
Abstract
OBJECTIVE: To determine alterations in Th2 chemokines eotaxin and monocyte chemoattractant protein-4 (MCP-4), and cytokines interleukin-5 (IL-5) and interleukin-13 (IL-13), in nasal polyps (NP) after steroid treatment.
STUDY DESIGN: Cytokine/chemokine levels were measured in NP before and after steroid therapy and compared to control sinus mucosa.
RESULTS: Twenty-one patients (control = 7, NP = 14) were enrolled. Eotaxin and MCP-4 were significantly higher than control tissue (P = 0.004 and 0.003). All four mediators decreased after steroid treatment (P < 0.03). IL-5 and IL-13 in untreated polyps were not significantly different from controls. Patients showed clinical improvement according to SNOT-20 scores (average presteroid score 19, post-steroid score 13) and endoscopic grading (1.75 each side presteroid, 1.13 poststeroid).
CONCLUSIONS: Steroids significantly decreased all cytokine/chemokine levels, but the impact on Th2 chemokines was of a much greater magnitude.
SIGNIFICANCE: Novel approaches to block inflammatory mediators, particularly Th2 chemokines, may lead to better control of nasal polyposis in the future.
Chronic hyperplastic sinusitis (CHS) with nasal polyposis (NP) represents one of the most severe forms of chronic sinusitis and has a strong tendency for recurrence in spite of aggressive medical and surgical treatment. Two of the most common forms of this disease are allergic fungal sinusitis (AFS) and eosinophilic mucin rhinosinusitis (EMRS). AFS patients exhibit Type I hypersensitivity (skin test or serology), nasal polyposis, characteristic CT scan, eosinophilic mucin, and fungus on culture or histology. EMRS may be clinically similar to AFS, but patients may not exhibit Type I hypersensitivity or have positive fungal culture/histology. Both forms have marked tissue eosinophilia and nasal polyposis and these entities may actually represent varying expressions of a similar pathophysiology that have a common final inflammatory pathway. Inflammatory cytokines and chemokines of the Th2 variety play a large role in both disease processes, resulting in marked tissue eosinophilia.
Cytokines are intracellular messengers that act as signaling molecules in an immune response and can shift the inflammatory response toward a Th1 or Th2 profile. Th2 cytokines include IL-5, which is known to stimulate the growth of eosinophils. Treatments targeting Th2 cytokines, such as anti-IL-5 antibody, have been shown to be very effective at inhibiting peripheral blood and airway eosinophils. 1 Interleukin-13 is a more recently described cytokine that has a critical role in the accumulation of intraepithelial eosinophils in chronic asthma, as well as in epithelial and subepithelial remodeling. 2 Additionally, elevated mRNA production of IL-13 has been found in patients with allergic rhinosinusitis. 3 These cytokines probably play a large role in the tissue eosinophilia seen in AFS and EMRS.
Chemokines are groups of cytokines that share the ability to induce movement and direction in leukocytes. They may also exhibit properties of other cytokines, including degranulation, differentiation, and activation of cells. 4 These proteins are an essential part of the immune system and are vital in inflammatory responses. Two prominent Th2 chemokines include eotaxin and monocyte chemoattractant protein-4 (MCP-4). Eotaxin induces chemotaxis in eosinophils, basophils, and Th2 subset lymphocytes as well as affecting migration, release of reactive oxygen species, calcium mobilization, and actin polymerization in eosinophils. 5 MCP-4 recruits eosinophils, induces histamine release from basophils, and raises free cytosolic calcium levels in eosinophils. 6
Clinically, the most effective pharmacological agents for nasal polyposis are systemic corticosteroids, which cause a decrease in mucosal inflammation and broadly suppress the immune response directed against environmental irritants and bacterial/fungal antigens. Most patients with chronic hyperplastic sinusitis generally experience temporary improvement of their symptoms when treated with systemic steroid therapy. Steroids have wide-ranging anti-inflammatory properties which appear to be related to their potent effects on leukocyte circulation and function. 7-9 A better understanding of the cytokine/chemokine pattern in CHS/NP before and after steroid therapy will improve our understanding of the pathophysiology and may identify key mediators in AFS and EMRS.
