Abstract
OBJECTIVE: Patients who undergo skull base resection after prior surgery or radiation may be at high risk for complications when local flaps alone are used for reconstruction. To determine whether the complication rate could be reduced, fasciocutaneous free tissue transfer was used to reinforce the dural closure in patients who had prior skull base surgery or radiation.
METHODS: This study is a case series of 20 patients (14 males, 6 females, aged 8–79 years of age with a mean of 47.7 years) from 1997 to 2001 who had prior skull base surgery or radiation, and underwent salvage skull base resection without large volume defects. All patients had a radial forearm free tissue transfer to reinforce the dural closure. Six patients had an osseous component to the forearm flap to provide vascularized bone to the orbital rim.
RESULTS: The overall local complication rate was 35%. Three patients (15%) had major complications including 1 case of meningitis, 1 case of cerebrospinal fluid leak, and 1 case of a flap requiring venous salvage. There were no flap failures, 1 idiopathic median nerve palsy, and no pathologic radius bone fractures.
CONCLUSION: Reconstruction with fasciocutaneous free tissue transfer for high-risk patients with low-volume dural defects following skull base resection can minimize the risk of major postoperative complications. EBM rating: C.
Factors that can influence the complication rate following skull base surgery include the size of the defect, the type of reconstruction performed, medical comorbidities, as well as previous treatment. When patients have had previous skull base surgery or radiation, there is decreased vascularity and increased scarring of the local tissues, which can lead to poor wound healing. In addition, local tissue flaps for reconstruction may not be available or reliable. Several studies have shown higher complication rates in salvage skull base cases. 2,3 In Donald's series, previous surgery was a risk factor associated with increased postoperative complications. Dos Santos et al 3 reported a significantly higher complication rate in patients who had been treated previously.
The challenge for skull base surgery is to reduce the local complication rate in patients who are at high risk as defined by having had prior skull base surgery and/or radiation. The rate of skull base surgical complications varies widely in the published literature. 1,2,4–6 The wide range is a result of variability in the way complications are tabulated, as well as variance of the population under evaluation. There can also be significant differences in complication rate depending on the type of reconstruction performed. In the study by Neligian and coworkers, 5 the overall complication rate was 38.8% for local flaps, 33.5% for free flaps, and 75% for pedicled flaps, suggesting that reconstructive approach is an important factor in reducing postoperative complications.
By definition, following skull base resection, the meninges are open to the contaminated sinonasal cavity. To reduce the incidence of postoperative infection and CSF leak, a watertight dural closure and a vascularized tissue barrier to separate the intracranial contents from the sinonasal cavity are required. There are several reconstructive options available, including local flaps, such as pericranial flaps, scalp flaps, and temporalis muscle flaps, as well as pedicled flaps and free flaps. 5,7–15 Free flaps have facilitated the advancement of skull base surgery in the past 2 decades. Free flaps can seal off the intracranial cavity and obliterate large-volume defects. Numerous studies have demonstrated an acceptably low complication rate when free flaps are used for large-volume skull base defects. 5,16 In low-volume defects, a free flap is generally not considered because local flaps perform adequately in controlling CSF leak and local infection. However, in the setting of prior surgery or radiation, local flaps may be unreliable. In this higher-risk population, a thin sheet of revascularized free tissue may prove useful in reducing surgical complications.
Specifically, the radial forearm flap was chosen because it has low donor site morbidity, a long vascular pedicle that can reach the upper neck, and permits a 2-team simultaneous resection and flap harvest. The flap is thin and pliable, and can easily fill small but complex defects of the orbitocraniofacial structures. It also can provide limited vascularized bone stock to reconstruct the upper facial skeleton. Our hypothesis was that vascularized tissue to reinforce the dural closure or pericranial flap in high-risk patients would lower the rate of major and minor local complications. This study describes our experience using the radial forearm free tissue transfer for low-volume defects following salvage skull base surgery.
