
Abstract

CASE REPORT
A former 30-week premature twin male (Twin A) was intubated at birth for 4 days, and stayed in the neonatal intensive care unit (NICU) for 7 weeks. He was subsequently transferred to a step-down hospital for 2 weeks, then discharged. At 3 1/2 months of age, he presented to an emergency room with stridor and a hoarse cry. He was admitted and underwent a flexible laryngoscopy, which revealed laryngeal papillomas. He tested negative for respiratory syncytial virus. On his fourth hospital day, he deteriorated significantly, with increased respiratory distress necessitating endotracheal intubation, and was transferred to Children's National Medical Center for further management. Upon transfer, he underwent a repeat flexible laryngoscopy with the endotracheal tube still in place. This revealed papillomas in the area of supraglottis and glottis surrounding the endotracheal tube. He was taken to the operating room that evening. Microlaryngoscopy and bronchoscopy revealed papillomas of the right and left ventricles, true cords, and the anterior commissure (Fig 1). There were no papillomas noted in the distal airway. The papillomas were removed with a Xomed laryngeal microdebrider, after a biopsy was taken and sent to pathology. The patient was extubated at the end of the procedure and transferred back to the pediatric intensive care unit. He was discharged on his first postoperative day.
The parents reported that the patient's phenotypic identical twin brother (Twin B) was having similar symptoms, although less severe. His past medical history was significant for being a 30-week ex-premature infant, intubated for 4 days, a 7-week stay in the NICU, and a 2-week stay in a step-down unit. He was examined in the otolaryngology clinic and underwent a flexible laryngoscopy, which revealed a large pedunculated papilloma of the left true vocal cord. He was also brought to the operating room and underwent a micro-laryngoscopy and bronchoscopy (Fig 2). His papillomas were removed with a Xomed laryngeal microdebrider. There were no papillomas noted in his distal airway. He was discharged home on his first postoperative day.
Both patients were seen in follow-up approximately 5 weeks after the procedures. Twin A was found to have recurrence of the papillomas in the same locations, although somewhat less severe, and has required a second procedure. Twin B was found to have no recurrence and was scheduled to follow up in clinic for repeat flexible laryngoscopy in 4 weeks.
Upon questioning of their mother, she reported that she did have genital condylomas, which were treated with cauterization approximately 2 years prior to the birth of her first-born twins. She had no interval disease. During her pregnancy and at the birth of her twins, she had no evidence of condylomas and was not offered a cesarean delivery.
DISCUSSION
Juvenile onset recurrent respiratory papillomas (JORRP) are histologically benign neoplasms, although there are reported cases of malignant transformation. Papillomas often recur after removal and can cause sudden respiratory obstruction and life-threatening events. In severe cases, regrowth of the papillomas can necessitate surgical removal every 2 to 4 weeks. They generally enter remission after several years, but can persist into adulthood. JORRP usually affects the larynx, but can extend to the distal respiratory tract (trachea and lungs).
