
Abstract
OBJECTIVE: To assess the use of titanium prostheses in tympanoplasty for reconstruction of the sound pressure and to evaluate the audiometric results obtained.
STUDY DESIGN AND SETTING AND PATIENTS: Retrospective chart review in a tertiary referral center. Between September 1998 and October 2000, 23 titanium middle ear implants (23 TORP) were used for reconstruction of the ossicular chain after tympanomastoidectomy. Preliminary functional results were obtained in 23 cases.
RESULTS: Average follow-up time was 18 months (range, 12-40) and no adverse reactions or extrusions occurred. Seven of 16 canal wall down tympanoplasties (43.7%), and 3 of 7 canal wall up tympanoplasties performed (42.9%) had a postoperative air-bone gap of between 0 and 10 dB.
CONCLUSIONS: Preliminary results show that titanium prosthesis provide a promising hearing result after total ossicular reconstruction, although long-term results are not yet available. The low weight of these prostheses may be the reason for the decrease in the air-bone gap.
The ideal middle ear implant for hearing reconstruction in chronic ear surgery should have 4 characteristics: it should be compatible, readily available, technically easy to use, and it should give the best possible hearing results. Because autologous ossicles often cannot be used as a result of underlying disease, homografts may transmit infectious, alloplastic materials are frequently considered as an option for reconstruction.
The best hearing results are achieved with a straight columella-type ossicular reconstruction, either from the footplate or from the stapes toward the malleus or the tympanic membrane. In contrast, angled reconstructions do not provide an ideal transmission of the sound pressure.
Titanium has been used as a prosthetic material for many years in craniofacial and orthopedic surgery. 1 Animal experiments have indicated that titanium is a useful material in the special environment of the middle ear space, 2 and several studies report a hearing improvement after tympanoplasty with titanium prostheses. 3-5 Among the advantages of titanium are the absence of bone-bonding and its low weight of approximately 4 mg.
MATERIALS AND METHODS
A computerized otologic database was used to identify all patients undergoing tympanomastoidectomy with reconstruction of the ossicular chain between September 1998 and October 2000. Pure-tone air and bone conduction thresholds were obtained preoperatively and postoperatively. Air and bone conduction 4-frequency (0.5, 1, 2, 4 kHz) pure-tone averages (PTA) were used to calculate the PTA air-bone gap. Follow-up of at least 12 months was required for inclusion in the study. In total, we found 23 cases of tympanomastoidectomy using total ossicular replacement prostheses (TORP) of 4.5 mm in length.
Surgical Technique
Autograft cartilage palisade was used for reconstruction of the tympanic membrane, as described by Heermann. 6 Cholesteatomas were operated on as a single-stage procedure under general anesthesia. Approach to the cholesteatoma started from the outer ear canal (scutum) and performing consecutively, depending on the extension of the cholesteatoma, an atticotomy, an antrotomy or a mastoidectomy with a canal wall down. Thus, mainly the extension of the cholesteatoma was a selection criteria for canal wall up or canal wall down. All atticotomies or smaller antrotomies were closed by means of cartilage in contact with the preserved canal. Open cavities were obliterated partially or totally with a cartilage from the cavum conchae. Cartilage was cut into smaller pieces used to fill up the anterior epitympanum, antrum, and to cover the horizontal semicircular canal. A meatoplasty with cartilage excision from the concha (subsequently used for obliteration) was performed in all canal wall down procedures. 7 The cartilage was usually harvested from the cymba when the incision was retroauricular or from the tragus when the approach was endaural.
Canal wall up tympanoplasties (n = 7)
The preparation of TORP requires trimming the shaft to the appropriate size. The stem has breaking points at distances of 1 mm to allow the selection of the correct measurement. The prosthesis was placed on the footplate, in some cases between the crura of stapes. In all cases, the prosthesis was protected with one of the cartilage palisades to avoid extrusion.