MATERIALS AND METHODS
Population
This study is a prospective case series of 20 patients from 1997 to 2001 who underwent radial forearm free flap reconstruction for salvage skull base surgery. The medical records for these 20 patients were retrospectively reviewed. Patients who had prior skull base surgery or radiation therapy who underwent skull base resection with resultant low-volume defects were selected to undergo reconstruction with the radial forearm free tissue transfer. A low-volume skull base defect was classified as a defect that did not require free tissue transfer to restore volume loss; rather, the free flap acted to reinforce the dural closure and provide a reliable layer of vascularized tissue between the sinonasal cavity and the intracranial space. Eleven patients (55%) underwent a radial forearm free tissue transfer alone for dural closure, whereas the remaining 9 patients (45%) underwent a radial forearm tree tissue transfer to augment a poorly vascularized pericranial flap. A poorly vascularized pericranial flap is one that, after elevation, had dark venous blood or no evidence of bleeding. Six (30%) of the radial forearm free tissue transfers were placed solely to act as a vascularized tissue barrier between the sinonasal cavity and intracranial space. Fourteen (70%) of the radial forearm free tissue transfers were utilized for both separation of the intracranial contents as well as for local reconstruction, such as for obliterating the orbit if the patient did not wish to have an orbital prosthesis. Of these 14 patients, 6 had reconstruction of their frontal orbital bar with an osseocutaneous forearm flap. Skull base patients who had large volume defects that required a free flap were not included.
In this series, there were 14 men and 6 women. Their ages varied from 8 to 79 years of age (mean, 47.7 years). All patients had been previously treated. Three patients had previous surgery, 3 patients had previous radiation, 11 patients had previous surgery and radiation, and 3 patients had previous chemotherapy and radiation. Follow-up varied from 1 to 48 months (mean, 15.65 months). All surviving patients had at least 2 years of follow-up.
Approach
For all cases in this series, a skull base resection was felt necessary either because of direct tumor invasion, or to obtain an adequate tumor-free margin. Each case involved neurosurgery, otolaryngology, and the micro-vascular reconstructive team. At our institution, skull base tumor resection is performed via a subcranial approach. The subcranial approach, as described previously by Raveh et al, 17 offers advantages over the classic frontal craniotomy with lateral rhinotomy approach, including avoidance of frontal lobe retraction with improved exposure and cosmetically hidden incisions. Our technique for subcranial approach has been reported previously. 18 A standard bicoronal incision is used to expose the frontal-nasoglabellar complex. The supraorbital dissection is performed in either a subperiosteal or supraperiosteal plane depending on the need or availability to preserve a pericranial flap. The medial walls of the orbits and the nasal bones are skeletonized, and the anterior ethmoid artery is ligated. A limited midline bifrontal craniotomy is performed just above the frontal bar. The frontonasal complex is mobilized by making osteotomies into the right and left supraorbital foramina, the nasal bones just below the frontonasal angle and coronally up the medial and superior aspect of the orbit. The nasoglabellar complex is then removed. Removal of the nasoglabellar complex allows excellent tumor exposure, permitting en bloc resection without frontal lobe retraction. The olfactory nerve is mobilized from the cribriform only if required for oncologic resection. After tumor removal, the floor of the anterior cranial fossa is reconstructed with a pericranial flap, if available. In cases in which the pericranial flap appears unreliable, it is our practice to reinforce the pericranial flap with a free, vascularized fascial forearm flap. If the frontal bar is resected, vascularized bone is used for reconstruction. In general, our approach is to use vascularized bone along prominent areas of the orbital rim. We use this approach particularly in the previously treated patient because the tissues tend to be poorly vascularized and if vascularized bone is utilized for the reconstruction, it is our impression that the overlying soft tissue undergoes less atrophy and the incidence of plate exposure is reduced. Microplates are used to secure the nasoglabellar complex in position. If available, the pedicle of the pericranial flap is laid across the superior aspect of the nasofrontal complex. The frontal craniotomy bone flap is also secured in place with microplates. The bicoronal incision is then closed.
