
Abstract
OBJECTIVE: To examine pediatric temporal bone fractures in a rural population.
STUDY DESIGN AND SETTING: A retrospective chart review of pediatric temporal bone fractures between January 1, 1996, and December 31, 2000, at a rural academic medical center.
RESULTS: A total of 108 patients were identified. Common etiologies include falls, bicycle-related injuries, and motor vehicle accidents. Animal-related injuries were identified primarily in patients under 5. Facial nerve injuries were noted in 7%, hearing loss in 16%, additional skull base fractures in 65%, and intracranial injuries in 75%.
CONCLUSIONS: Temporal bone fracture etiology in the rural pediatric population is associated with age. Young children may suffer fractures secondary to animal-related accidents. Patterns of injury differ little between rural and urban settings.
SIGNIFICANCE: Animal-related accidents may be a significant cause of temporal bone trauma in rural young children. Our data remain unique in that we report additional skull base fractures as well as intracranial injuries in this population.
The long-term sequelae of temporal bone fractures can be significant, and include hearing loss and facial nerve paralysis. Hearing loss may be either conductive or sensorineural. Conductive loss results from hemotympanum, tympanic membrane rupture, or ossicular chain injury. Hearing may recover spontaneously or may require surgical intervention. Sensorineural loss is secondary to inner ear or auditory nerve injury and is associated with a poorer prognosis. 3
Facial nerve paralysis may be immediate or delayed. Incomplete paralysis tends to recover without intervention, 4 while treatment for complete facial paralysis remains controversial, and outcomes vary. 5
There are few studies on the subject of pediatric temporal bone fractures. Earlier studies have been performed at urban medical centers. 3,6–8 The Penn State Milton S. Hershey Medical Center (HMC) offers a novel perspective on the subject, due to its location in rural central Pennsylvania. The intent of this study is to examine the unique aspects of pediatric temporal bone fractures in a rural population. Our results were compared with earlier studies looking for any differences in etiology or sequelae.
METHODS
A retrospective chart review was performed, focusing on patients aged 17 years and younger discharged from HMC between January 1, 1996, and December 31, 2000, with the ICD-9 diagnosis codes 801.xx, indicating basilar skull fractures. All identified charts were reviewed for radiological confirmation of temporal bone fracture via formal radiology report. Only those charts with confirmation by official report were included in the study. Charts were then reviewed for other pertinent data related to the injury. Special attention was paid to available computed tomography scans (CTs) and audiograms. The data were analyzed and compared with previous adult and pediatric temporal bone fracture studies.
RESULTS
A total of 256 charts were listed with ICD-9 code 801.xx (skull base fracture) in patients 17 years old and younger between January 1, 1996 and December 31, 2001. Temporal bone fractures were confirmed by CT report in 108 patients at the time of admission. There were 71 males and 37 females.
All patients received a standard head CT as part of a pediatric trauma protocol. Three patients received dedicated temporal bone CTs at outside hospitals, and 6 patients underwent a temporal bone CT during their hospitalization. Only 31 patients (29%) were formally evaluated with an otolaryngology consultation. All 6 patients who received temporal bone CTs at HMC were within this group.
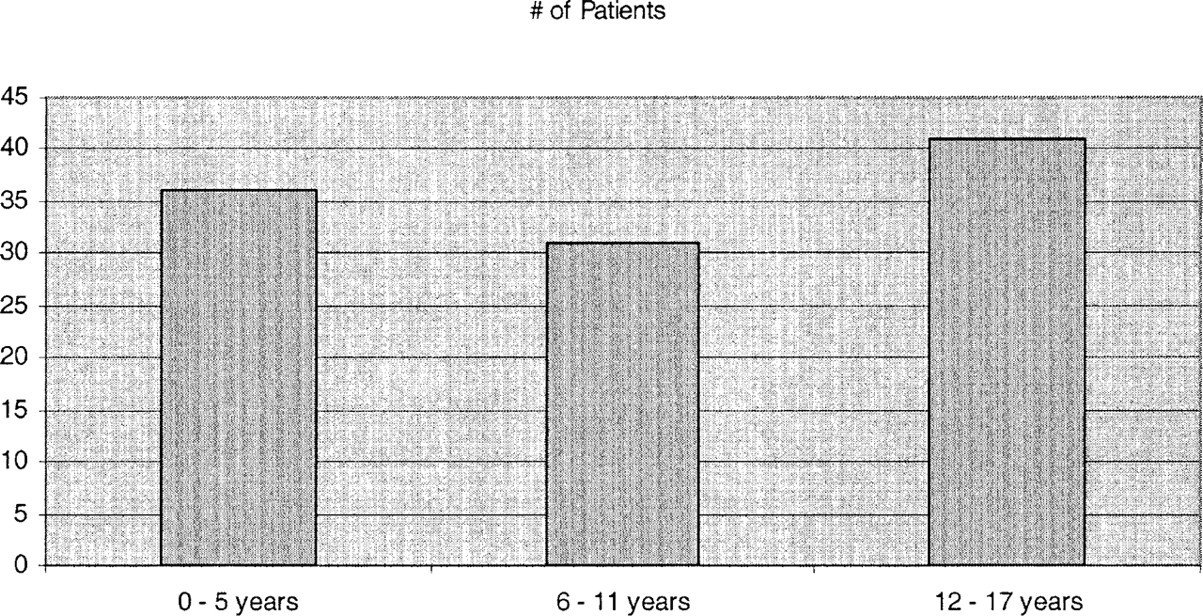
Age distribution of study population.
