
Abstract
OBJECTIVE: To evaluate children with obstructive sleep apnea syndrome (OSAS) for features of attention deficit disorder (ADD) using an objective test of inattention and impulsivity: Test of Variables of Attention (TOVA) and then to determine whether tonsillectomy and adenoidectomy (T+A) results in an improvement in TOVA scores.
STUDY DESIGN AND SETTING: This study was a prospective interventional comparative trial in a tertiary care children's hospital. Nineteen children ages 5 to 14 years with OSAS, and otherwise healthy, with a clinical indication for T+A. Preoperative and 2 months postoperative OSA-18, CBCL questionnaires, and TOVA scores were evaluated.
RESULTS: The preoperative TOVA scores were in the abnormal range in 12/19 (63%) of the children. The mean preoperative TOVA score was −2.9 (± 3.1). The mean postoperative TOVA score was −0.4 (±2.8). The improvement in the TOVA scores was significant (P < 0.0001, t-test).
CONCLUSION: This preliminary data suggests that treatment of OSAS with T+A results in significant improvement in objective parameters of inattention and impulsivity.
SIGNIFICANCE: These findings may be important in understanding the impact of OSAS and therapeutic interventions on behavioral problems in children.
The nighttime symptoms of OSA include snoring, breathing cessation, choking, gasping, struggling to breathe, restless sleep, and frequent awakenings. Although daytime sleepiness may be present, it is not a common symptom in children as compared with adults. 1 Daytime symptoms that are more frequently associated with OSA in children include learning difficulties, attention disorders, hyperactivity, aggression, and antisocial behavior. 1–5 When OSA is not recognized and is left untreated, significant morbidity such as failure to thrive, systemic hypertension, and pulmonary hypertension with or without cor pulmonale can develop. 1 Data is emerging regarding neurocognitive sequela.
In the vast majority of children with OSA, surgical removal of hypertrophic tonsillar and adenoid tissue will usually result in complete resolution of OSA. 1 By using standardized behavioral assessments, recent reports support the association between behavioral and attention problems in children with sleep-disordered breathing. 3–7
The Test of Variables of Attention (TOVA) has been used as objective measures to assist in the diagnosis of attention deficit hyperactivity disorders (ADHD). 8,9 TOVA is a 23-minute visual continuous performance test with minimal language demands, no left-right discrimination, and has a proven test-retest validity. 8–11 The test is done in the form of a computer game allowing for excellent cooperation by the child. In this study, TOVA was used to evaluate attention and concentration in children with OSAS before and after tonsillectomy and adenoidectomy (T+A).
The OSA-18 is an 18-item health-related quality of life survey of pediatric OSAS that has been correlated with the respiratory disturbance index on nap polysom-nography. It has been shown to have a high level of reliability, validity, and responsiveness. 12,13
The Achenbach Child Behavior Checklist (CBCL)/4–8 attention problems syndrome scales is an 11-item standardized parent report questionnaire designed to evaluate behavioral problems in children between the age of 4 and 18. The CBCL has a high validity for detecting attention problems and is widely used in comparative studies. 14,15
The purpose of this study was to determine the impact of T+A on attention in children with OSA using TOVA as an objective tool. To our knowledge, no prior study has used an objective measure of ADHD for the evaluation of children with OSAS before or after treatment.
PATIENTS AND METHODS
In a prospective cohort interventional outcomes study, children ages 5 to 14 years presenting to the Pediatric Otolaryngology Outpatient Clinic in our institution between April 2002 and March 2003 who were scheduled for tonsillectomy and adenoidectomy (T+A) for upper airway obstruction were included. The indication for T+A was a more than 3-month history consistent with OSA as measured by parental observation of continuous loud snoring with occasional cessation of breathing or respiratory effort during sleep and a physical examination that demonstrated adenotonsillar hypertrophy. Tonsillar hypertrophy was considered when tonsil size was 3+ and above on a scale of 1 to 4+. Adenoid size was assessed by fiberoptic endoscopy or lateral neck x-ray and hypertrophy considered when 3+ or above.
Exclusion criteria included airway obstruction that was not only due to adenotonsillar hypertrophy, such as craniofacial anomalies, neurological impairment or when T+A was contraindicated. Children with a prior diagnosis or suspicion of ADHD were also excluded.
