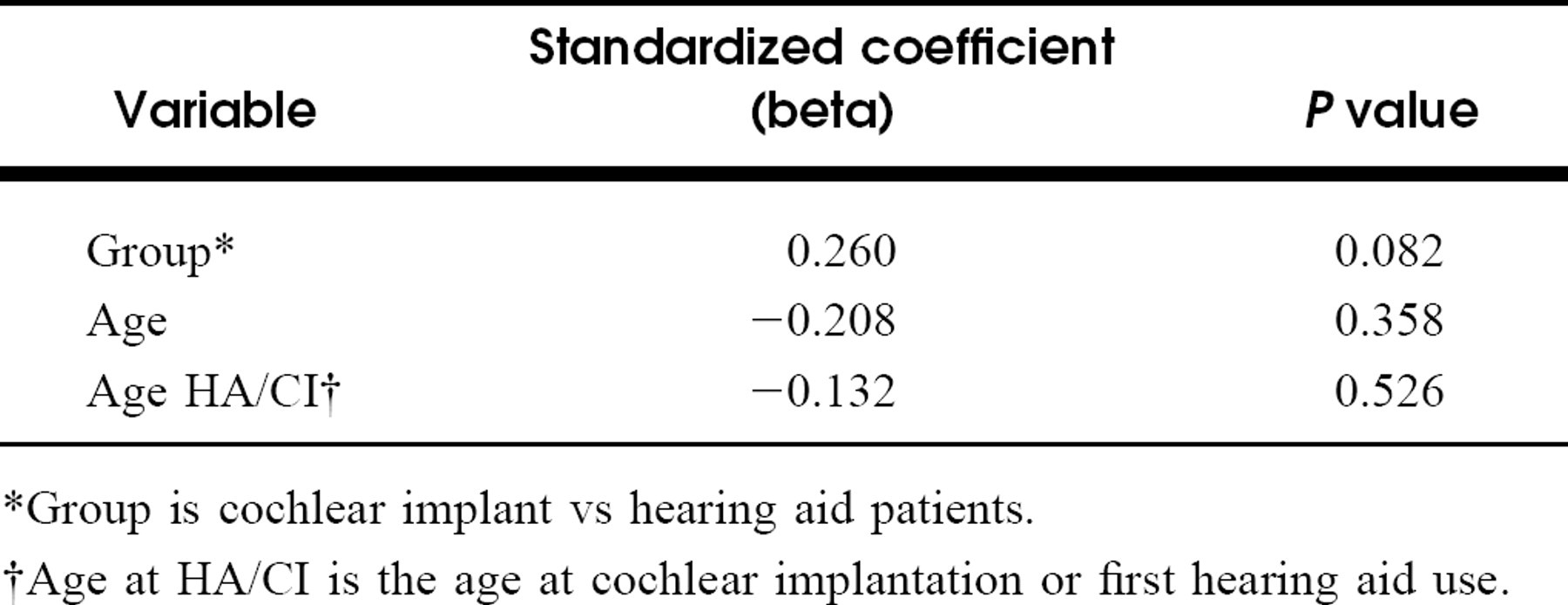
Group is cochlear implant vs hearing aid patients.
Age at HA/CI is the age at cochlear implantation or first hearing aid use.
Both HA and CI patients received benefit from their particular auditory intervention (Fig 1). Across both groups, the total postintervention QOL scores were greater than the total preintervention QOL scores (F = 89.8, P ≤ 0.001, 2-way repeated-measure ANOVA). While HA patients had higher QOL scores than CI users, CI patients had twice as much improvement in their QOL scores (F = 9.6, P = 0.003, 2-way repeated-measure ANOVA) (Table 2).
Analysis of variables known to affect QOL independent of hearing impairment, race, sex, education, or marital status groups, revealed no statistically significant associations with QOL (P > 0.05, Mann-Whitney). No statistically significant associations were found between QOL benefit and length of hearing loss, time since intervention, or number of medical/psychiatric problems (P > 0.05, Spearman correlation). Among HA users, the type of hearing aid (P = 0.68, Kruskal-Wallis ANOVA) and number of hearing aids tried (r = −0.07, P = 0.72, Spearman correlation) was not related to QOL benefit. However, statistically significant inverse relationships across both groups were seen between QOL benefit score and age at intervention (r = −0.35, P = 0.01, Spearman correlation) and current age (r = −0.36, P = 0.01, Spearman correlation). Multicollinearity between current age and age at intervention was not found and both were included in the regression model. Multiple regression results showed a statistical trend (beta = 0.260, P = 0.082) for greater QOL benefit among the CI patients than among the group of HA users (Table 3).