The hypothesis of this study was that Th2 cytokines and chemokines would be elevated in nasal polyposis associated with AFS and EMRS compared to normal controls and these inflammatory profiles will return toward normal after systemic steroid treatment. Additionally, we correlated changes in cytokines/chemokine profiles to clinical parameters, including endoscopic examination and grading, radiographic staging, and clinical outcomes using the Sino-Nasal Outcome Test (SNOT-20). 10
MATERIALS AND METHODS
Clinical Evaluation
We obtained Institutional Review Board approval for this study. Study patients were 18 years old or over with a history of allergic fungal sinusitis (AFS) or eosinophilic mucin rhinosinusitis (EMRS) refractory to standard medical management, but with normal overall health without being treated for any major medical disorder other than sinus or associated pulmonary disease. Patients receiving oral steroid therapy, anti-fungal medications, or immunotherapy within the preceding 4 weeks or those with a contraindication to oral steroid use were excluded from the study. An additional exclusion criterion was nasal polyposis due to other known causes, such as cystic fibrosis or aspirin triad. Control patients were free of sinusitis and undergoing surgeries such as encephalocele/CSF leak repairs or benign tumor removal. The diagnosis of AFS was made when patients met all of the following criteria: 1) type I hypersensitivity (skin test or serology), 2) nasal polyposis, 3) characteristic CT, 4) eosinophilic mucin without fungal invasion, and 5) fungi present on culture or histology. Patients who did not meet these diagnostic criteria were included in the EMRS group.
Patients underwent endoscopic examination of both nasal cavities following topical anesthesia and decongestion. The degree of polyposis was semi-quantitatively graded endoscopically by determining their relationship to fixed anatomic landmarks as previously described. 10 In this scale 0 = no polyposis seen, 1 = polyps within middle meatus, and 2 = polyps outside of the middle meatus. Polypoid mucosa in the middle meatus/anterior ethmoid/maxillary sinus regions was then biopsied using straight or angled forceps under direct endoscopic vision.
Patients were asked to evaluate their clinical symptoms by completing the SNOT-20 questionnaire before and after their course of steroids. Sinus disease was treated with oral prednisone (60 mg daily for 3 days, 40 mg daily for 3 days, 30 mg daily for 3 days, 20 mg daily for 12 days. Upon conclusion of the 3-week taper, a repeat sinus mucosal biopsy was performed. Posttreatment biopsies were performed in CHS/NP patients in the same general sites as performed initially and endoscopic grading was repeated to evaluate poststeroid NP response. If the patient was an appropriate surgical candidate and desired surgical treatment, the posttreatment biopsy was performed in the operating room as part of standard endoscopic sinus surgery. If the patient was not a surgical candidate or did not desire surgery after completion of the prednisone taper, the posttreatment biopsy was performed in the Otolaryngology Clinic during routine follow-up in the manner previously described.
Cytokine/Chemokine Analysis
Biopsy specimens were frozen at −70°C until homogenization. The tissue was assigned a number for blinding purposes for the remainder of the experiment. Tissue was thawed, and 1 mL of homogenization buffer (10 mM Hepes, 137 mM NaCl, 4 mM KCl, 11 mM glucose, 2 mM phenlymethylsulphonyl fluoride, 1 uM aprotinin, 1 uM pepstatin, 1 mM EDTA, and 0.1% soybean trypsin inhibitor at pH 7.2) was added to several pieces of sinus tissue. The tissue was then homogenized for 3-4 minutes. The resultant homogenate was centrifuged at 5000 rpm and 4°C for 20 minutes. The total protein concentration of the homogenates was determined using the Bradford method with the Coomassie protein assay kit (Bio-Rad Laboratories, Hercules, CA). 11 The homogenate supernatants were pipetted into individual 100-microliter aliquots and stored at −70°C until used for cytokine/chemokine assays. IL-5, IL-13, eotaxin, and MCP-4 assays were performed using standard ELISA kits (R&D systems) available for quantification of specific cytokine/chemokine levels. Subsequent data is expressed as picograms of cytokine or chemokine per milligram of total protein.