Patients were divided into 3 age groups, 0–5 years (36, or 33.3%), 6–11 years (31, or 28.7%), and 12–17 years (41, or 38%) (Fig 1). The most common etiologies of injury in the 0–5 group were falls (17, or 47.2%) followed by animal-related injuries (6. or 16.7%). In the 6–11 group, bicycle-related injuries (12, or 38.7%) caused the most fractures, followed by other falls (9, or 29%). In the 12–17 group, motor vehicle accidents (passenger or driver) dominated (19, or 46.3%), followed by pedestrian vs motor vehicle incidents (6, or 14.6%) and falls (6, or 14.6%) (Table 1).
Fifteen patients (14%) died as a result of their injuries. Five fatal injuries occurred in the 0–5 group, 3 in the 6–11 group, and 7 in the 12–17 group. The etiology associated with the highest mortality rate was pedestrian verses motor vehicle injuries (4/14, 29%) followed by motor vehicle accidents (6/27, 22%). Patients with bilateral fractures suffered a much higher mortality rate (63%) than those with unilateral fractures (10%).
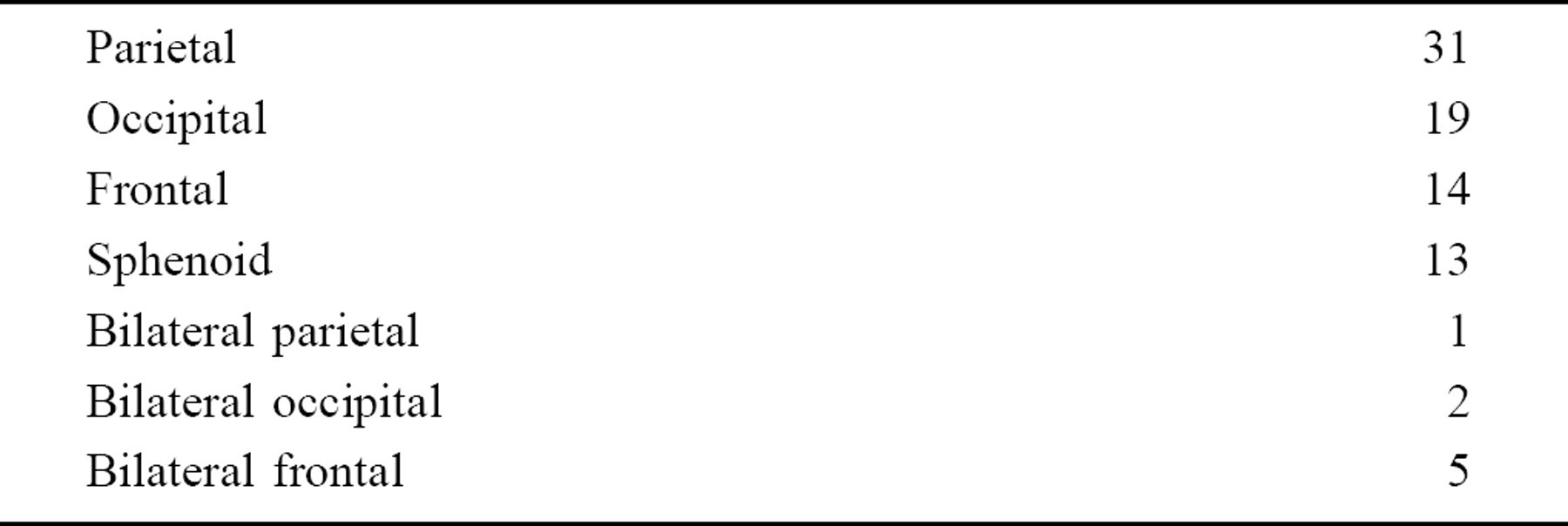
Temporal bone fractures are associated with other skull base fractures. Seventy patients (65%) had additional skull base fractures, either continuous with or discrete from the temporal bone fracture. Parietal bone fractures were most common (32/108), with 1 patient suffering bilateral parietal fractures (Table 2). An increased number of fractures was associated with increased mortality.