Prior to surgery and 2 months postoperatively all children were administered TOVA. The children's parents completed 2 questionnaires: the OSA-18 and attention CBCL/4–18. The children also had a clinical and physical evaluation by a pediatric otolaryngologist before surgery and 2 months postoperatively. A detailed description of TOVA is beyond the scope of this paper. 8–11 In brief, TOVA is a 23-minute fixed-interval visual continuous performance test with minimal language demands and no left-right discrimination. It is similar to a computer game. The child observes the monitor as targets are presented. When he/she sees a target he/she presses on a microswitch. Targets and nontargets are randomly presented and the child must differentiate between them and press the switch only for targets. Every 2 seconds, a stimulus will flash on the screen and the subject then responds to the targets and not to the nontargets. In such a manner, TOVA evaluates omission and commission errors, response times, and anticipatory responses. Errors of omission are indicators of inattention. Errors of commission are indicators of impulsivity. These errors, response times, and other variables are all recorded for each 5-minute quarter and 10-minute halves, as well as overall total scores for each variable. Scores are then compared to standardized norms and an interpretation of the data is summarized in a printable report. The manual recommends that the diagnosis of attention deficit disorders be consider when there is a 1.5 standard deviation from the age- and sex-adjusted mean.
The OSA-18 questionnaire consists of 18 survey items divided into 5 domains (sleep disturbance, physical symptoms, emotional symptoms, daytime functioning, and caregiver concerns). The items are scored on a scale of 1 to 7. 12,13
The CBCL/4–8 attention problems syndrome scales is an 11-item standardized parent report questionnaire designed to asses behavior problems in children between the age of 4 and 18. 2 The CBCL has high validity for detecting attention problems and is widely used in comparative studies. Each item is scored as follows: 0, not true; 1, somewhat or sometimes true; and, 2, very true or often true. The total score can also be compared with the score of children in normative samples.
Statistical Analysis
The TOVA score of each child was compared before and after surgery using a matched 2-tailed t-test. The OSA-18 and the CBCL parental questionnaire scores were compared before and after surgery with a matched 2-tailed t-test. A P-value < 0.05 was considered significant.
Permission was obtained from the institutional review board for human investigations in our hospital (Helsinki committee). Informed consent was obtained from all parents.
RESULTS
A total of 19 children (8 females and 11 males) completed preoperative and postoperative surveys. Mean patient age was 7.97 (range, 5–14).
The OSA-18, CBCL, and TOVA preoperative and postoperative mean scores are presented in Table 1. There was a significant improvement in the OSA-18 scores with a 46% reduction in scores postoperatively reflecting improvement of sleep-related quality of life (P < 0.0001). Sleep disturbance, physical symptoms, and caregiver concerns were the highest rated domains, followed by daytime function and emotional symptoms. The improvement in OSA-18 scores before and after surgery was significant for all domains except for emotional symptoms (Table 2).
Preoperative and postoperative TOVA, OSA-18 and CBCL scores

P values using a matched 2-tailed t-test. Improvement was significant in all 3 parameters.
OSA-18 domains before and after surgery
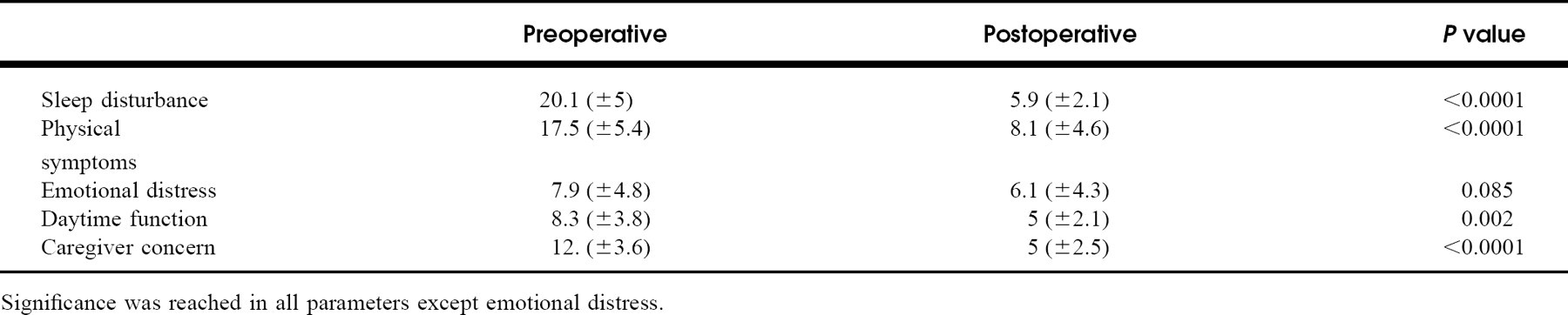
Significance was reached in all parameters except emotional distress.
