
Abstract
OBJECTIVE: To review a single surgeon's experience utilizing an intraoperative methylene blue infusion (IMBI) to identify parathyroid glands during neck exploration for primary hyperparathyroidism.
STUDY DESIGN AND SETTING: Retrospective review of 35 patients who underwent bilateral neck exploration utilizing an IMBI at a dose of 7.5 mg/kg following the induction of general anesthesia.
RESULTS: All patients reverted to normocalcemia with a mean follow-up of 17 months. IMBI facilitated the identification of abnormal parathyroid tissue in 34/35 patients (97%). A dark blue-purple staining was observed in 33/37 stained adenomas (89%). Four adenomas and four hyperplastic glands stained a lighter shade of blue-green. Among 89 normal glands, 41(46%) stained a pale green-grey color.
CONCLUSIONS: IMBI is a safe, readily available, cost-effective, and underutilized technique that facilitates rapid identification of parathyroid adenomas, helps distinguish normal glands from hyperplastic glands, and helps to locate ectopic glands. An overall reduction in operative time, especially for bilateral neck exploration, can be anticipated.
Since parathyroid glands are often inconspicuous, their identification can be a challenging problem when performing neck exploration for the treatment of hyperparathyroidism. Normal parathyroid glands can be a few millimeters in size (especially when suppressed by hypercalcemia), of variable color, and supernumerary. They may also be surrounded by or imbedded in adipose tissue or confused with small paratracheal lymph nodes. When thyroid surgery is performed by experienced surgeons, inadvertent parathyroidectomy may be as high as 9%. 1 Abnormal parathyroid glands may be concealed beneath the thyroid capsule, intrathyroid, intrathymic, or inside the carotid sheath. Other ectopic locations in the neck or anterior mediastinum are also encountered. Furthermore, the distinction between true double adenomas and asymmetric hyperplasia continues to challenge even the most seasoned endocrine surgeon.
It has been argued that with the exception of a mediastinal parathyroid adenoma, localizing studies (eg, technetium-99m-sestamibi [Tc-MIBI] imaging, MRI, CT, and ultrasound [US]) add little to the overall success of parathyroidectomy, especially for primary explorations in the hands of experienced endocrine surgeons. However, for the less experienced surgeon, preoperative localization studies have been helpful in directing the side of the neck for initial exploration, and for reducing operative times and frustration. Revision parathyroidectomy, after a failed initial neck exploration, can be an exercise in futility without some form of localizing study, the cost of which is then always justified. Recent extramural pressures to perform “minimally invasive surgery,” limiting both the scope and duration of parathyroidectomy and reducing hospital length of stay, have popularized the use of preoperative parathyroid localizing studies. Over the past decade, Tc-MIBI imaging has become the “gold standard” for preoperative localization because of its high sensitivity and specificity, and its use has become routine in many centers. Intraoperative procedures such as Tc-MIBI localization using a hand-held gamma probe, intraoperative circulating iPTH assay (Nichols Institute Diagnostics, San Juan Capistrano, CA, USA), have evolved to permit a more limited “minimally invasive” unilateral neck exploration. However, this approach is limited to patients for whom a preoperative Tc-MIBI strongly suggests the presence of a single adenoma. Even with this positive finding, Tc-MIBI will miss double adenomas and asymmetric four-gland hyperplasia in a significant number of patients. The additional radiation exposure to patient and personnel with radioguided surgery, the need for more than one scan, and complex scheduling issues for appropriate timing of the radiopharmaceutical administration may represent other disadvantages.
In their search for a better intraoperative localizing technique, Klopper and Moe 2 in 1966 discovered the ability of a toluidine blue dye infusion to selectively stain normal parathyroid tissue in dogs. This was corroborated two years later in man by Hurvitz et al. 3 Initial enthusiasm for this technique soon waned because of its toxicity (arrhythmia and cardiac arrest). In 1971, Dudley 4 first reported the successful use of an intraoperative infusion of another thiazin dye, variably called methylthionine chloride, tetramethylthionine chloride, or methylene blue, for the rapid identification of parathyroid tissue. Unlike toluidine blue, methylene blue caused no cardiac toxicity or other adverse effects when a dose of 5 mg/kg was infused one hour prior to neck exploration. Since then numerous other investigators have confirmed the utility and safety of the technique, even at higher doses (7.5-10 mg/kg).