Statistical Analysis
Two subject groups were used in this study: 14 subjects with nasal polyps and 7 controls. Unpaired Student t tests were used to compare differences between subject groups. CT scores were measured before treatment only. Other measurements, such as eotaxin, MCP4, IL-5, IL-13, Sino-Nasal Outcome Test (SNOT) scores, and endoscopic scores, were measured before and after treatments. Although before- and after-treatment data were paired, some missing data made the power of paired t tests smaller than the unpaired t tests. Therefore all the t tests in this report were unpaired t tests. Correlation of SNOT-20 scores to cytokine/chemokine levels was also performed.
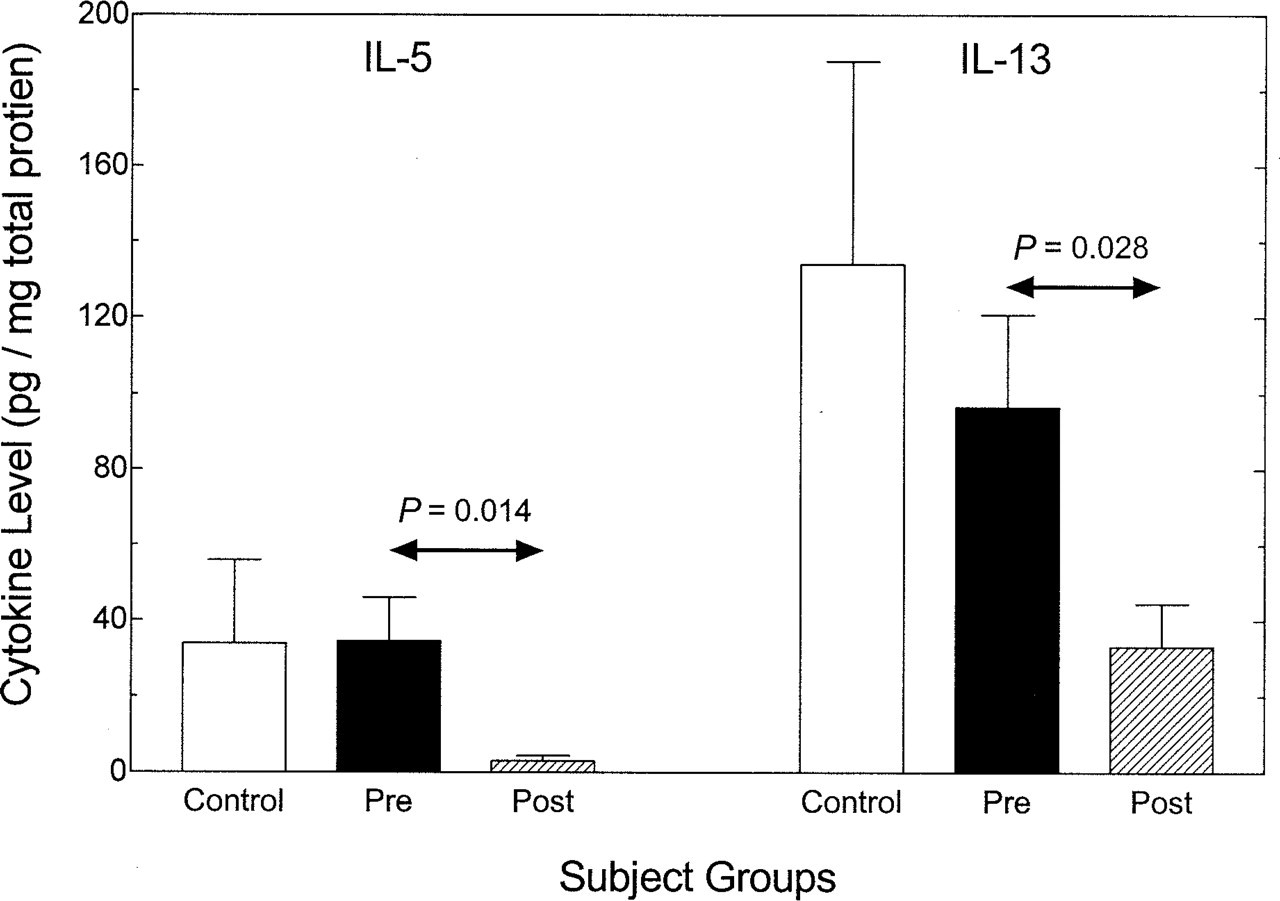
Cytokine levels before and after steroid treatment.