Average QOL subdomain benefit scores for each patient group increased from the pre-rehab to post-rehab state (Table 2, Figs 2 through 7). Multivariate analysis of variance showed a statistically significant difference in the degree of improvement in QOL between the CI and HA users across the 6 subdomains (Wilks' lambda = 0.642, P = 0.002, effect size = 0.358). This multivariate statistically significant difference was retained after controlling for age and age at intervention (Wilks' lambda = 0.851, P = 0.030, effect size = 0.279). Post-hoc univariate analysis of the individual subdomains, adjusting for age and age at intervention, found a statistically significant difference in QOL benefit between CI and HA users in the basic sound perception subdomain (F(1,46) = 14.227, P < 0.001, effect size = 0.236) and trends of greater improvement in CI users for the other subdomains.
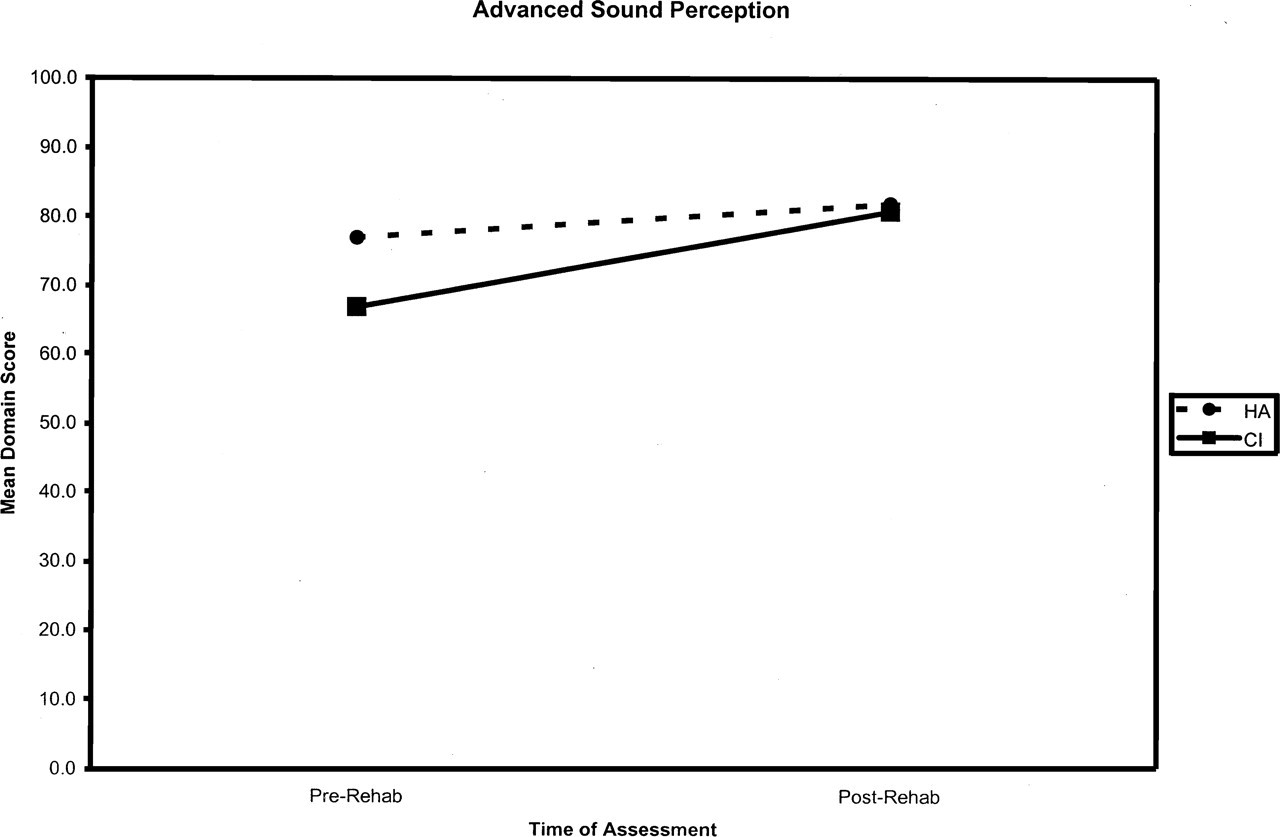
Change in advanced sound perception quality-of-life scores for cochlear implant vs hearing aid patients.