The exact physiologic mechanism for selective staining of enlarged and/or hypercellular parathyroid tissue is poorly understood. Lavelle 5 reported one case of a parathyroid adenoma that only partially stained dark blue with an IMBI. Histologic evaluation of the stained versus unstained areas revealed a predominance of oxyphil cells rich in mitochondria, compared to either chief cells or clear cells respectively. It has been proposed that the uptake and selective retention of Tc-MIBI within parathyroid adenomas also occurs within mitochondria. Both methylene blue and Tc-MIBI are lipophylic cations and may more readily diffuse through the mitochondrial cell membrane without a specific transmembrane transporter. Westreich et al 6 found an increased oxyphil content in adenomas for which Tc-MIBI scans were positive. Accumulation within the mitochondrial matrix may explain this selective retention of the two agents. Orloff 7 found that 6 diseased parathyroid glands that failed to concentrate Tc-MIBI also failed to concentrate methylene blue. Other investigators have postulated that the differential uptake and retention of these agents are influenced by differences in vascularity between enlarged and normal parathyroid glands with further variations caused by the total dose, timing, and velocity of the infusion. The effectiveness of the dose of methylene blue and the rate of administration have not been entirely evaluated, and there are some differences of opinion. Rowntree 8 found that most of the IMBI failures occurred in thin women and heavy men. They postulated that since fat was not stained compared to muscle, that better results would be achieved with a calculated dose of methylene blue based on lean-body weight. Sherlock et al 9 concluded that a higher dose of methylene blue was needed (7.5 to 8.5 mg/kg) based on lean-body mass, with the higher dose needed for leaner patients. A longer infusion time of 2 hours was also felt to give more uniform and prolonged staining of the parathyroid glands. Muslumanoglu et al 10 found that best staining occurred when the IMBI was given 1 hour before anesthesia induction and with 40% of the solution given in the first 30 minutes and the remainder in the last 30 minutes. In contrast, Gavilan et al 11 found that in the few cases where staining was unsatisfactory, the infusion had been performed slowly. They recommended initiation of the infusion immediately following induction of general anesthesia and completion within 15 minutes. Traynor et al 12 attempted to establish an ideal timing and velocity of IMBI in a canine model. Maximum uptake of methylene blue occurred between 20 and 30 minutes after completing the infusion, with washout diminution first noticed 20 to 73 minutes later. The rate of infusion did not affect staining. Only 7 published reports in the United States have documented an experience with an IMBI in parathyroid surgery.
The purpose of this communication is to retrospectively review a single surgeon's experience with the technique of IMBI for the rapid identification of parathyroid tissue in 35 patients who were treated for primary hyperparathyroidism by bilateral neck exploration and parathyroidectomy.
MATERIALS AND METHODS
Between June 2000 and August 2003, 47 patients with primary hyperparathyroidism underwent bilateral neck exploration with parathyroidectomy for the initial treatment of primary hyperparathyroidism. During this period, 35 patients were given an IMBI to help identify parathyroid tissue. Patients with significant cardiac disease or other serious co-morbidities were excluded from the use of an IMBI because of our early concerns regarding pseudocyanosis and unreliability of pulse oxymetry monitoring. All patients gave informed consent with detailed knowledge about the use of an IMBI. The same surgeon performed all surgery under general anesthesia. IMBI was administered at a calculated dose of 7.5 mg/kg (1% methylene blue injection, USP, 10-mL vials, 10 mg/mL; American Regent Laboratories, Inc., Shirley, NY) diluted in 250 to 500 cc of normal saline. The infusion was administered over a mean period of 17 minutes (range, 15-30) immediately following endotracheal intubation and secure patient positioning. The anesthesiologist was alerted to the phenomenon of pseudocyanosis resulting from the IMBI and the possibility of pseudohypoxia as registered by pulse-oxymetry. In general, the incision was made after completion of the IMBI. In the few patients for whom the incision was made before this, the blood appeared darker than usual but there was no staining of the soft tissues of the neck. A bilateral exploration was performed in all patients with the goal of finding 4 parathyroid glands. Once one or more enlarged parathyroid glands were identified, they were removed and a minimum of one normal-appearing gland was biopsied. Both size of the gland and the intensity of staining with methylene blue determined which glands were removed.
RESULTS
There were 27 women (77%) and 8 men (23%). Ages ranged from 37 to 80 years (mean age, 57). All patients had hypercalcemia and elevated intact parathyroid hormone levels (iPTH) relative to the serum calcium level, sufficient to confirm the diagnosis of primary hyperparathyroidism. The mean preoperative serum calcium was 11.3 mg/dL (range 10.6-13.3). iPTH levels ranged from 58 to 367 pg/mL. None of the patients had a history to suggest a multiple endocrine neoplasia syndrome or familial hyperparathyroidism. Preoperative localizing studies were variably performed by referring physicians and included Tc-MIBI imaging (in 32/35 patients), US (in 20/35 patients), CT (in 4/35 patients), and MRI (in 2/35 patients). US, CT, and MRI were generally obtained after a negative Tc-MIBI study to further help identify the initial side for exploration in the case of a single parathyroid adenoma, or to anticipate four-gland hyperplasia. In 2 patients, an initial US clearly identified a single adenoma separate from the thyroid gland and no further studies were deemed necessary.
At least one abnormal parathyroid gland was identified in all 35 patients explored. Nine patients had coexistent preoperative thyroid disease and underwent partial thyroidectomy. There were 2 papillary carcinomas and the remainder were either benign adenomas or hyperplastic nodules.
There were 30 patients with a single adenoma (85.7%), 4 with double adenomas (11.4%), and 1 with four-gland hyperplasia (2.9%). All abnormal parathyroid tissue was confirmed by histopathology. All but one of the double adenomas had a compressed rim of normocellular parathyroid tissue. One patient with a single parathyroid adenoma had a total of 5 histologically confirmed glands. At least one half of a single, normal gland equivalent was left intact with a viable blood supply in one patient with four-gland hyperplasia.