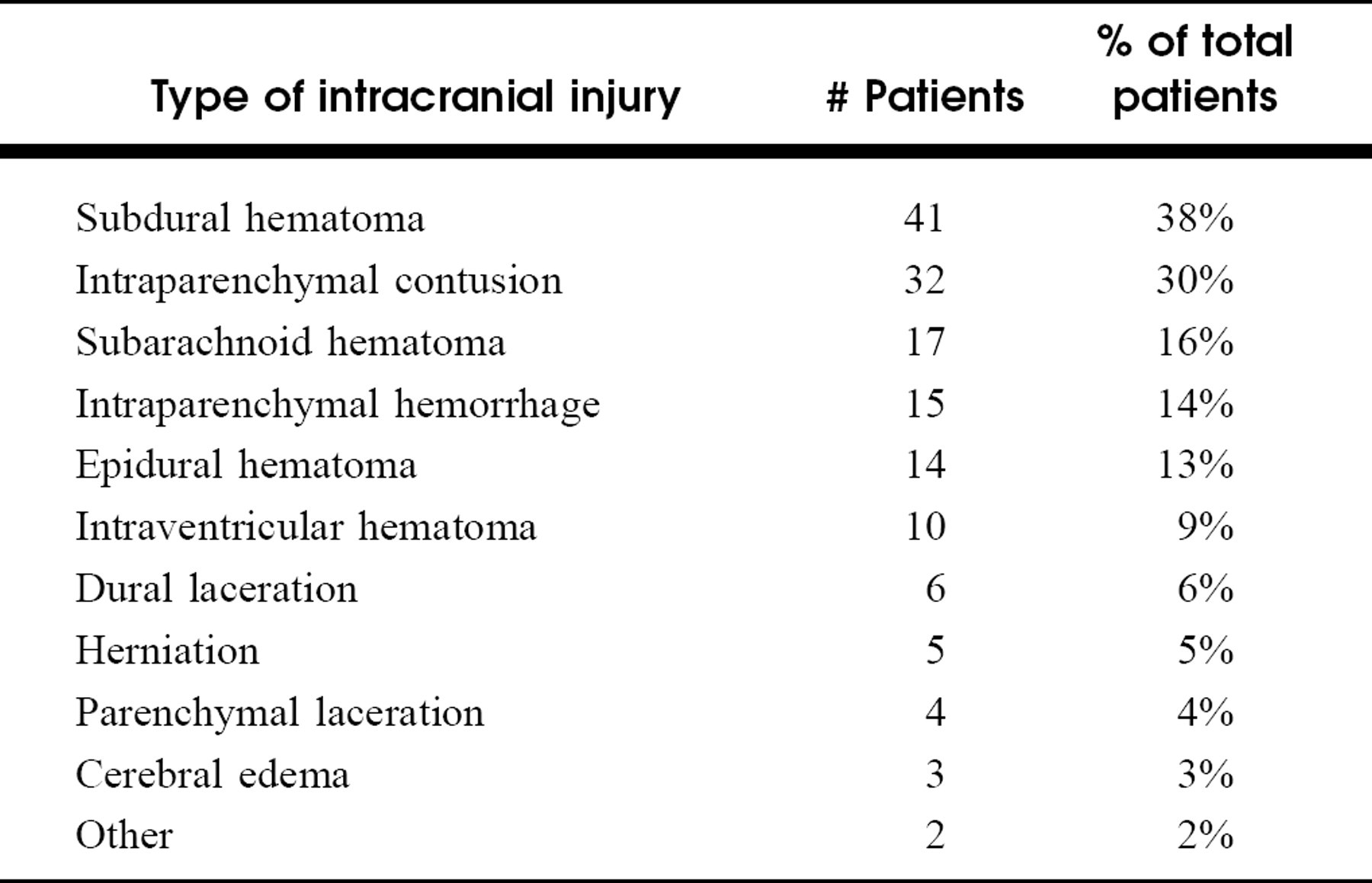
Intracranial injuries were identified in 81 patients (75%) by head CT. Multiple intracranial injuries were identified in 43 patients (40%). The most common injuries were subdural hematomas (38%) and intraparenchymal contusions (30%) (Table 3). All 15 fatalities had intracranial injuries.