All reconstructions in this series involved use of a radial forearm free flap. In 6 cases, bone was harvested with the flap. The technique for radial forearm harvest has been described elsewhere, 19 but several technical points are useful to keep in mind. For cases without orbital exenteration defects, it is important to ensure that there will be adequate pedicle length for the flap to reach the upper neck and avoid the necessity for vein grafting. For cases in which the defect involves an orbital exenteration cavity and a closed orbital reconstruction is to be performed, it is first important to determine whether there is sufficient fat in the forearm for orbital volume restoration. When harvesting the fat, a very superficial, subdermal elevation is done to maximize volume and maintain the papillary dermis. To control the orbital volume so that it remains smooth and undistorted, several technical aspects should be considered. The fat must be vigorously bleeding; in general, this requires that the fat should not be disconnected from the vascular pedicle for a distance greater than 10 centimeters. The fat should not be packed into the orbit; rather, it should be rolled up snugly and sutured in position. When harvesting bone as part of an osseocutaneous forearm flap, one must consider what the ultimate position of bone relative to the skin paddle is, because there is limited flexibility of the two with respect to each other. This means that the flap inset rather than the patient's nondominant hand will dictate the side of the donor site. Rather than cutting a tangent to the cross section of the radius, a wedge of bone is removed that is centered on the attachment of the flexor retinaculum and the vascular supply from the radial artery. This approach allows for better control of the amount of bone being harvested. The two longitudinal radial osteotomies are made with a 5-mm rounded tip sagittal oscillating blade. Full-arm casting for 4 weeks is followed by 2 additional weeks of forearm casting to allow gradual loading and reorientation of the stress lines to minimize risk of pathologic radius fracture.
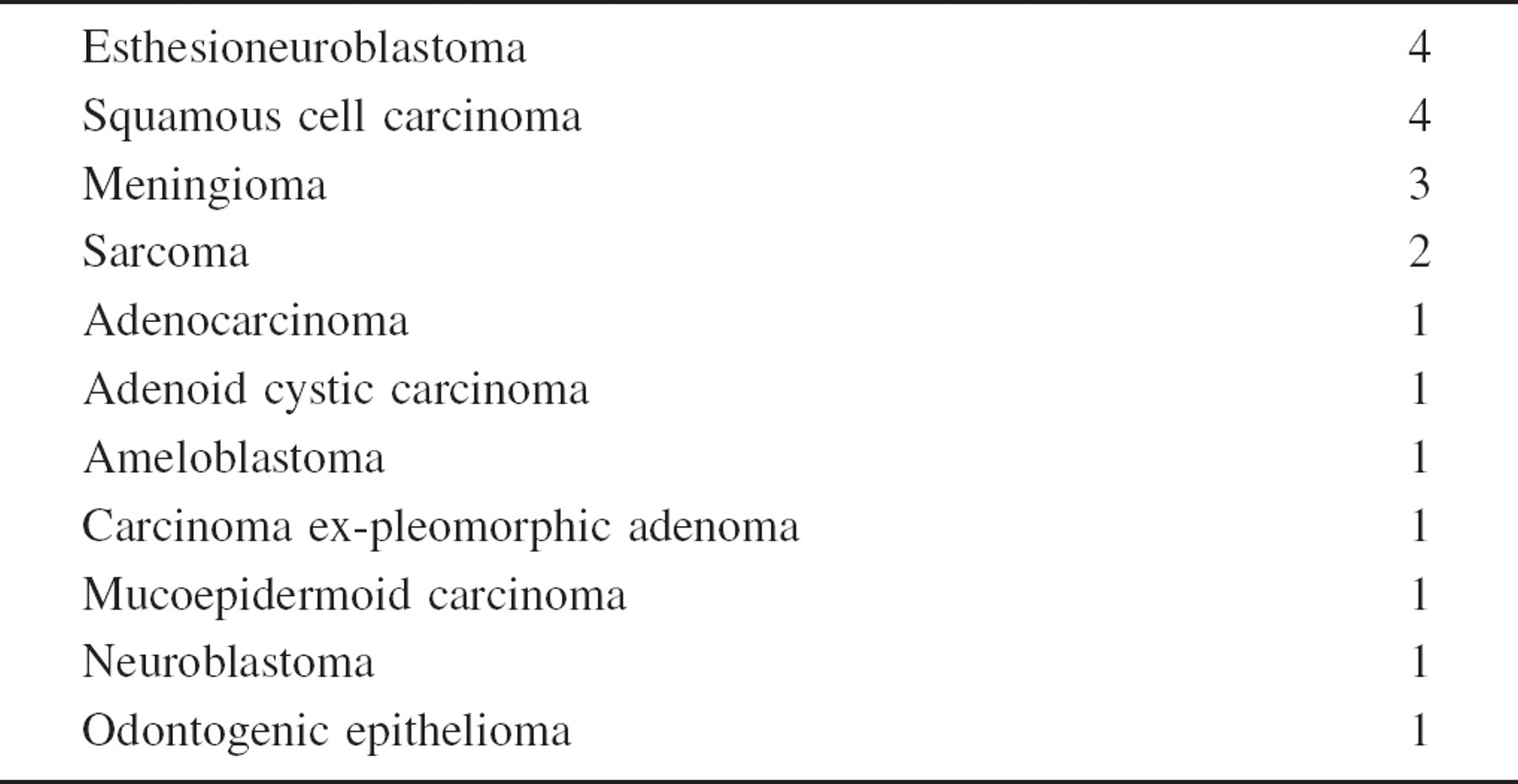
Pathology of skull base tumors
Outcome Measures
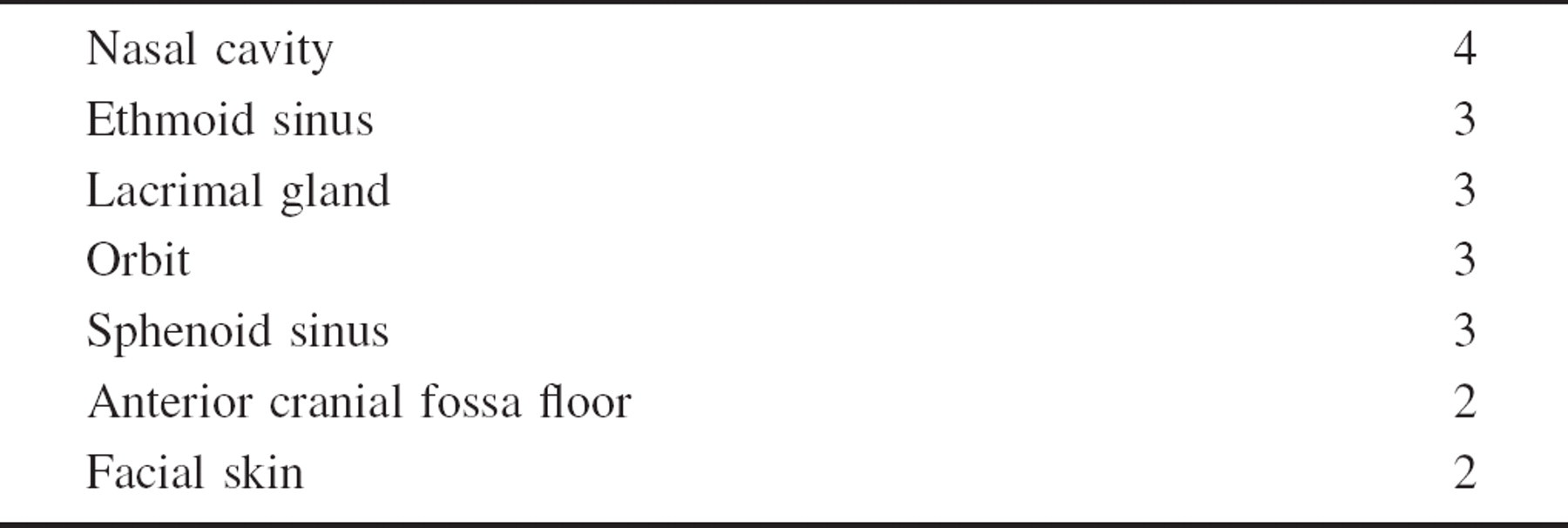
The outcome variables included local complications such as CSF leak, meningitis, pneumocephalus, wound abscess, subdural hematoma, stroke, and loss of subfrontal bone flap. Flap survival, donor site complications, tracheostomy status, length of operation, and duration of hospitalization were also tabulated. The pathology of the skull base tumors was quite varied with the most common being esthesioneuroblastoma and squamous cell carcinoma. Pathology of the tumors is shown in Table 1. Tumor sites are shown in Table 2.