Methylene Blue Staining
The mean total administered dose of methylene blue was 618 mg (range, 375-890). All but one of the single adenomas stained with methylene blue (97%). Among the total number of adenomas that stained (37, including double adenomas), 33 glands were observed to stain dark blue to purple in color (89%) (Figs 1 & 2). Four adenomas stained a less intense shade of blue or had a greenish-blue/teal color. All of the 4 less intense staining adenomas were in thin males. In nearly every case, all stained adenomas were easily identified beneath several fascia layers immediately after rotating the thyroid gland away from the tracheoesophageal groove. In 2 patients, the adenoma was deeply positioned behind the common carotid artery; in another patient it was within the thymic tongue inferiorly. However, all were easily identified due to methylene blue staining. There was also 1 mediastinal parathyroid adenoma, which had been identified by preoperative Tc-MIBI scanning. This gland was situated inferior to the inominate artery, stained deep blue (Fig 3), and was easily distinguished from the surrounding thymic tissue. Unequivocal fourgland hyperplasia was encountered surprisingly in only 1 patient and may represent a skew caused by the small number of patients in this series. The hyperplastic glands all stained with methylene blue, albeit to a lesser degree than the adenomas. The hyperplastic glands, even when only slightly enlarged, were more saturated with pigment compared to normal glands, which stained very lightly or not at all. In this series, 89 normal glands were identified out of a possible 98 (90.8%), with the assumption of all patients having at least 4 parathyroid glands. Of the 89 normal glands, only 41 (46%) were visibly stained with methylene blue. All but one of the 41 glands took on a pale, greenish-grey hue (Fig 4). One histologically normal gland (normal cellularity with abundant stromal fat) stained deeply blue but was clearly enlarged (1.2 cm) and therefore removed. Normal glands that did stain were quickly identified, especially small suppressed glands, which otherwise would have likely taken longer to find. In many cases, just rotating the thyroid lobe away from the tracheoesophageal groove allowed identification of 2 normal parathyroid glands. As experience with this technique accrued, the need to biopsy normal glands was reduced, since nonstained or very light staining glands were always normal. In the majority of cases, the thyroid gland became a darker than normal color and cysts/colloid nodules also stained to varying degrees. Lymph nodes also occasionally stained a light slate blue color. However, in no situation did the minimal staining characteristics of nonparathyroid tissues cause confusion, because of their differing morphological features and location.
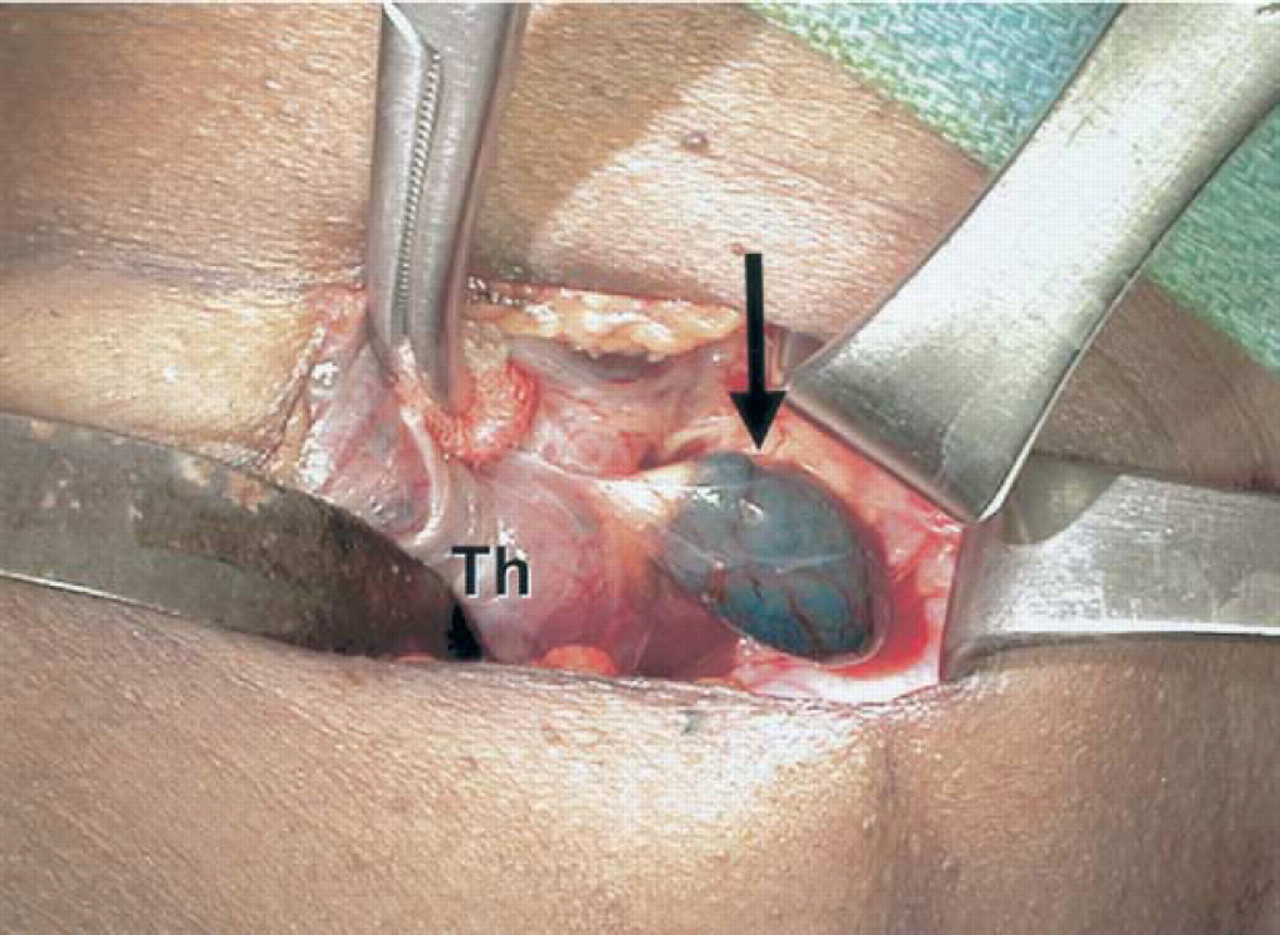
Intraoperative photograph demonstrating intense staining of a parathyroid adenoma (black arrow) following an IMBI. Th, thyroid gland.