DISCUSSION
The number of elderly adults continues to increase. Consequently, more people will be afflicted with hearing loss. Identifying and treating the hearing impaired may ameliorate the adverse consequences of hearing loss. This study demonstrates that HAs and CIs can improve the overall QOL of hearing-impaired adults with a trend of greater benefit among the CI patients. Furthermore, the increase in at least 1 subdomain (basic sound perception) was significantly larger in CI users as compared to HA patients.
This study used a new health-related QOL questionnaire designed for use in CI users. The questionnaire has been previously tested and was found to be reliable, valid, and able to detect clinical changes and to have good internal consistency among CI users. 12,13 Our study also administered this questionnaire to HA patients. The questionnaire was able to detect changes in pre-rehab vs post-rehab QOL performance and correlated with objective audiologic measures in both the CI and HA users, supporting its use as a measurement tool in each group. Thus, the QOL benefit, in the physical, psychological, and social domains, from CIs and HAs could be measured. Future studies could compare this questionnaire with QOL tools specifically designed for HA patients.
Overall, our study further supports the previously identified association between QOL and hearing loss. Hearing impairment negatively impacts physical and social function, emotional state, and communication. 14,15 Additionally, patients with more significant hearing loss experience greater impairment in their QOL. Our HA patients with lower pre-rehab speech discrimination levels demonstrated reduced pre-rehab QOL scores (r = 0.41, P = 0.05, Spearman correlation). Similarly, Bess et al found that the degree of hearing loss correlated with patients' level of physical and psychosocial disability. 15 Furthermore, the finding that improved audiologic performance brings about positive changes in QOL is also supported by our study. Among the HA patients, improvements were seen in overall QOL and not only the physical subdomains but also in self-esteem and social functioning (Figs 1–7). Mulrow et al also found significant changes in social, emotional, and communication function. 7
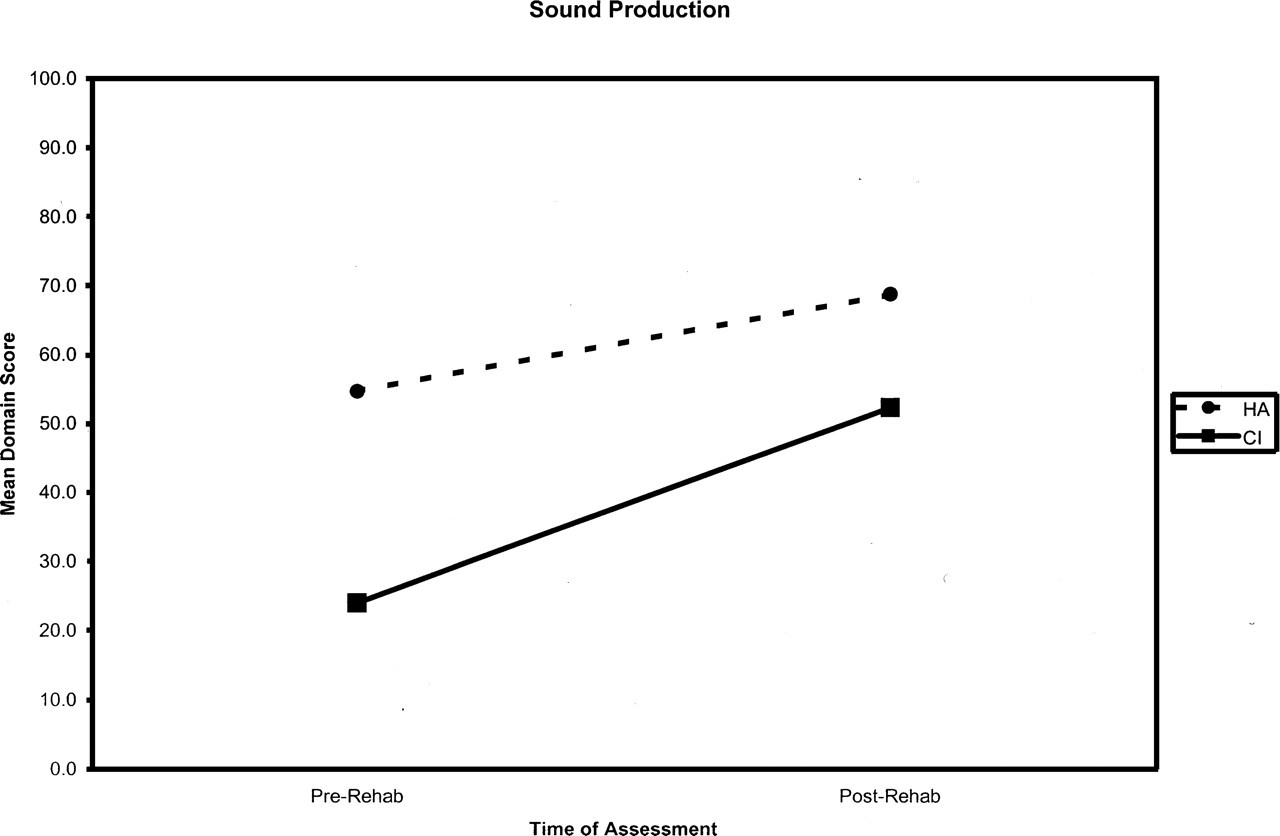
Change in sound production quality-of-life scores for cochlear implant vs hearing aid patients.