RESULTS
We reviewed 23 cases of tympanoplasty type III (Wullstein classification) performed between September 1998 and October 2000 in which titanium middle ear implants (23 TORP) were used. Of the patients, 17 were men and 6 were women, 15 were right ears and 8 left ears. The average age of the patients was 37 years, 7 months (range, 8-65 years). Preoperative diagnoses are shown in Tables 1 and 2. The average follow-up was 18 months (range, 12-40 months).
In 21 cases, a complete reconstruction of the tympanic membrane using palisade cartilage was performed. One 8-year-old girl had a bilateral minor malformation of the ossicular chain. No extrusion of the prosthesis or any perforation of the tympanic membrane was observed.
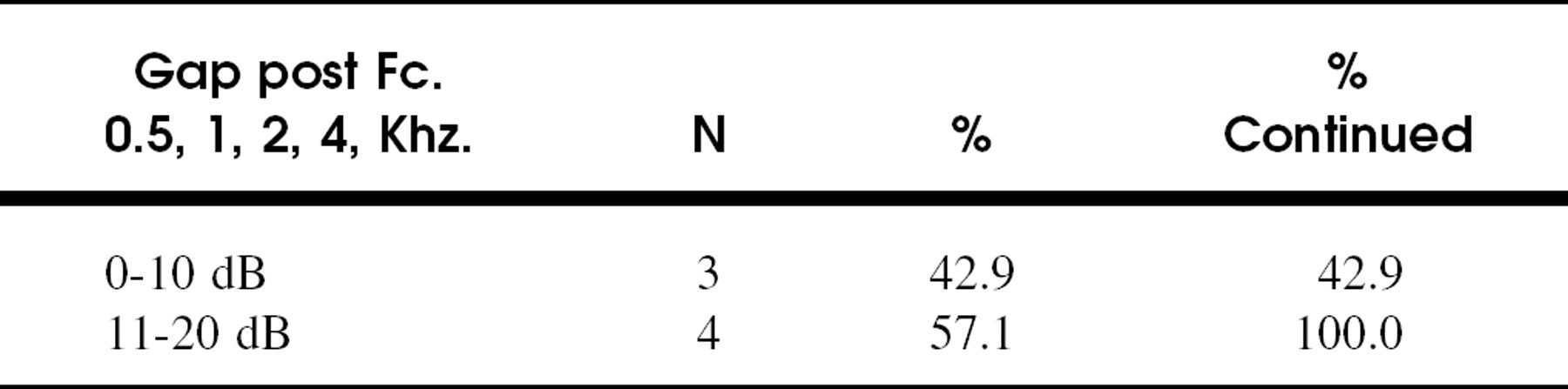
Seven ears (30.4%) had a tympanomastoidectomy with canal wall up. A hearing result of 0 to 10 dB residual air-bone gap was achieved in 42.9% of cases; all results were within the 0- to 20-dB range (Table 3).