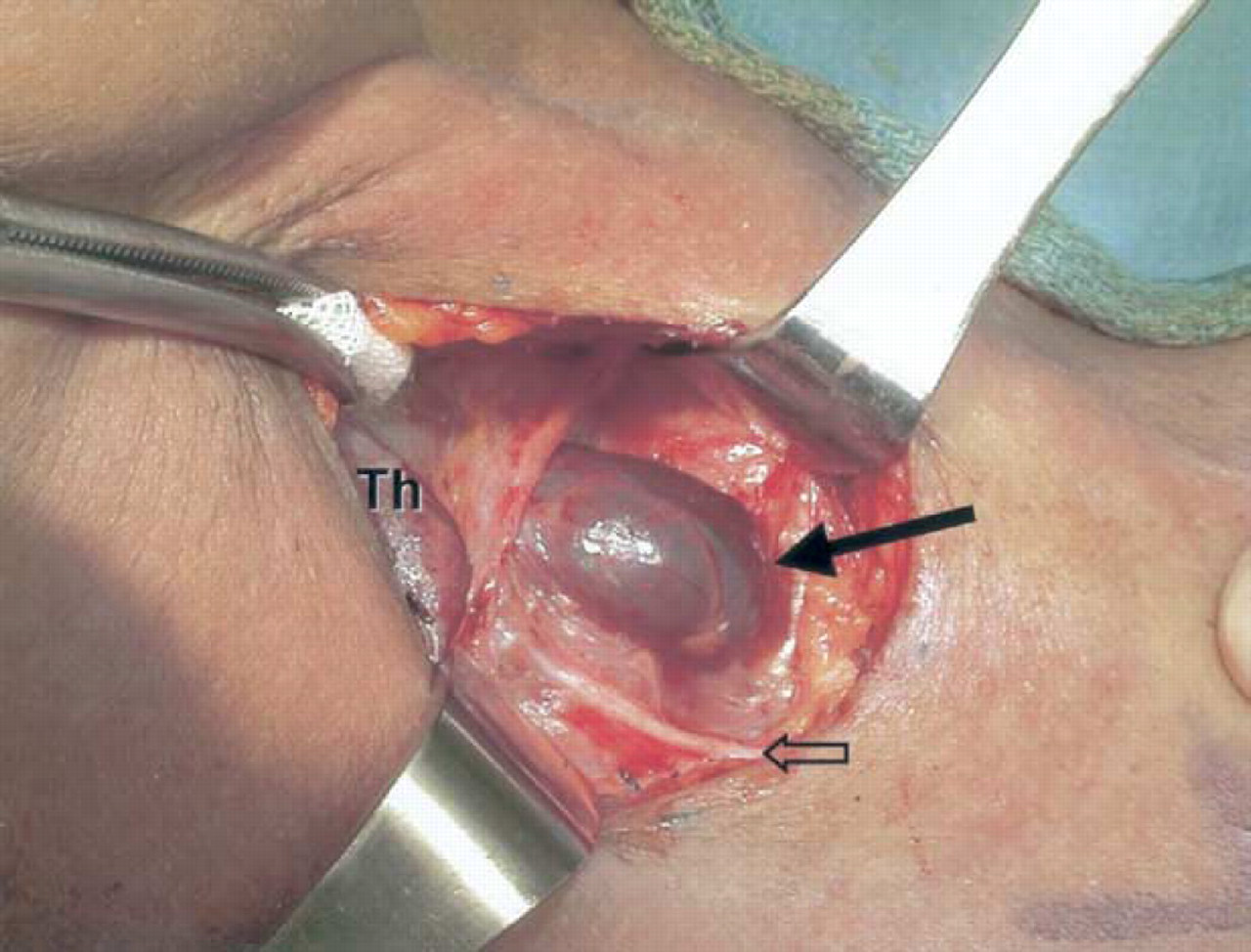
Intraoperative photograph demonstrating intense staining of a parathyroid adenoma (solid black arrow) following an IMBI. Open arrow points to recurrent laryngeal nerve. Th, thyroid gland.