We have categorized our complications into major and minor, and early and late. Major complications were those that required operative intervention, or resulted in a hospital stay of more than 17 days or readmission to the hospital within 30 days following discharge. Minor complications were self-limited, managed with local wound care, did not require operative intervention, and did not result in hospitalization stay of more than 17 days. Early complications were those that occurred less than 30 days, whereas late complications occurred more than 30 days from the date of surgery.
Statistical Analysis
Univariate data on age, gender, prior treatment, duration of operation, duration of hospitalization, flap survival, and major and minor and early and late surgical complications were tabulated. Mean, proportions, and ranges were calculated where appropriate. Comparisons were made among groups, which were categorized by type of previous treatment (surgery vs. radiation vs. chemotherapy). No significant differences were seen.
RESULTS
Complications were categorized, and these results are summarized in Table 3. Seven patients (35%) had postoperative complications, of which 3 (15%) were major complications. Of the 3 major complications, the first patient had a CSF leak noted following surgery. The patient was taken back to the operating room, where the free flap was repositioned and the CSF leak resolved. The second patient developed venous obstruction of his free flap on postoperative day 2, and the flap was successfully salvaged with vein grafts. The third patient developed a subdural hemorrhage on postoperative day 2, which required embolization of the ophthalmic branch of the carotid artery. Unfortunately, the patient had a hemispheric stroke, as well as meningitis and never recovered neurologically. This complication was a result of extensive surgical dissection of the internal carotid artery, which was required to extirpate the tumor. Of the patients, 25% (5/20) had minor complications, including 1 occurrence of pneumocephalus that resolved with conservative measures and 4 minor wound complications. The 4 minor wound complications were all treated with local measures and antibiotics.