There was a significant change in the mean CBCL score, which showed a significant improvement from 6.1 before to 3.8 after the operation (P < 0.018). This indicates an improvement in attention related items of this questionnaire.
All children with the exception of 1, showed significant improvement in their TOVA scores after T+A. The mean improvement was from −2.9 preoperatively to −0.4 postoperatively (P < 0.0001).
Prior to surgery, 36% (7/19) of the children had TOVA scores within normal limits. These scores improved significantly after surgery. In addition, 42% (8/19) of the children had preoperative TOVA scores below normal limits that improved into the normal range following surgery. In 21% (4/19) of the children, TOVA scores remained below normal limits postoperatively. Nevertheless, an improvement was observed in all the children except 1 (Fig 1).
DISCUSSION
Our understanding of the relationship of SDB in children to learning and behavioral problems is incomplete. Recent studies have suggested an association between poor behavior and neurocognitive performance in children with SDB. These studies also showed that therapeutic surgical intervention resulted in significant improvements in school grades, or in standardized behavioral assessments. 1,2,5–7,16 However, these studies examined the child's behavior and neurocognitive performance on the basis of questionnaires, intelligence tests, and school grades. Using these methods, behavior rating is subjective and susceptible to certain biases. In this study, we used the TOVA, which is considered an objective tool used to measure attention in children and to aid in the diagnosis and treatment of ADHD. 9–11 This study is the first, to our knowledge to use the TOVA to estimate attention problems in children suffering from OSAS.
TOVA is widely accepted as an ancillary test for the diagnosis of children with ADHD over 5 years old. It is also used for monitoring medication effectiveness in these children. This test has proved to have test retest reliability; there is no learning effect on repeated administration of the test. 10
This study revealed an association between OSAS and attention problems in children. The TOVA scores prior to surgery in this cohort were pathological in 12/19 (63%) of the children, though they were not previously diagnosed with behavioral problems. This high percentage of pathological TOVA scores in this cohort is alarming especially considering that children that were suspected to have ADHD were excluded from the study. This result may be due to a sampling error in this small group of children. A large longitudinal study is needed to verify the magnitude of this result. Of importance was the significant improvement in the TOVA scores after surgery, paralleling improvement in their SDB as assessed by the OSA-18 questionnaire. This improvement in attention might have a great influence on the child's daily behavior, quality of life, and school performance, as was demonstrated in other studies.