Temporal bone fractures have characteristic presenting signs. Hemotympanum and/or blood in the external ear canal was noted in 45 patients (42%), Battle's sign was noted in 7 patients (6%), and cerebrospinal fluid (CSF) otorrhea was noted in 8 patients (7%). Two patients had CSF rhinorrhea due to anterior skull base fractures.
Meningitis is a rare complication of CSF leaks. Fifty-six patients (52%) received antibiotics during their admission. Fifty-four received intravenous antibiotics or a combined regimen of oral and intravenous antibiotics. Two were treated with oral antibiotics alone. Eight of the 10 patients with confirmed CSF leaks received intravenous antibiotics. There were no reported cases of meningitis.
Facial nerve weakness was noted in 8 patients (7%). Seven patients were noted to have immediate weakness, and 1 patient had delayed weakness. Three patients belonged to the 0–5 group, 1 to the 6–11 group, and 4 to the 12–17 group. The single patient with delayed weakness was treated with steroid therapy, but information on the degree of recovery was not available. Two patients with immediate and complete paralysis were treated with middle fossa surgical decompression and both were noted to have full facial nerve recovery. The information on the degree of weakness for the remaining 5 patients, as well as treatment and recovery, was not available.
Hearing loss was noted in 17 patients (16%), 6 in the 6–11 group and 11 in the 12–17 group. Fifteen were noted have hemotympanum. Eleven audiograms were available for review. Conductive hearing loss was noted in 9 patients, and sensorineural hearing loss was noted in 1. One patient with a left-sided temporal bone fracture was noted to have a bilateral loss, with an ipsilateral mixed loss and