Site of skull base tumors
Complication rate
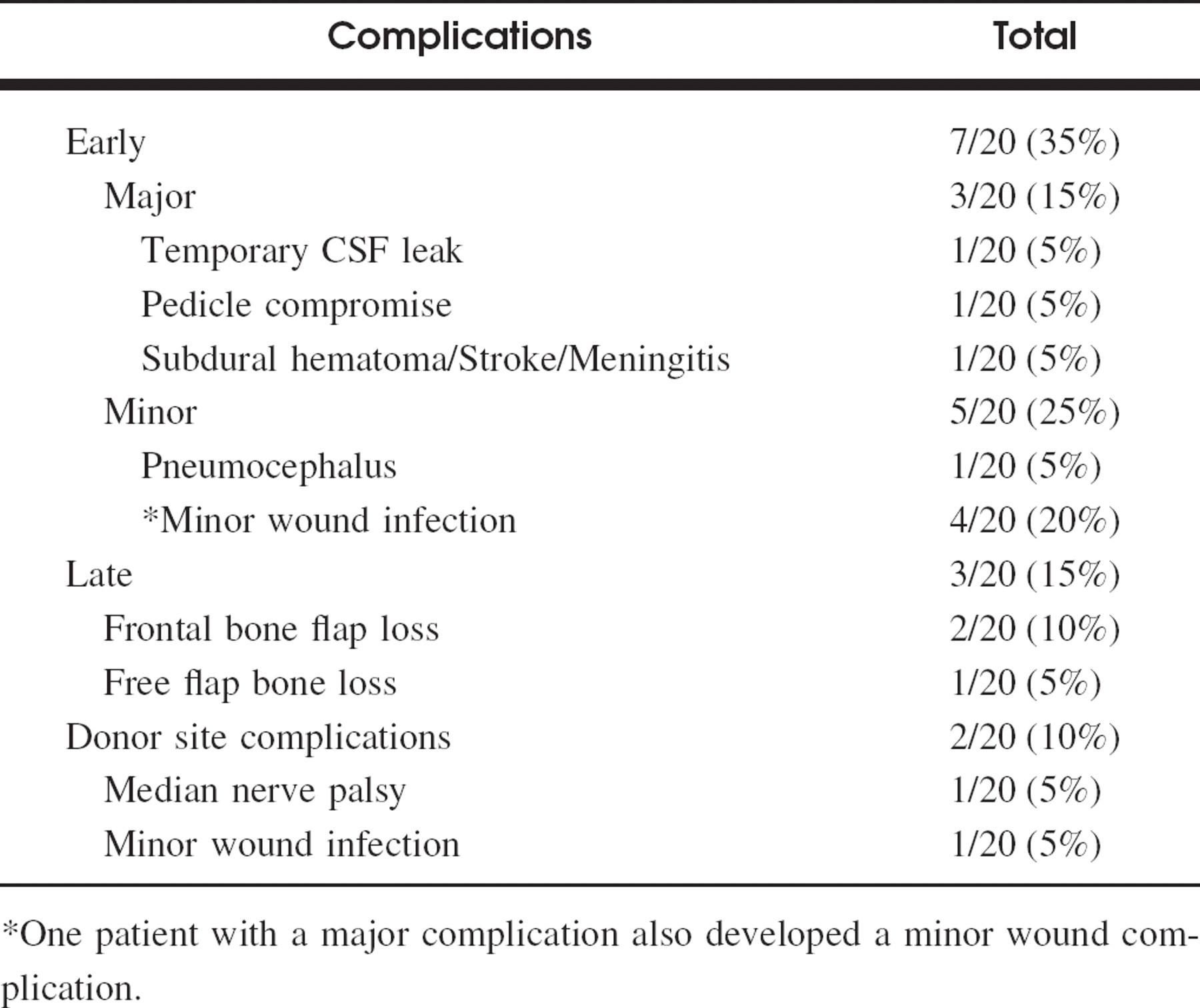
One patient with a major complication also developed a minor wound complication.
Three patients (15%) had late complications. Two patients had progressive loss of the subfrontal bone flap, which was used in the subfrontal approach. This was probably related to the poor vascularity in a previously radiated field. One patient had a delayed loss of the bony portion of his free flap. This patient developed a nasocutaneous fistula in the region of the medial canthus in the immediate postoperative period, after blowing his nose against medical advice. He would demonstrate this new anatomical relationship to friends and family, which led to a chronic fistula that eventually resulted in exposure and osteitis of the transplanted radial bone. The radial bone was removed 3 years following initial surgery with no further sequelae.
Two donor site complications (10%) occurred, including 1 median nerve palsy. The patient had a re-exploration and his nerve was noted to be intact. The etiology of his palsy is not entirely clear. He has subsequently had a near total recovery of function, following tendon transfer. There was also 1 minor donor site wound infection. None of the patients who had osseocutaneous flaps suffered pathologic radius fractures.
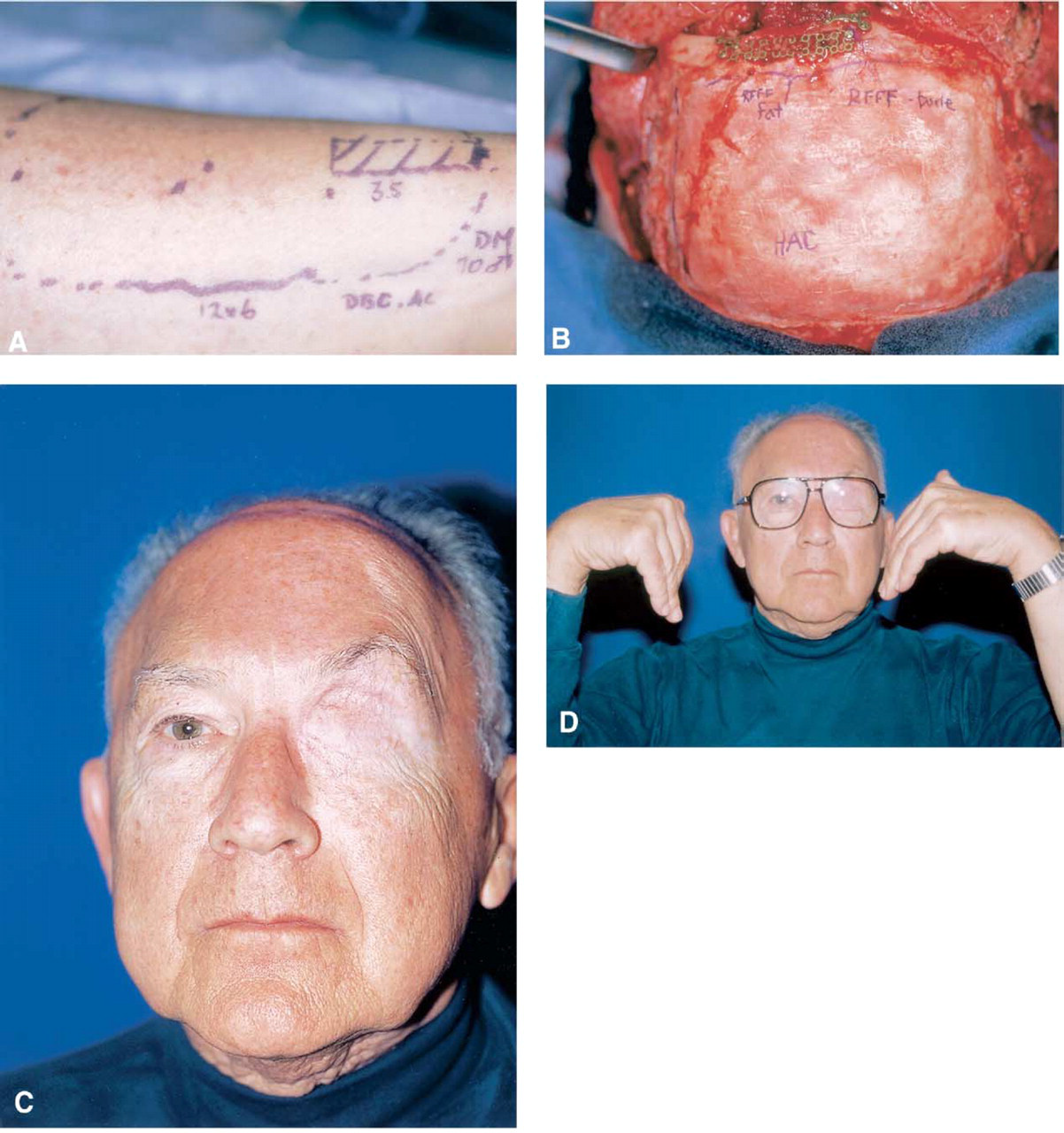
The mean operative time was 14 hours (range, 9.75–19.75 hours), and hospital stay ranged from 5 to 25 days (mean, 9.6 days). Two patients had prolonged hospital stay of more than 17 days. A representative case example from our series is summarized in Figure 1.
DISCUSSION
In this series, the incidence of CSF leak was 5% (1/20). The incidence of meningitis was 5% (1/20). Overall, 35% (7/20) of the patients had postoperative complications. Fifteen percent (3/20) of the complications were major, with 2/20 (10%) related to the reconstruction (CSF leak, venous compromise). Both of the major complications related to the reconstruction were successfully resolved with a single re-operation. One of the patients' complications (hemorrhage, meningitis, stroke) was related to the surgical dissection of the tumor along the internal carotid artery. There were no flap losses.