RESULTS
Demographics
A total of 21 patients were recruited for participation in this study. The control group consisted of 3 males and 4 females, mean age of 39 years. The nasal polyposis (NP) group consisted of 14 total patients, 11 males and 3 females, mean age of 35 years. Eight NP patients were diagnosed with AFS and 6 with EMRS.
Cytokines
Data expressed as pg of cytokine or chemokine per mg of total protein is shown in Figure 1. IL-5 levels in untreated polyps were not significantly different from the control group. After treatment with systemic steroids, there was a 10-fold reduction in IL-5 in the polyp patients (P = 0.014). Similarly, IL-13 levels in untreated polyps were not significantly different from control tissue. After treatment with systemic steroids, there was a significant threefold drop in IL-13 levels (P = 0.028).
Chemokines
Levels of Th-2 chemokines had more substantial changes (Fig 2). Eotaxin levels in untreated polyps were over 100 times that of control tissue (P = 0.004). After treatment with systemic steroids, there was a 10-fold decrease in eotaxin levels (P = 0.003). MCP-4 levels in untreated polyps were approximately 10 times that of controls (P = 0.007) and levels dropped nearly 10-fold after treatment with systemic steroids (P = 0.003).
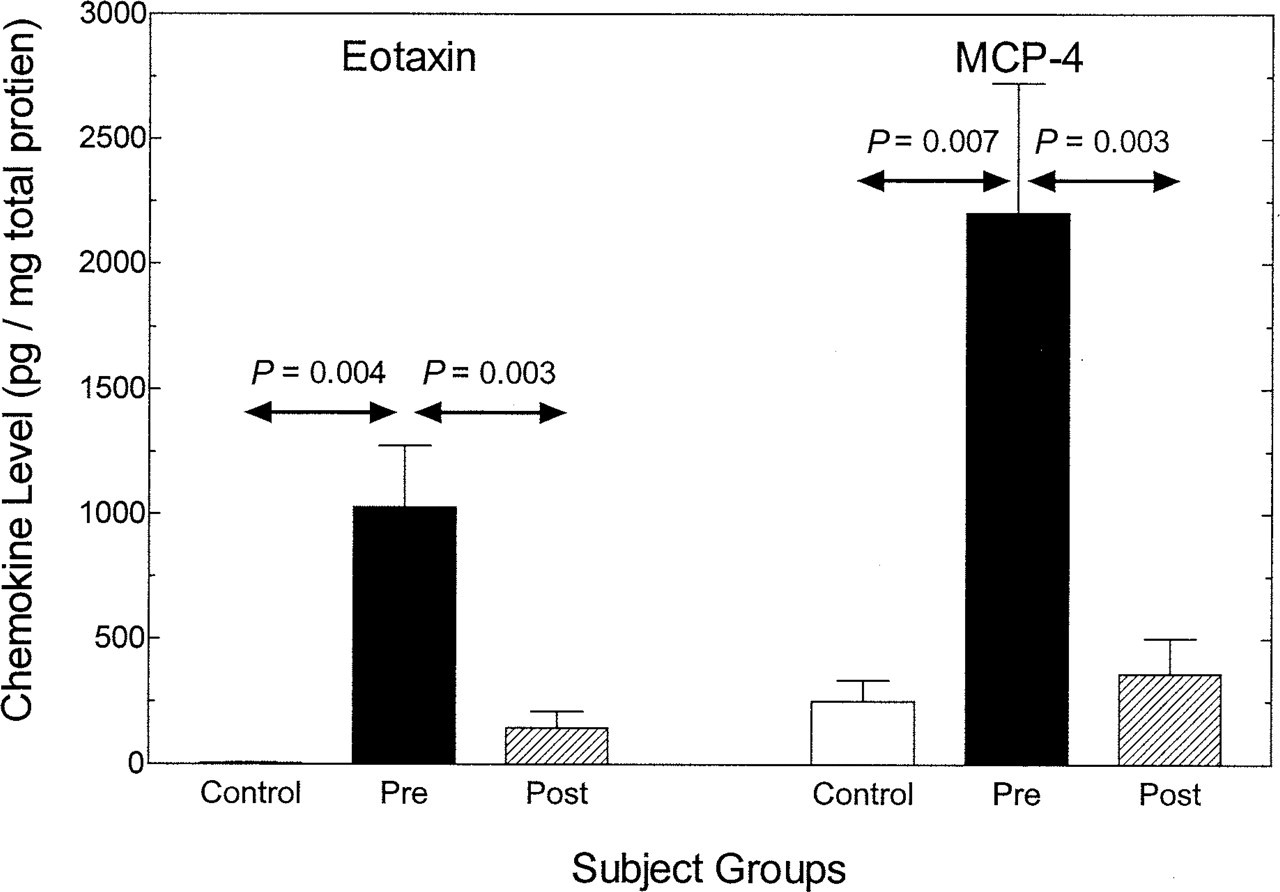
Chemokine levels before and after steroid treatment.