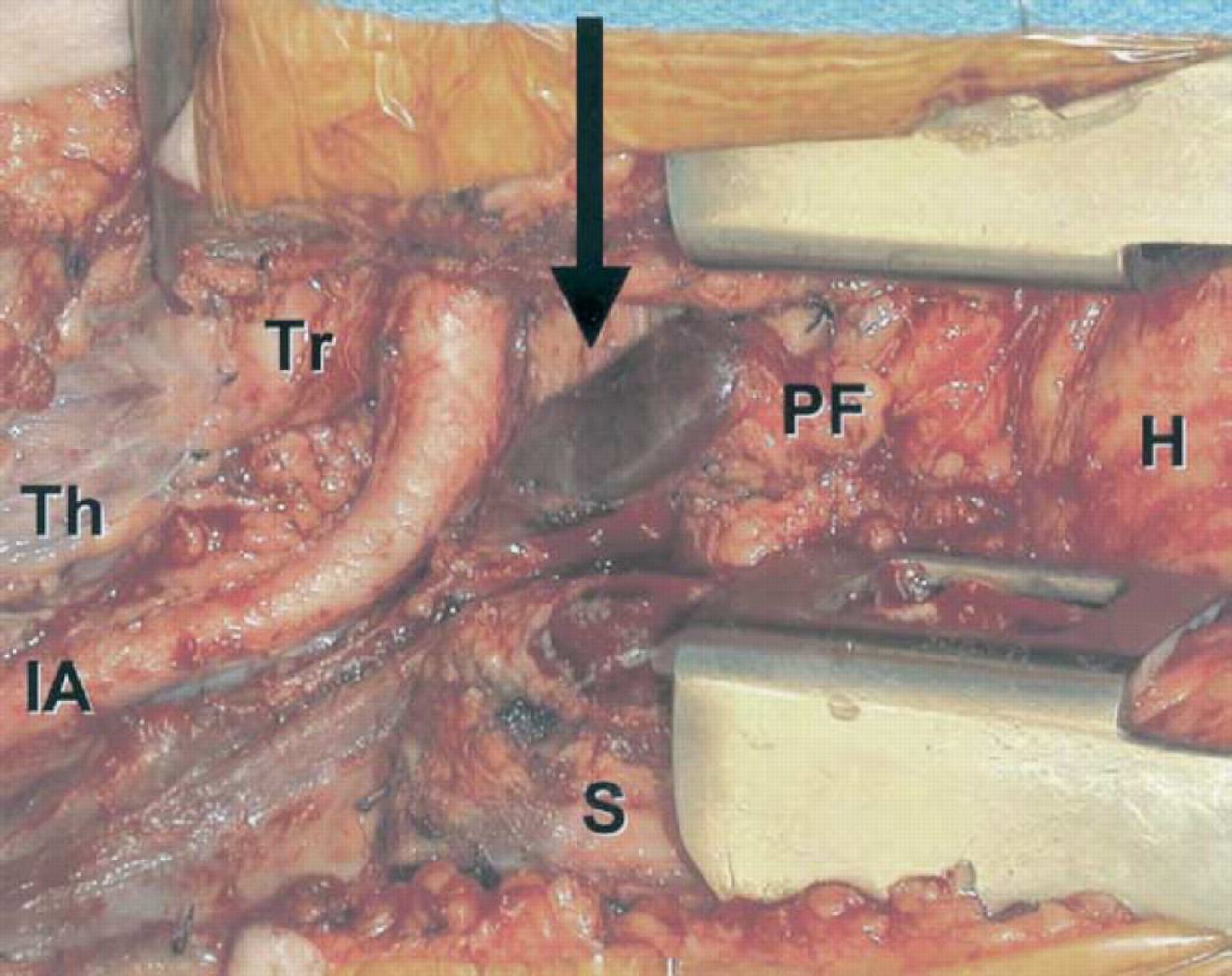
Intraoperative photograph demonstrating intense staining of a large mediastinal parathyroid adenoma (black arrow) following an IMBI. Tr, trachea; Th, thyroid gland; IA, inominate artery; PFk, pericardial fat; H, heart; S, sternum (split).