contralateral sensorineural loss. Seven repeat audiograms were available for review. Five ears with conductive loss experienced some recovery at 24 months. Neither ear with sensorineural loss had any recovery on follow-up audiogram (3 months and 22 months) (Table 4).
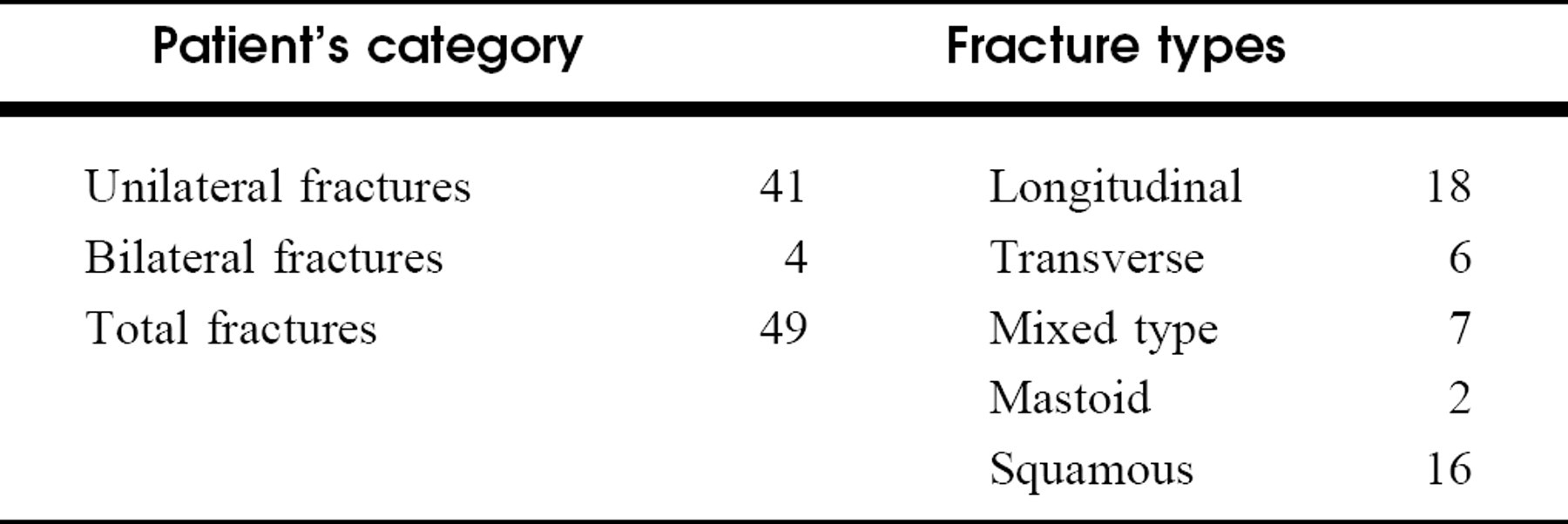
Forty-five CTs were available for review. Thirty-six had head CTs only, 3 had temporal bone studies only, and 6 had both. In total, 49 fractures were reviewed radiologically, with 41 unilateral fractures and 4 bilateral fractures identified. Longitudinal fractures were most common (49%), followed by squamosa only (33%), pure transverse (12%), mixed (6%), and mastoid only (4%) (Table 5). All fractures reviewed were otic capsule sparing. Specific intratemporal structures fractured included the temporomandibular joint (43%), the external auditory canal (37%), the carotid canal (22%), the jugular bulb (6%), and the internal auditory canal (2%) (Table 6).
DISCUSSION
Our study population is drawn from a large geographic area covering much of rural central Pennsylvania including urban Harrisburg. HMC is the regional level one trauma center. We looked for differences between our study population and those of previous studies preformed in large urban centers. Similar to previous studies, motor vehicle accidents (31%–60%) and falls (28%–46%) 3,6–8 were the most common mechanisms of injury. Animal-related injuries represent an etiology unique to our population. These injuries were the second most common cause of fractures in the 0–5 group. Such injuries were not reported earlier, and included dog attacks, horse falls and tramplings, and a kick from a cow.
Mechanism of injury by age group
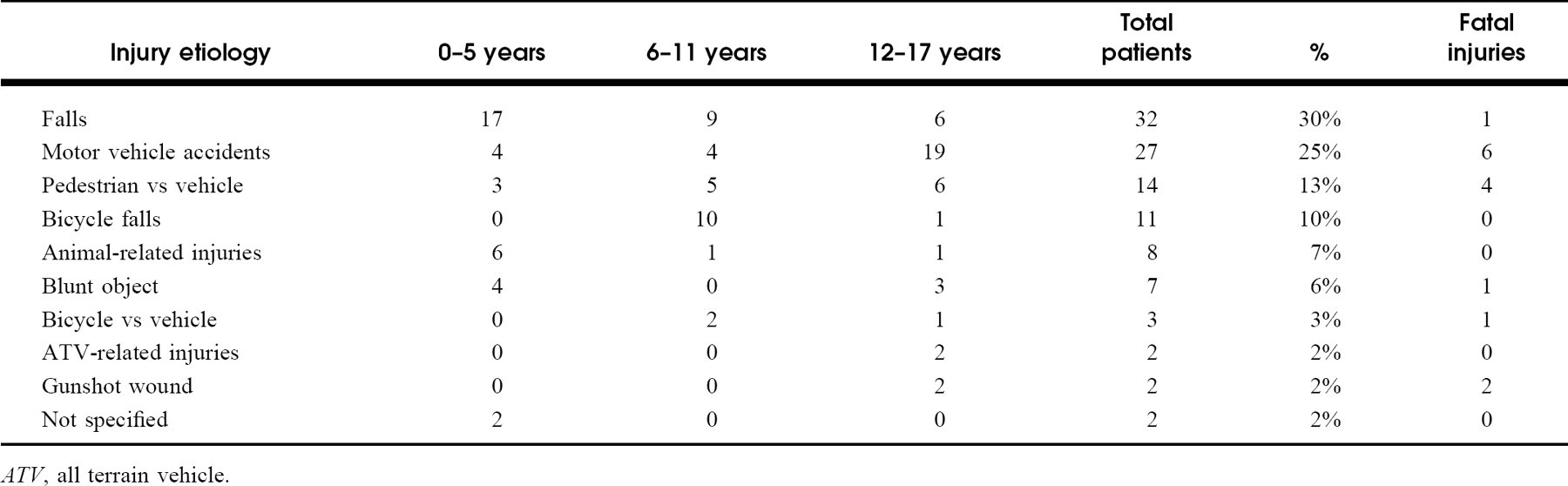
ATV, all terrain vehicle.