Clinical parameters
There were no significant differences in cytokine/chemokine levels between our AFS and EMRS patients (data not shown). Both displayed a typical Th2 response as described above. SNOT-20 scores demonstrated a marked improvement in clinical outcomes as reported by patients after treatment with systemic steroids as outlined above. However, this did not reach significance (Fig 3). The mean presteroid score was 19 (range, 10-38, 60 worst score possible) and poststeroid score was 13 (range 2-33). Using the Lund-McKay 10 scoring system for CT grading, the mean score for our polyp patients was 20.9 (range 15-24), demonstrating the severity of NP in our study. The mean endoscopic score for nasal polyposis for each side was 1.75 prior to steroid treatment (maximum score of 2), and this significantly decreased to 1.13 after steroid treatment (Fig 4).
Correlations between eotaxin, MCP4, IL-5, and IL-13 levels and the SNOT-20 score were examined. There was a tendency for SNOT-20 scores to decrease with decreasing cytokine/chemokine levels, but none of the correlations reached the statistically significant level of P < 0.05 (see Fig 5 for MCP-4 correlation). Graphs for other mediators were similar to that shown for MCP-4.
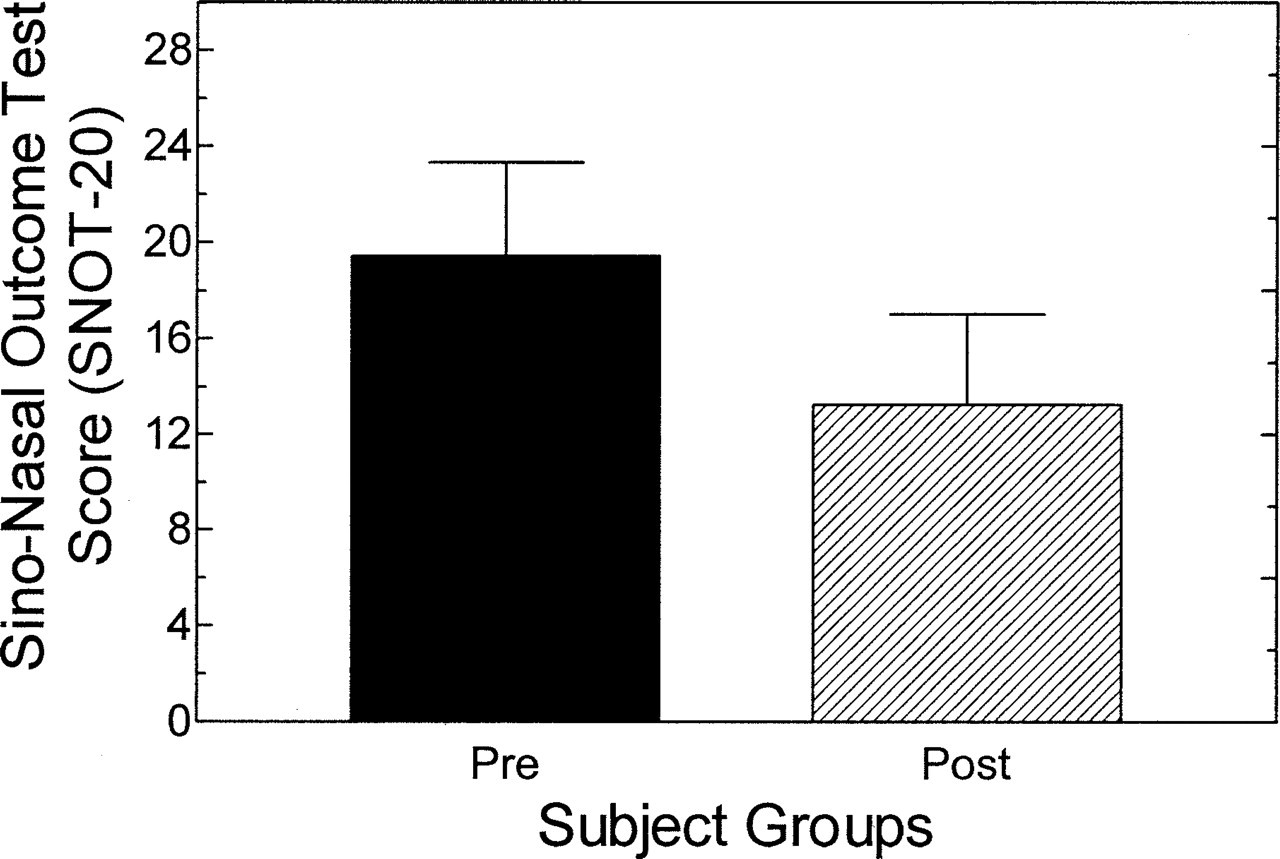