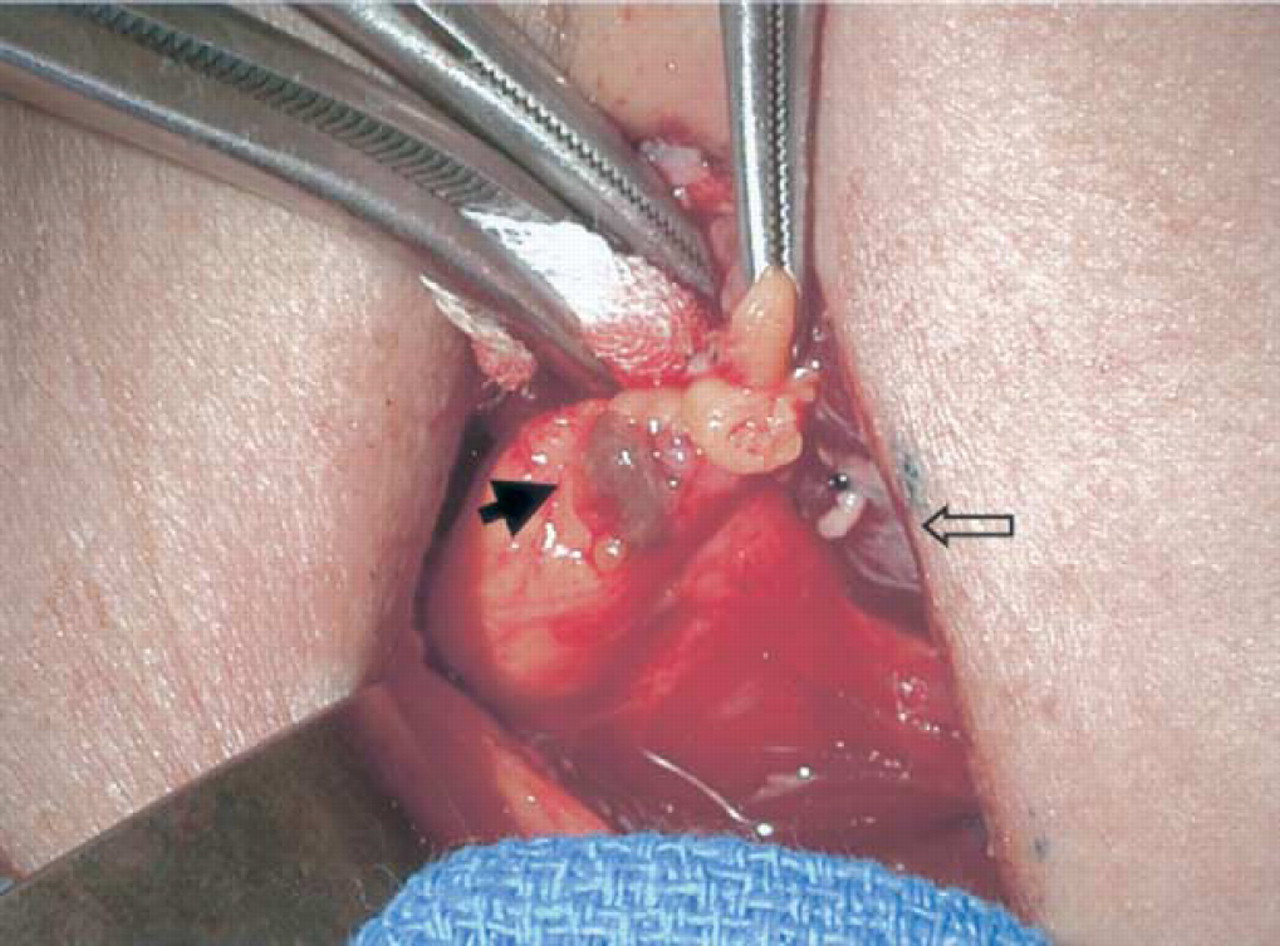
Intraoperative photograph demonstrating grey-green staining of a normal parathyroid gland (solid black arrow) following an IMBI. Open arrow points to thyroid gland.
Preoperative Localizing Studies
All 4 of the patients with double adenomas had preoperative Tc-MIBI studies. In 1 patient, the Tc-MIBI imaging missed both adenomas and only 1 adenoma was detected by a second study utilizing MRI. In each of the 3 other patients with a double adenoma, only 1 of the 2 pathologic glands were detected by Tc-MIBI imaging.
Biochemical Results
Serum calcium determinations were made postoperatively at approximately 8-hour intervals until stable. In all 35 patients, the serum calcium level was normal or slightly low prior to hospital discharge. To date, all 35 patients (100%) have sustained normocalcemia with a mean follow-up period of 17 months (range, 1.5-39). Three patients have mildly elevated iPTH levels despite continued normocalcemia at 18.2, 13.3, and 10.7 months respectively. In all 3 patients, the persistent, albeit lower, iPTH levels postoperatively were attributed to some degree of secondary hyperparathyroidism. Two patients were found to have a vitamin D deficiency, one with a previously unrecognized malabsorption syndrome. One other patient, with stable normocalcemia, has an unexplained mildly persistent iPTH elevation and continues to be monitored.
Pseudohypoxia and Pulse Oxymetry
Pulse oxymetry data was obtained from computerized anesthesia records using Compurecord software (ARI-Agilent Technologies, Pittsburgh, PA) and tabulated on a Microsoft Excel spreadsheet for analysis. Several minutes following the infusion of methylene blue, pseudohypoxia occurred to a variable degree as measured by pulse oxymetry. In 2/35 patients, the SP02 remained above 90%. Overall, the mean nadir SP02 reached was 65% (range, 31-96%). The lowest measured SP02 following a IMBI was 31%. The time to reach the nadir SP02 was a mean of 10.84 minutes (range, 2.0-25.75). The mean time for the SP02 to return back to baseline was 14.93 minutes (range, 4.5-90). In the first patient for whom an IMBI was used, a blood gas determination was obtained during the period of pseudocyanosis to reassure the anesthesiologist that the patient was not hypoxic. Pulse oxymetry measured an oxygen saturation of 60 to 65%, while the arterial blood gas determination measured a P02 of 178 mm Hg. In general, pulse oxymetry data begins to return to baseline once the IMBI is finished. However, in some instances, pseudohypoxia persisted long after the termination of the infusion.