Additional skull fractures
Associated intracranial injuries
Degree, type, and recovery of hearing loss confirmed by audiogram
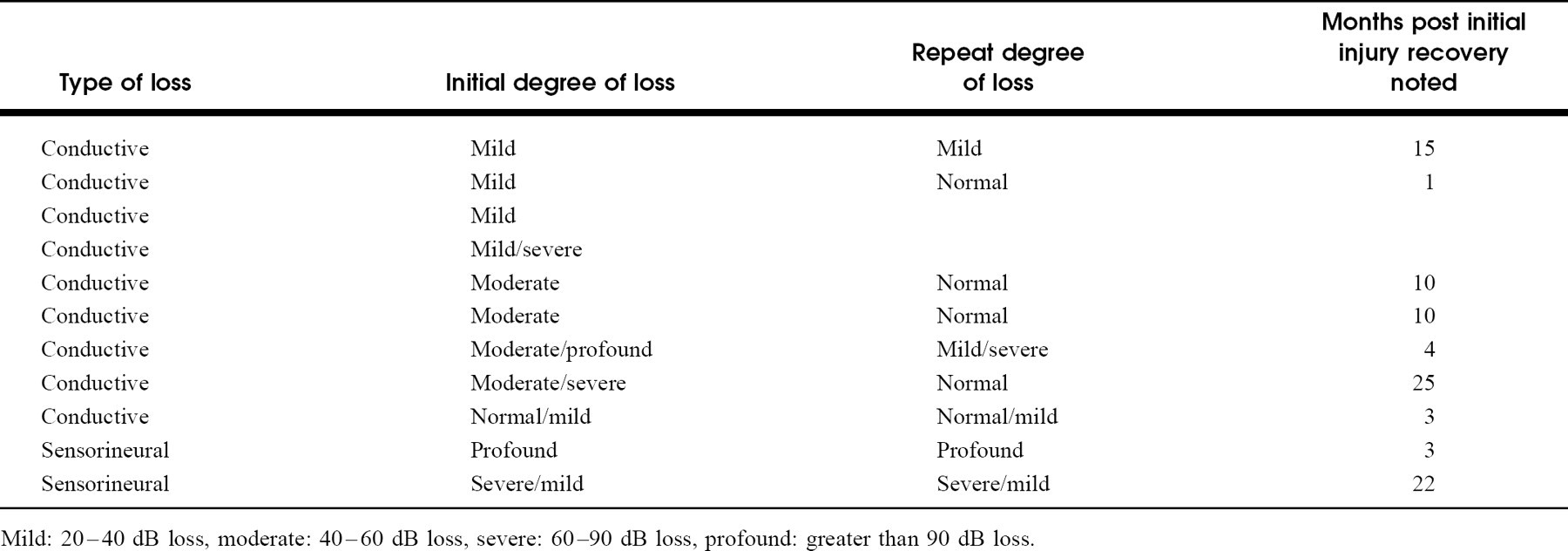
Mild: 20–40 dB loss, moderate: 40–60 dB loss, severe: 60–90 dB loss, profound: greater than 90 dB loss.
Fractures identified on available CTs
Facial nerve paralysis in pediatric temporal bone fractures has been noted to occur at a rate of 3% to 9%. 3,6–10 We found an incidence of 7%. While this number falls within the rates previously reported, it might represent underreporting, as nerve function was rarely assessed beyond gross facial symmetry on initial trauma assessment. Only 1 patient underwent formal electro-diagnostic testing.