Hajek first identified the link between maternal condylomas and JORRP in 1956. 4 Further case reports and a study showed that more than 50% of mothers with JORRP children gave a history of having vaginal condylomas during pregnancy and/or at delivery. 3 Viral studies confirmed the link between JORRP and genital condylomas, when human papillomavirus (HPV) types 6 and 11 were found to be responsible for 80 to 90% of the condylomas and papillomas. 3 The transmission of the virus is believed to happen during birth when the child passes through an infected birth canal, and is further supported by studies that cesarean delivery in mothers with condylomas decreases the risk of acquiring JORRP. 5
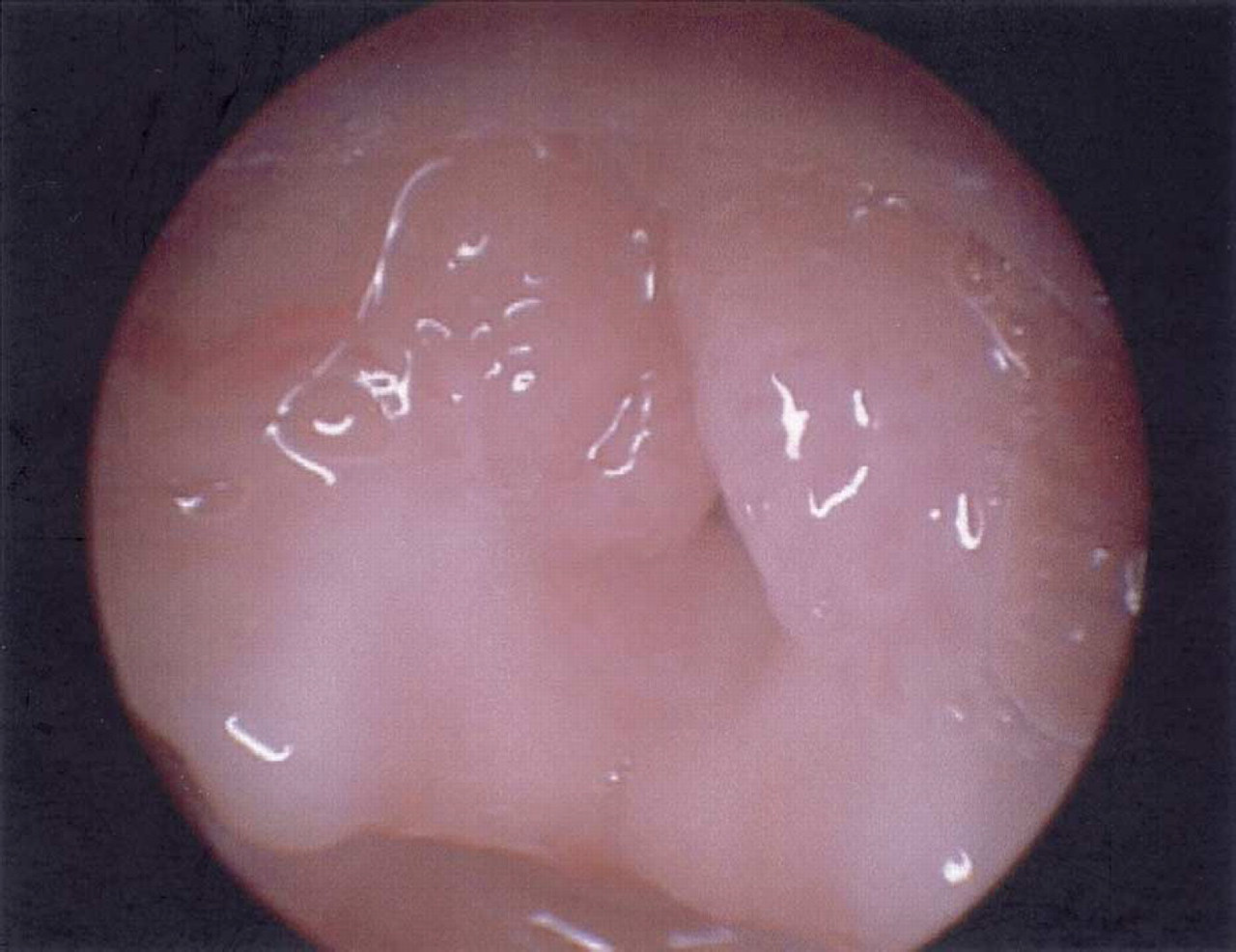
Endoscopic laryngeal papilloma picture of twin A.