Similar to HAs, CIs also improve QOL among the hearing impaired. Like Hinderink et al, we found that CI users demonstrated increased overall QOL and benefits in all physical, psychological, and social subdomains (Figs 1–7). 12 Additionally, our QOL benefit was associated with improvements in objective sound-only sentence recognition scores (r = 0.56, P = 0.03, Spearman correlation). The more audiologic improvement patients had, the greater overall QOL benefit they realized. Wyatt et al also found better speech, hearing, and cognitive function and improved emotional state among adult CI users. 16 Other reports have found improved audiologic performance and enhanced QOL in elderly CI patients. 9–11 Furthermore, elderly patients implanted at younger ages have been shown to receive greater QOL benefit from their implant. 17,18 Thus, early identification of deaf adults may further enhance the benefit received from cochlear implants.
Cochlear implants provide exciting options for patients with profound hearing loss. Although the details of how the comparison was performed were not mentioned, Summerfield et al found that adult multichannel CI patients had larger increases in QOL compared to HA users. 19 In our study, after controlling for variables that affect QOL, a trend towards significance of twice as much overall QOL benefit in CI users vs HA patients occurred (Tables 2 and 3). Additionally, the benefit seen in the basic sound perception subdomain for CI patients was almost 3 times that of the HA users (F(1,46) = 14.227, P < 0.001, effect size = 0.236) with trends of greater improvement for CI than HA patients in the other subdomains (Figs 2–7).
Despite the severity of their hearing loss, CI patients obtained at least comparable benefit as patients with milder forms of hearing loss received from HAs. In particular, CIs narrowed the gap between elderly patients with profound hearing loss and HA patients with less severe hearing impairment with respect to overall QOL and across all subdomains (Figs 1–7). Although CI users more commonly had monaural auditory input, CI patients still approached the QOL levels of HA patients. Perhaps bilateral implantation would bring further improvements in QOL. Thus, CIs raised the physical, psychological, and social function of deaf patients closer to levels enjoyed by HA patients.