The published literature suggests that the overall surgical complication rate for skull base surgery varies from 27% to 75%. 1–6 It has been shown that previous surgery or prior treatment is associated with a higher complication rate. 2,3,20 Teknos et al 21 showed that hospital stay was significantly longer in previously radiated versus nonradiated patients who underwent skull base surgery. Some studies do not show an increased rate of complications in patients with prior surgery or radiation, but this may be due to the fact that many of their previously treated patients had free flaps for reconstruction. 1,4,6
Skull base reconstruction after previous surgery or radiation is more difficult. Scarring of the tissues and decreased vascularity make local flaps less reliable. The patients in this series had small-volume defects, which are typically reconstructed with local tissue. However, several studies have reported that vascularized free flap skull base reconstruction, by providing a reliable vascularized tissue barrier between the intradural contents and the sinonasal cavity, is associated with fewer complications compared with local or pedicled flaps. 5,6,12–15 In an attempt to reduce the complication rate, we utilized the radial forearm free flap to reinforce the dural closure of our pericranial flap. In this series, we found that the additional operative time required for free tissue transfer at the initial surgery is rewarded by fewer post-operative complications. Use of the radial forearm free flap reconstruction in previously operated or radiated patients who have low volume defects following skull base resection, resulted in a low major complication rate of 15%. We conclude that free tissue transfer can reduce local complication rates in salvage skull base surgery.