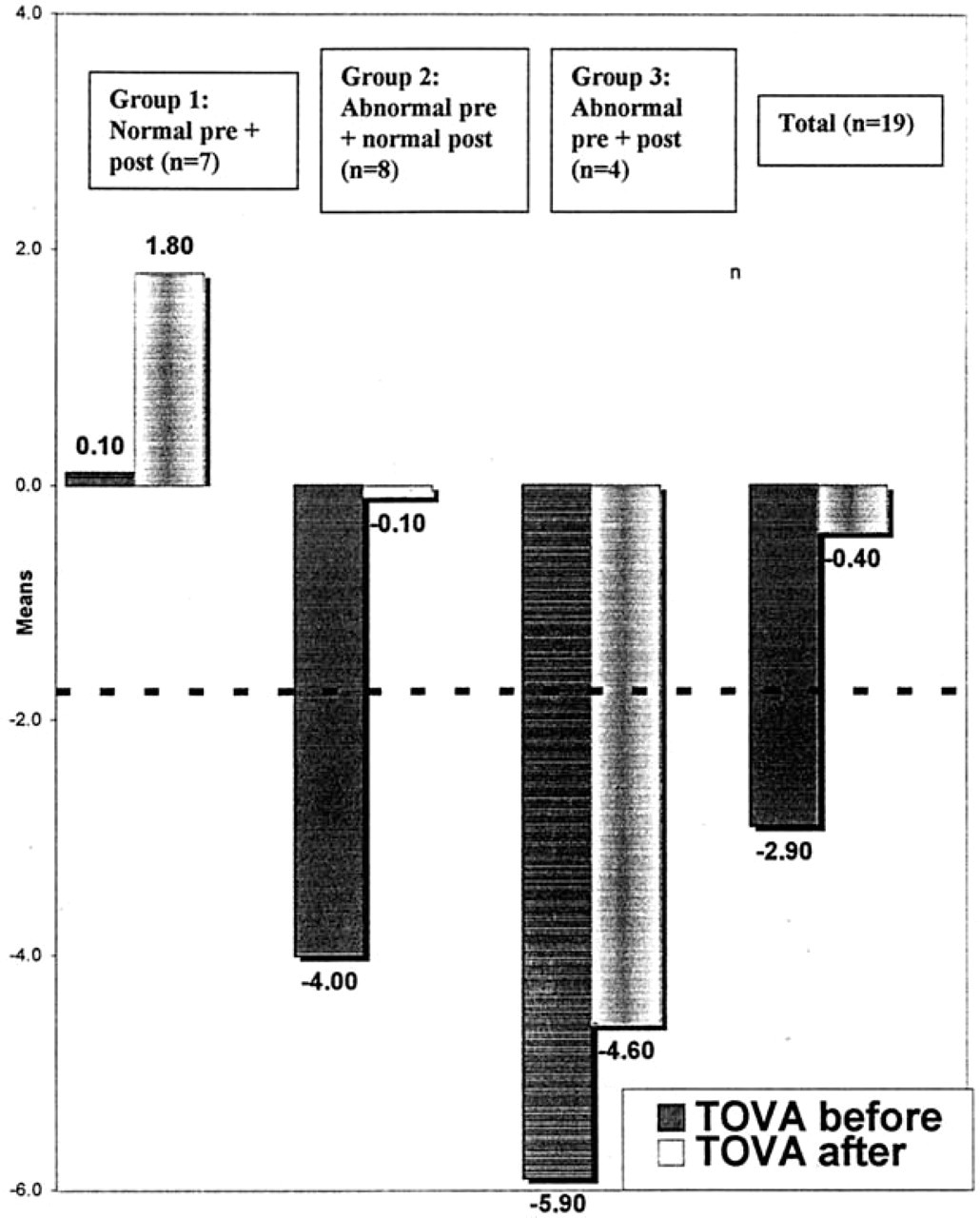
TOVA scores in 3 subgroups before and after surgery. Group 1 with normal preoperative and postoperative scores showing improvement. Group 2 with abnormal preoperative scores that improved to the normal range. Group 3 with abnormal preoperative and postoperative scores but still improved. TOVA scores in the whole group (n = 19) showed improvement. Scores below the thick dotted line represent abnormal TOVA scores.
Gozal 3 demonstrated a significant change in school performance in children with SDB that underwent T+A as compared to a control group of children with SDB that their parents elected not to seek therapeutic intervention. Bluden et al 5 showed that compared with controls, children who snore have significantly impaired attention and, although within the normal range, lower memory and intelligence scores. Goldstein et al 6 demonstrated a high prevalence of abnormal behavior in children undergoing T+A for chronic upper airway obstruction. Scores on a standardized measure of behavior questionnaire improved following T+A. 4,6 Serres et al 7 showed a large improvement in at least short-term quality of life in children with OSAS following treatment.
The present population of children comprised of 3 groups according to preoperative TOVA scores. One group had a score within the normal range but still showed an improvement in scores. The abnormal TOVA scores split into 2 groups, 1 with an improvement of scores to the normal range, the other improved but remained in the abnormal range. If children with behavioral problems are referred for treatment of SDB it should not be taken for granted that the behavioral problems will resolve in all cases. Possible explanation can found in earlier studies. Gozal and Pope 17 found a correlation between children with lower academic performance in middle school and snoring in early childhood. They concluded that residual deficits in learning performance may still be detected even several years after snoring has resolved. O'Brien et al 18 found an unusually high prevalence of snoring among children with mild symptoms of ADHD. However, in children with severe ADHD there was a similar prevalence of OSA as in the general pediatric population. Thus, the findings of these authors suggest that although OSA can cause mild behavioral effects it does not seem to mimic more severe ADHD symptoms. 18
The patient population in this study was small, but using each child as his/her own control, statistical analysis was possible and significance was reached. The improvements in objective measures coincided to the improvements in the subjective questionnaires. Even in this small group, significance was reached showing improvement in all children using behavioral subjective and objective parameters of ADHD. Using TOVA as an objective measure of ADHD-related behavior may prove to be an important tool in evaluating children with SDB. T+A in children with OSA appears to have a positive effect on the child's ability to pay attention.