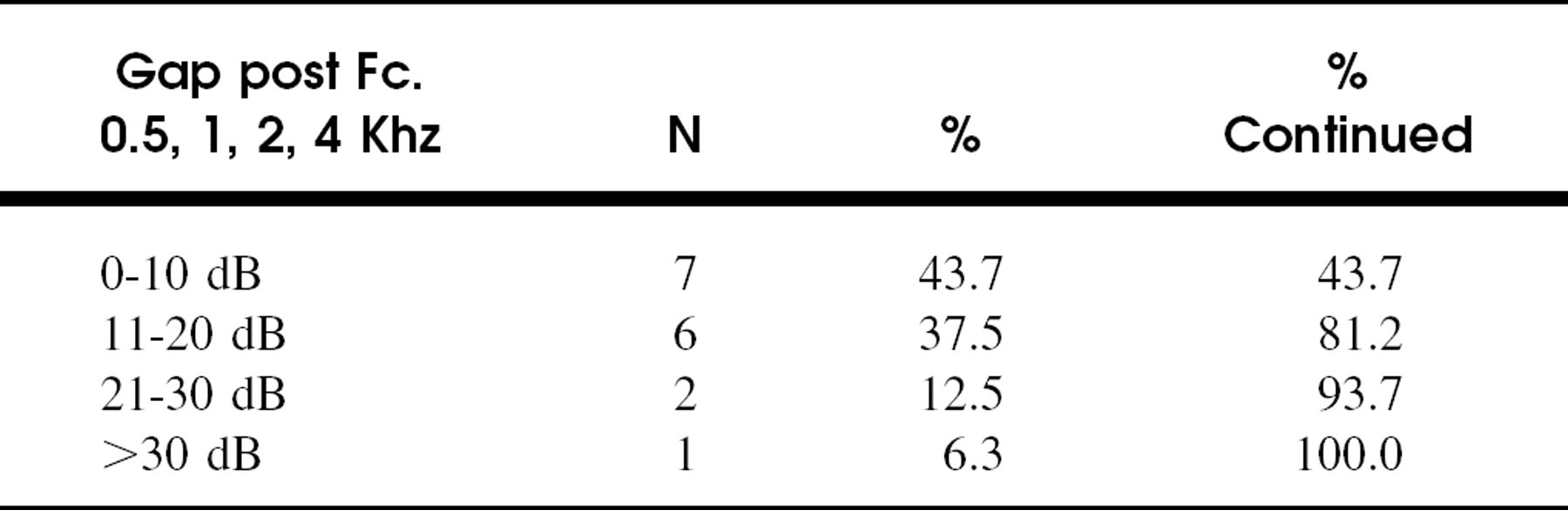
Sixteen ears (69.6%) had a tympanomastoidectomy with canal wall down, either as a primary procedure (n = 7) or as a revision (n = 9). A hearing result of 0 to 10 dB residual air-bone gap was achieved in 43.7% of cases; and results within the 0- to 20-dB range were obtained residual in 81.2% of the cases (Table 4).
DISCUSSION
Because of the current concern regarding the possible transmission of viral infections by means of homologous middle ear implants, 8 the search for other biocompatible materials has intensified.
Titanium has shown a high biocompatibility and close affinity to human body tissues. It is nontoxic, nonmagnetic, chemically stable, and nonerosive. Its specific density is low (57% that of stainless steel), and it is extremely strong. It has been used as a prosthesis in reconstruction of the ossicular chain, and clinical studies report favorable results. 3-5 The affinity of titanium to bone, known as osseointegration, has been shown in bone-anchored devices; 9 it has also been observed experimentally in the middle ear. 2 In titanium prostheses obtained during revision surgery and studied by scanning electron microscopy no macrophages or foreign body reactions were seen. 10
Canal wall down tympanoplasties (n = 16)
CWD, canal wall donor.
Postoperative air-bone gap in patients followed of at least 12 months with canal wall up timpanoplasties (n = 7)
Postoperative air-bone gap in patients followed of at least 12 months with canal wall down tympanoplasties (n = 16)
In a recent study, Plasti-Pore showed a better hearing result compared with titanium, especially when a canal wall up operation was performed. 11 However, in another preliminary study with titanium total ossicular prosthesis, 89% of patients had closure of the postoperative air-bone gap to within 20 dB compared with porous polyethylene total ossicular prosthesis, in which 67% patients closed the air-bone gap to within 20 dB. 12
After a mean follow-up of 18 months, the hearing results with titanium prostheses are promising in our hands. With the same surgical technique, but using glass ionomer prostheses, the postoperative air-bone gap was between 0 and 10 dB in only 29.6 %, and between 11 and 20 dB in 32.4%. 13,14
CONCLUSIONS
We have used titanium prostheses and palisade cartilage for tympanoossicular reconstruction. The preliminary hearing results suggest that titanium prostheses are ideal for the reconstruction of the ossicular chain. Long-term follow-up is needed to assess the compatibility and hearing results. We believe that the low weight of these prostheses (4 mg) is one of the reasons for the improved sound transmission.