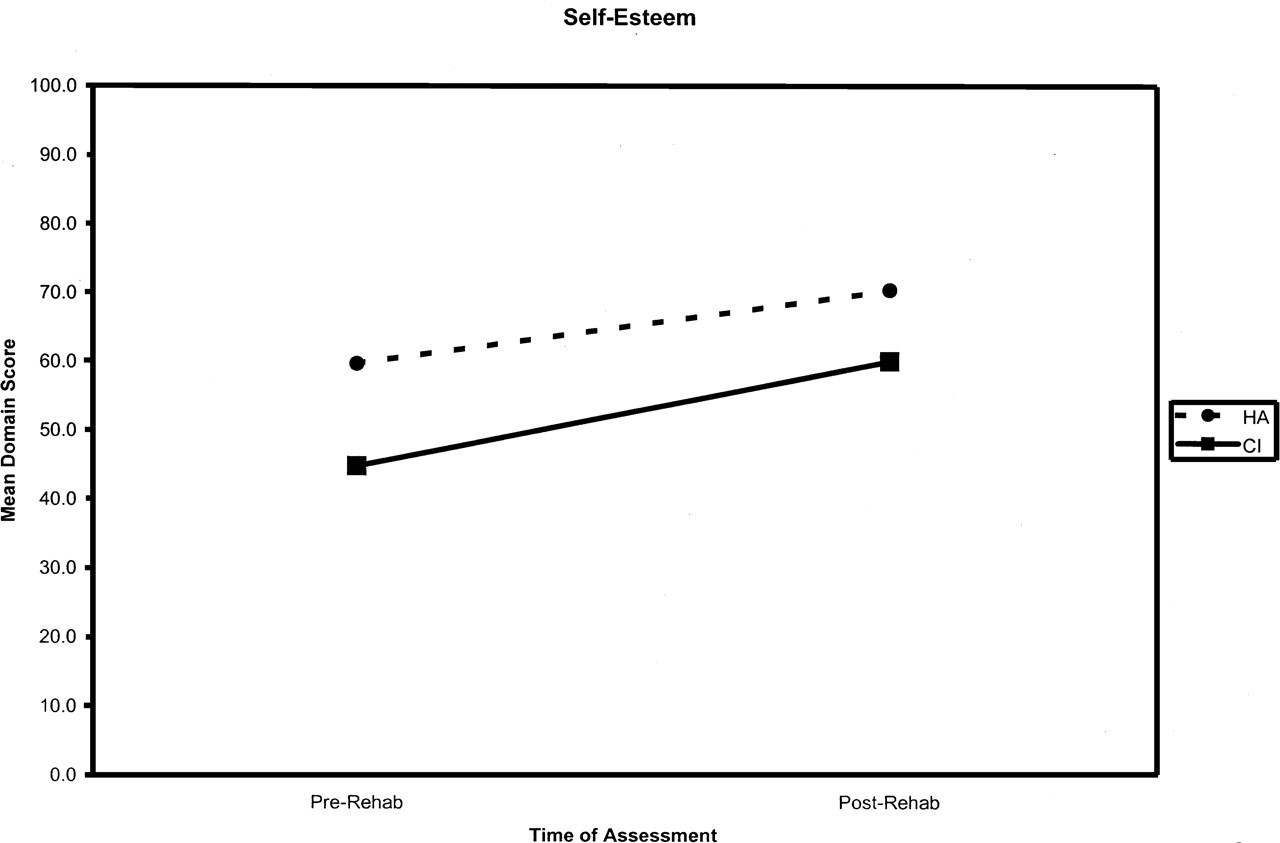
Change in self-esteem quality-of-life scores for cochlear implant vs hearing aid patients.
A few points regarding the study design are relevant. First, limited numbers did not allow subgroup analysis between different levels of hearing loss across the 2 groups. To avoid responder burden from multiple surveys, generic QOL measures were not mailed. This limited our ability to compare auditory rehabilitation's impact on QOL with other interventions for various disease states.
Health-related QOL data from the pre-rehab state was collected retrospectively, possibly leading to recall bias. Elderly patients or those further in time from their intervention may not accurately remember their preintervention state. By including current age in the regression model, we attempted to control for the relationship between age and QOL benefit. However, no association between time since intervention and QOL benefit scores was found, indicating that the passage of time alone did not result in greater improvement in postintervention QOL. Attempts to minimize respondents' remembering their pre-rehab answers and, subsequently, influencing their post-rehab answers, were made by sending the pre-rehab and post-rehab questionnaires a minimum of 2 weeks apart. Additionally, Hinderink et al showed that retrospectively collected preimplant QOL data from CI users was comparable to prospective QOL scores from patients with profound hearing loss on a CI waiting list. 12 While this supports the collection method of the preintervention data, future prospective studies are needed to corroborate our findings.
Because HA users consistently had higher pre-rehab QOL scores than CI patients (Figs 1–7), we remained open to the possibility of a “ceiling effect.” The HA users' milder degrees of hearing loss may have resulted in these higher pre-rehab QOL scores. By starting at higher levels, concern could arise that HA patients' scores may not have been able to improve as much as the CI users'. However, such a “ceiling effect” does not seem to have occurred. Compared to the CI group, the HA pre-rehab scores did not become prohibitively close to the maximum score of 100 (Figs 1–7).