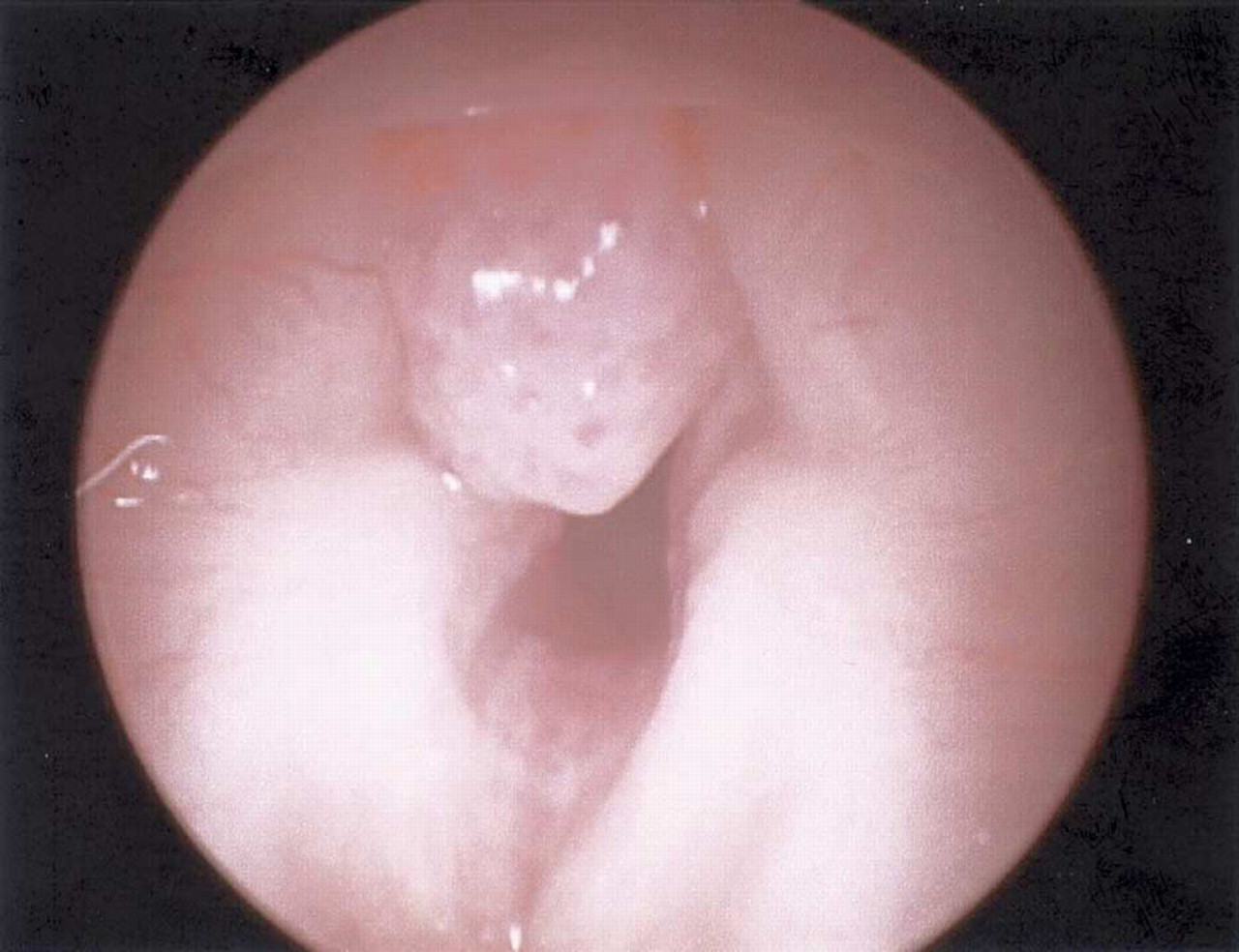
Endoscopic laryngeal papilloma picture of twin B.
The Recurrent Respiratory Papillomatosis Foundation observed that there is a triad that increases the risk of developing JORRP in children who are born to condylomatous mothers. The triad includes vaginal delivery, being firstborn, and maternal age of less than 20 years. Cesarean delivery decreases the risk by 4.6-fold, first-ordered birth increases the risk by 1.6-fold, and maternal age less than 20 years increases the risk by 2.6-fold.3 Our first-born patient (Twin A) had more significant papillomas than the second-born child (Twin B). Their mother did have a history of genital condylomas, yet was asymptomatic during her pregnancy and delivery. The option of cesarean section was not discussed with the parents. There have not been reported cases of twins with JORRP in the English literature.
CONCLUSION
The risks and benefits of undergoing a cesarean birth should be discussed with mothers with genital condylomas. In light of the increased risk of developing JORRP, mothers with genital condylomas should be given the choice of undergoing a cesarean delivery.