Distribution of intratemporal injury by fracture type on available CTs
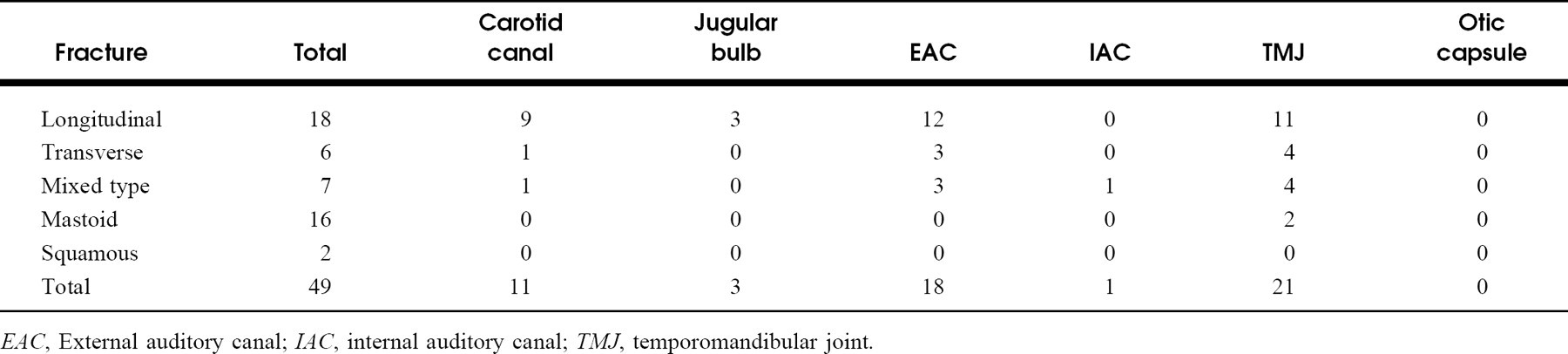
EAC, External auditory canal; IAC, internal auditory canal; TMJ, temporomandibular joint.
Facial paralysis is more common in adult patients with temporal bone fractures. Rates fall within 7% to 38%. 11,12 The difference has been ascribed to greater mineralization of adult temporal bones, and thus greater force transmitted to the facial canal during blunt trauma. 11
Hearing loss secondary to temporal bone fractures may be conductive, sensorineural, or mixed. Conductive loss results from hemotympanum, tympanic membrane perforation, or ossicular chain injury. Studies have shown that pediatric fractures most commonly result in conductive hearing losses. 3,6–8,10 Decreased mineralization of the pediatric temporal bone may also protect the dense otic capsule, limiting the risk of sensorineural hearing loss in this population.
Our population had a 16% rate of hearing loss. This is much lower than the 33% to 85% 3,7,8 previously published. This discrepancy may result from study methods. Previous patient groups received audiograms routinely as part of their inpatient assessment. Patients at HMC received audiograms only as follow-up to clinical signs of hearing loss. Young and preverbal children are especially difficult to assess for hearing loss. This may explain the lack of reported hearing loss in the 0–5 group.
Associated intracranial injuries played an important role in the morbidity and mortality of our patients. One pediatric study noted a rate of intracranial injury at 23%. 3 An adult study found 84% of their subjects had at least one type of intracranial injury, and 39% of these patients had multiple injury types. 12 This is consistent with our findings of a 75% injury rate and 40% multiple injury rate. Our group of children over the age of 5 were more likely to be involved in a high-speed mechanism of injury, making them more susceptible to intracranial injuries.
Our study is unique in that we report specific additional skull fractures, specific intracranial injuries, and specific intratemporal injuries. To our knowledge, this data had not previously been reported in this population. What seems most impressive is the very high number of fractures extending into the glenoid fossa. These children potentially are at risk for long-term occlusion and temporomandibular joint problems. Careful follow-up would be required to further investigate this. Also notable is that none of the CTs that we reviewed revealed a fracture involving the otic capsule.
Our study has all of the weaknesses of any retrospective chart review. Data regarding patients is based on what is documented, which remains variable from physician to physician and from patient to patient. Also, our pediatric trauma service has at times not requested an otolaryngology consultation for its patients, and thus much of the data is simply not available for our population. This is especially obvious when trying to draw conclusions regarding facial nerve injuries or hearing loss.
CONCLUSIONS
Temporal bone fractures represent significant morbidity and mortality in rural pediatric patients. The most common etiologies include motor vehicle accidents and falls. Etiologies are strongly influenced by patient age, and animal-related accidents are more common in children less than 5 years of age. Head CTs are necessary to identify intracranial injuries as well as additional skull base fractures. Temporal bone–specific sequelae in pediatric patients include hearing loss and facial nerve paralysis. Based upon comparisons with previously published work, patterns of injuries differ little between rural and urban settings (Table 6).