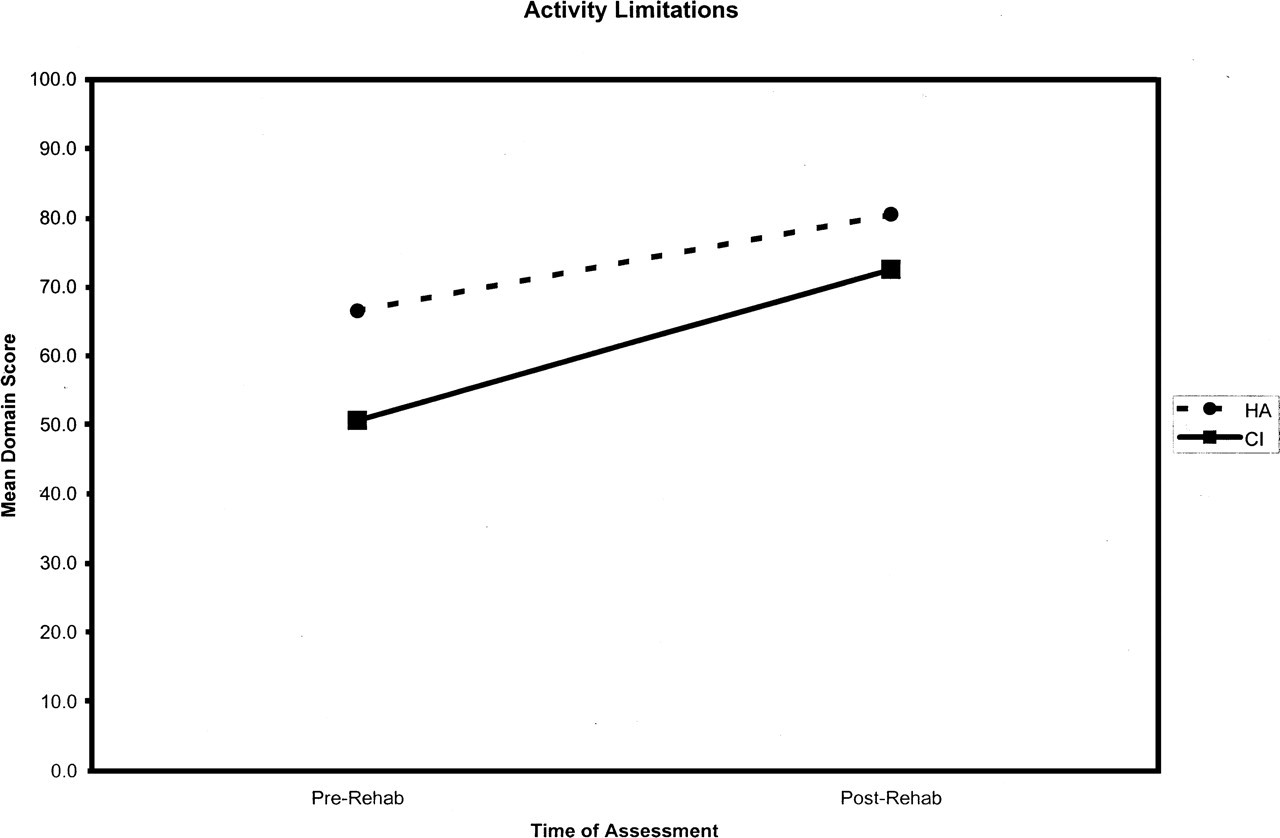
Change in activity limitations quality-of-life scores for cochlear implant vs hearing aid patients.
Lastly, although no statistically significant differences were seen between responders and nonresponders (Table 1), a selection bias likely existed. While all CI users did respond, only 61.2% of the HA users responded to the questionnaire (P ≤ 0.001, chi-square). The CI group includes patients who had improvements in their QOL as well as those with little or no improvement. In contrast, as determined by phone follow-up of nonresponders, the HA group excluded many poor performers. In fact, 21.1% of HA nonresponders verbally admitted that they quit using their aids due to frustration. Since the HA QOL measurements may be artificially inflated, the difference in QOL benefit received from CIs compared to HAs may be underestimated.
Despite the findings of this and other studies showing clear benefit in both auditory performance and QOL, many elderly patients are not receiving the benefits of cochlear implantation. Cost and difficulty obtaining coverage and reimbursement from health insurance companies have been barriers to implantation. 16 However, the favorable cost-effectiveness of adult cochlear implantation has been demonstrated. 20–22 Also, lack of awareness about cochlear implantation among other medical specialties has limited referrals. In a survey of primary care physicians, three-fourths did not refer adults for implantation most commonly because of uncertainty about patient candidacy and uncertainty about where to refer patients. 23 Because CIs reduced the functional gap between CI and HA users, exciting opportunities for auditory rehabilitation may be missed. Educating patients and physicians about the benefits of cochlear implantation can secure its essential role in treating hearing-impaired elderly adults.