Collective experience using IMBI for localizing parathyroid glands
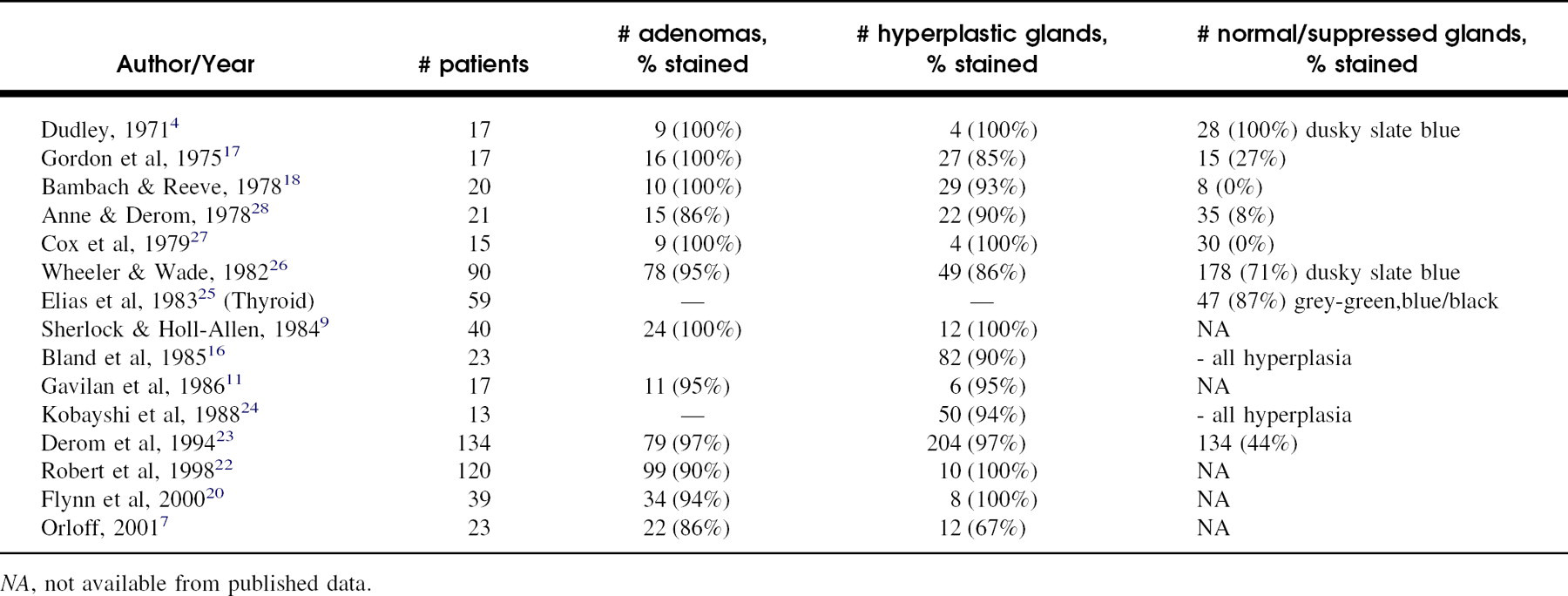
NA, not available from published data.
Complications
There were no complications or adverse effects attributable to an IMBI. Skin pseudocyanosis in Caucasians was generally subtle and normal skin tone recovered within 24 hours. Urine remained a blue-green tint for up to 10 days following the infusion of methylene blue. Gastric secretions also stained a green/blue color. All patients were warned of these effects prior to surgery. No patient required prolonged calcium or vitamin D supplementation beyond the early postoperative period.
DISCUSSION
Methylene blue is in a class of dyes called thiazins, which include toluidine blue, Azure A,B,C, and thionin. The active ingredient in methylene blue for injection is methylene blue trihydrate (3,7-Bisdimethyl-aminophenazathionium chloride trihydrate) and is occasionally referred to in the literature as methylothionine chloride or tetramethylthionine chloride. Methylene blue has been used for over a century in clinical medicine as a tissue dye as well as a treatment for methemoglobinemia and cyanide poisoning. At doses up to 10 mg/kg diluted in electrolyte solution, there have been no reported significant adverse effects or complications from the administration of this agent. In low concentrations, methylene blue is a reducing agent and therefore useful as a treatment for methemoglobinemia, whereas, at high concentrations, methylene blue induces methemoglobinemia. Induction of methemoglobinemia is one component of the immediate treatment of cyanide poisoning, since reduced hemoglobin binds free cyanide ions until more definitive therapy can be given. One single case of a methylene blue overdose (80 mg/kg), more than 10 times the recommended dose, was reported in an infant with mild renal failure. Other than intense pseudocyanosis lasting 6 days, there were no other sequellae. 13 Various studies have measured an insignificant level of methemoglobinemia. 14,15
Our experience corroborates the observation made by others, that an IMBI consistently stains parathyroid adenomas (97%), with a worldwide reported range of 86 to 100%. Hyperplastic glands stained lighter and somewhat less consistently with a reported range of 67 to 100%. The degree of staining normal/suppressed glands varies from 0 to 100% with the majority observed to be a light blue to green-grey color (Table 1). Muslumanoglu et al 10 graded the intensity of staining and found that 80% of adenomas and 75% of hyperplastic glands stained 4+ (dark blue), with the remaining adenomas and hyperplastic glands staining 3+ (sky blue). Of the normal (nonsuppressed) parathyroid glands in surgery for thyroid disease, 87% concentrated methylene blue and 57% stained 4+. In contrast, of the suppressed, normal glands associated with adenomas, 70% concentrated methylene blue but stained only 2+ (light blue) or 1+ (minimal). Bland et al 16 also reported a favorable experience using IMBI for localizing hyperplastic parathyroid glands in secondary hyperparathyroidism associated with chronic renal failure. The overall probability of hyperplastic glands staining with methylene blue was 90.1%. There was a statistically significant increased likelihood of staining with increasing serum iPTH levels, with 100% of the glands staining when iPTH levels were greater than 700 pg/ mL. Gordon et al 17 found that staining affinity for the dye was directly related to the size of the parathyroid gland.