SNOT scores before and after steroid treatment. Average SNOT score declined from 19.43 to 13.22, but the difference was not statistically significant (P > 0.05).
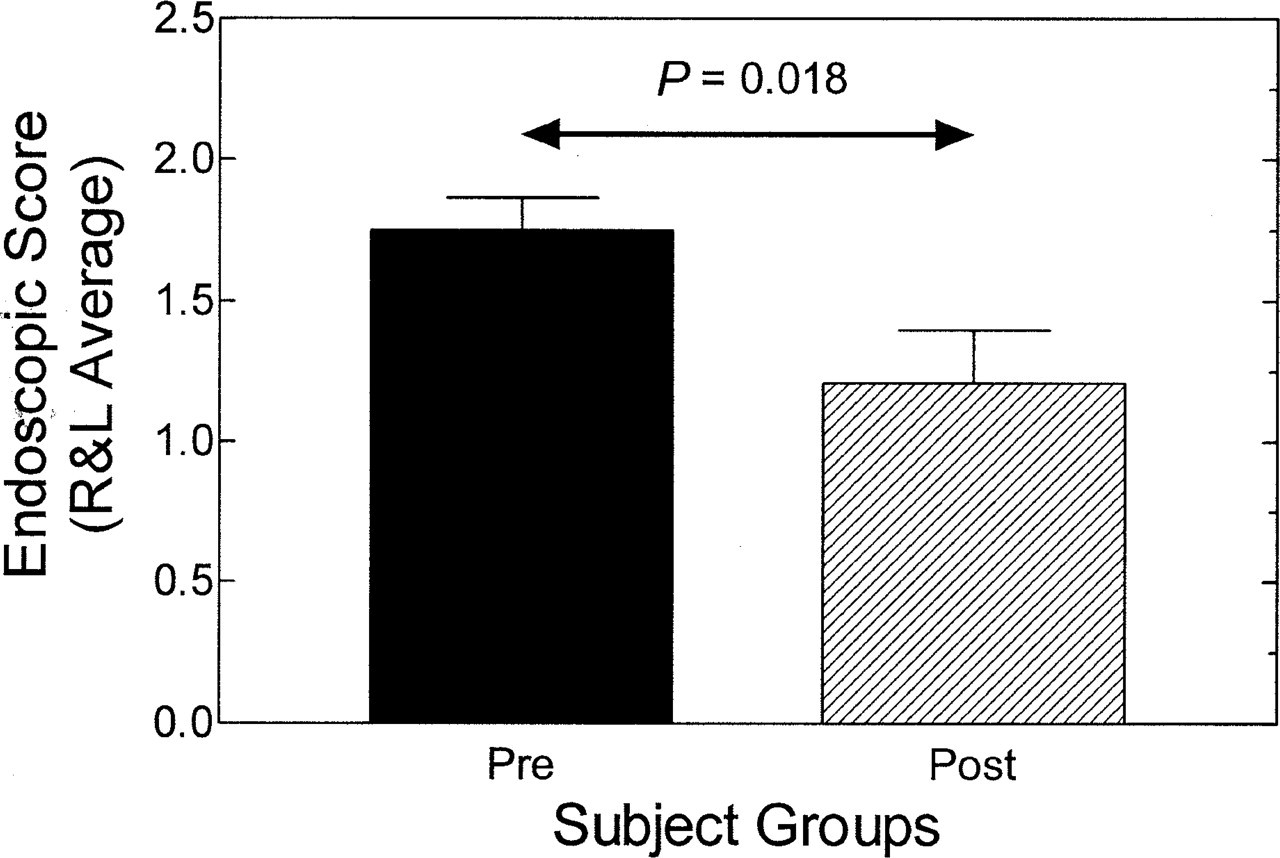
Endoscopic scores before and after steroid treatment. Average endoscopic score declined from 1.75 to 1.21.
DISCUSSION
Our study demonstrates that untreated CHS/NP has greatly elevated levels of the Th2 chemokines eotaxin and MCP-4 compared to controls, but levels of IL-5 and IL-13 similar to controls. After treatment with systemic steroids, we found significant decreases in IL-5, IL-13, eotaxin, and MCP-4. Other studies support these findings, as mRNA expression for eotaxin and MCP-4 has been shown to be significantly increased in nasal polyps compared to turbinate mucosa from the same patients. 12 In addition, tissue eosinophilia has been shown to correlate with eotaxin mRNA levels. 13 Thus, it appears that untreated NP demonstrates up-regulated transcription and/or translation of key Th2 chemokines that results in elevated production of these proteins. We also found precipitous drops in chemokine levels after administration of oral corticosteroids. Although a number of studies have shown elevated levels of Th2-type cytokines and chemokines in nasal polyps, few have addressed the effect of steroids. One study did show that systemic steroids reduce mRNA levels for eotaxin and MCP-4 in turbinate mucosa.