CONCLUSION
HAs and CIs can reverse the resulting disability brought by hearing loss. Improved overall physical, psychological, and social functioning is possible with HAs and CIs. For patients with profound hearing loss, CIs may bring greater QOL benefit, as HAs do for patients with milder hearing loss. Future prospective studies should continue to explore QOL changes seen in CI and HA users with both health-related and generic QOL measures and to identify which patients are more likely to benefit from CIs and HAs.
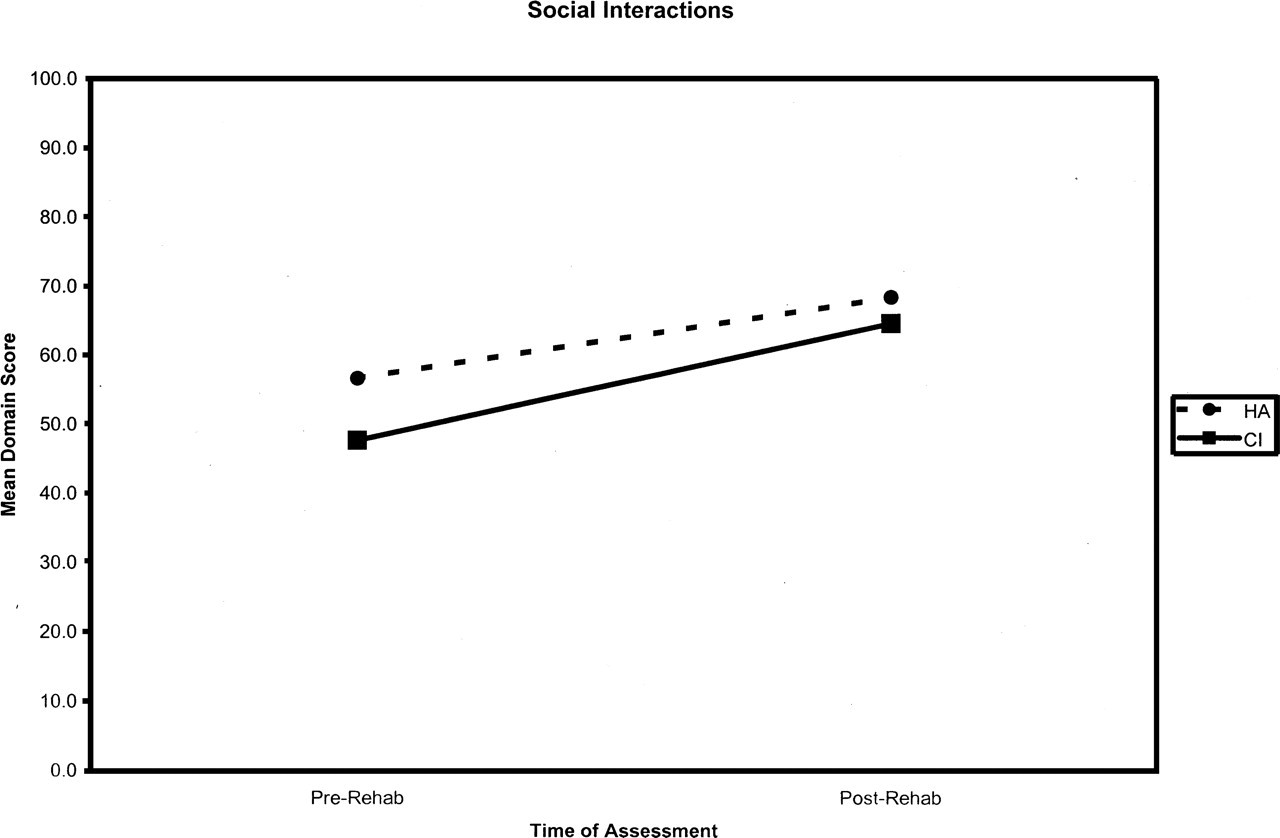
Change in social interactions quality-of-life scores for cochlear implant vs hearing aid patients.