IMBI is the only consistently reliable technique for intraoperative parathyroid localization. However, it does not obviate the need for systematic bilateral neck exploration. Even after identification, multigland disease can present a dilemma since the glands may be asymmetrically enlarged. Parathyroid glands of normal size or only slightly enlarged glands may be hyperplastic based on histologic criteria, and occasionally a slightly enlarged parathyroid gland may be entirely normal histologically, as we reported in 1 patient in this series. Therefore, the distinction between double adenomas, asymmetric hyperplasia, and diffuse hyperplasia can be difficult. Intraoperative frozen section assessment of abnormal parathyroid tissue can be misleading since normal parathyroid tissue can have areas of hypercellularity. With experience, an IMBI can guide intraoperative decision-making by relying on both the size of the gland(s) and staining characteristics. The intensity of methylene blue staining can help identify all abnormal glands, since normal parathyroid tissue either does not stain or stains minimally. Multiple, deeply stained glands should be regarded as pathological, regardless of size, and removed. Minimally stained or unstained glands of normal size are likely to be normal, and biopsy with the potential for devascularization should be avoided. 9,18 Normal unstained or minimally stained glands in the presence of 2 or more stained glands should be marked with hemoclips away from the vascular pedicle for future identification.
Both preoperative Tc-MIBI scanning and IMBI may serve as complementary techniques and, when used together, have been shown to significantly reduce operative time. Takei et al 19 found Tc-MIBI scanning to have a higher false positive and false negative rate compared to IMBI for localizing parathyroid adenomas. In 2 of the patients in this series with double adenomas, a second contralateral adenoma, which was not detected by Tc-MIBI imaging, was easily identified by methylene blue staining. If the Tc-MIBI scan had been relied upon for unilateral neck exploration without intraoperative parathyroid hormone assay, both patients would have required a second operation. An intraoperative methylene blue infusion was better than preoperative Tc-MIBI scans for localizing abnormal parathyroid glands in these patients. Orloff 7 found an overall 96% agreement between IMBI and Tc-MIBI. Flynn et al 20 reviewed their experience treating primary hyperparathyroidism using the combination of IMBI, intraoperative circulating iPTH assay, Tc-MIBI scan, and hand-held gamma probe for radioguided minimally invasive surgery. With this approach, hypercalcemia was corrected in 100% of their patients. Only 25% needed the contralateral neck explored when multigland disease was suspected based on iPTH assay analysis. This afforded a time savings of 42 minutes on average compared to the duration of bilateral neck exploration. Same-day discharges were possible in 15/27 (55%) patients who had minimally invasive, unilateral neck exploration. In their series, 95% of abnormal parathyroid glands stained with an IMBI, facilitating their identification.
Schell and Dudley 21 recently reported their extensive experience treating idiopathic primary hyperparathyroidism by bilateral neck exploration without any preoperative localizing studies or intraoperative circulating iPTH assay. In each patient, only an inexpensive IMBI was used to identify abnormal parathyroid glands. They reported a long-term cure rate among 688 consecutive patients of 97.7%. An analysis of their simple approach failed to show any advantage in terms of cost, overall time reduction, or biochemical success compared to the scan-directed, minimally invasive operation. Because of the significantly higher cost of preoperative Tc-MIBI scanning for all patients with primary hyperparathyroidism, no proven increase in cure rates, and marginal benefit to individual patients afforded by minimally invasive surgery, they suggested that preoperative Tc-MIBI scanning be reserved for re-operations after initial failed neck exploration. Devine et al 14 used an IMBI in the management of 30 patients undergoing re-operation for an initial failed neck exploration. In all 24 patients who were cured and found to have an enlarged parathyroid gland, it was stained blue. The authors recommended an IMBI for all cases of persistent or recurrent hyperparathyroidism.
CONCLUSIONS
While there is no substitute for a meticulous, systematic neck exploration in the management of hyperparathyroidism, markedly enhanced visibility of adenomas and hyperplastic glands in the surgical field, occurring almost immediately upon exposure, streamlines the procedure for experienced as well as less experienced surgeons. Our experience, utilizing an IMBI for rapid parathyroid gland localization during neck exploration for primary hyperparathyroidism, has been favorable and corroborates many of the observations made by our colleagues around the world. The technique is safe and reliable, and adds little to the cost of the procedure. It should be considered an important adjunct in the management of hyperparathyroidism. Its routine use is highly recommended.