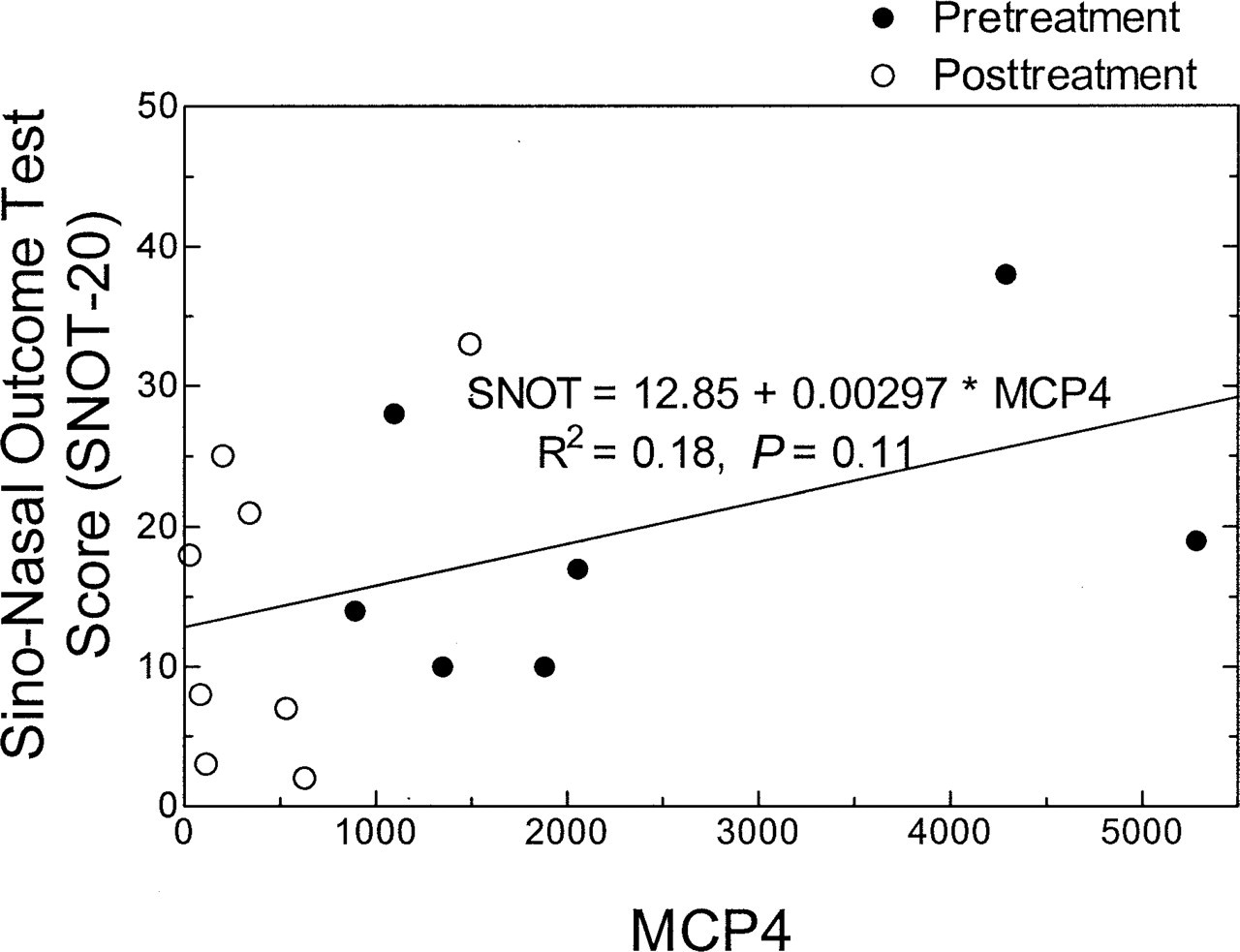
MCP-4 correlations to the SNOT-20 score. Note that levels and SNOT-20 scores declined after treatment but did not reach significance.
One unexpected finding in our study was the lack of significant difference in Th2 cytokine levels in untreated polyps vs control. Others report elevated IL-5 levels in patients with nonallergic nasal polyposis and allergic rhinitis. 14 One of the primary differences between our study and others that report an elevation of IL-5 and IL-13 is our method of normalizing cytokine/chemokine protein levels based upon mg of total protein in the specimen. This technique is more accurate than normalizing protein expression based upon the wet weight of polyp tissue that can vary significantly in water content and degree of cellularity of the specimen.
Our study also demonstrated that improvement in clinical symptoms, as evidenced by a trend in improved SNOT-20 scores, occurs after treatment with steroids. We also showed a significant decrease in mean endoscopic score. Most of our NP patients had severe disease as seen in their radiographic and endoscopic scores. Many of our untreated NP patients had polyps that extended to the floor of the nasal cavity. After steroid treatment their polyps may shrink back to the root of the inferior turbinate, but endoscopically, both pretreatment and posttreatment evaluations would receive the maximal score of 2. An even larger drop in score would be expected with a more sensitive scale.
Nasal polyposis represents a heterogeneous group of inflammatory disorders. In our study, it appears that in untreated AFS and EMRS, Th2 chemokines may play a more influential role in the eosinophilic inflammatory response than the Th2 cytokines. Our results may not apply to other etiologies, such as cystic fibrosis or aspirin triad patients. While systemic steroids significantly decreased both cytokines and chemokines, the impact on chemokines was certainly of a much greater magnitude. This may influence the effectiveness of subsequent therapies that target more specific mediators within the inflammatory cascade, as it appears that blocking the downstream chemokines may result in more improvement than inhibition of the upstream cytokines. Small-molecule antagonists for the CCR3 receptor for eotaxin are now in clinical development for the treatment of asthma. 15 Treatment of these disease processes with novel approaches to block chemokines and cytokines may lead to better control of polyps and decreased dependence on steroids in the future.
The authors would like to thank Fu Shing Lee, PhD, for his assistance with statistics.