
Abstract
Most patients with neurothekeoma are young women. Neurothekeoma typically presents on the upper body, most commonly on the head or neck. The histologic and immunohistochemical characteristics of both cellular and myxoid neurothekeoma have been fairly well documented and the debate about the origin and proper classification of the 2 forms continues, particularly with reference to the cellular variant. Most previous reports of neurothekeoma have been of single cases or pathologic case series.
METHODS
We retrospectively reviewed 13 cases. The medical records of the 7 patients with neurothekeoma treated at UT M. D. Anderson Cancer Center over a 15-year period (1986–2001) were reviewed. The clinical findings, surgical treatment, follow-up, and histopathologic features were examined. In addition, M. D. Anderson Cancer Center pathology records of 6 additional cases were reviewed.
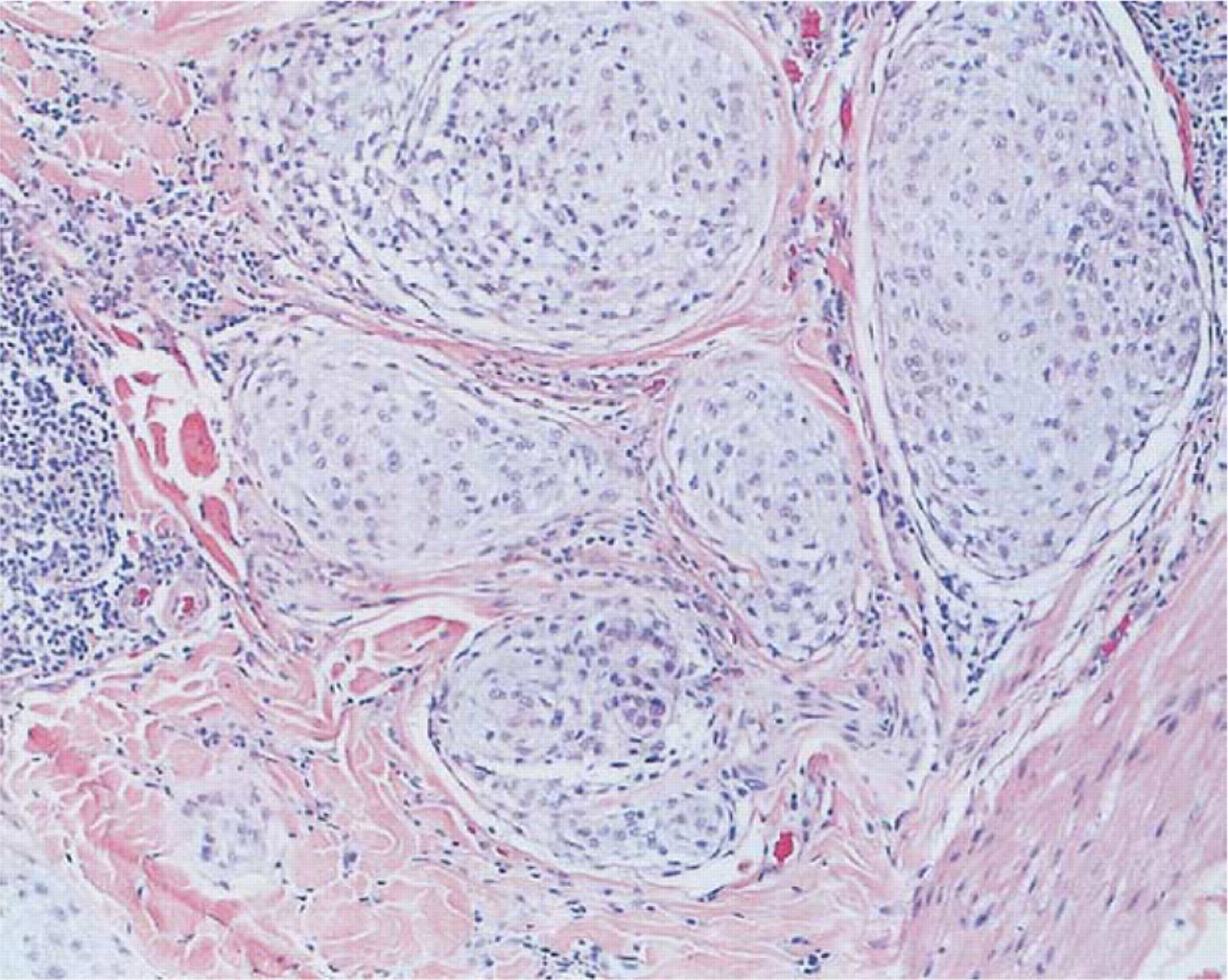
Cellular variant (x40 view); note characteristic clusters of spindle and epithelial cells.
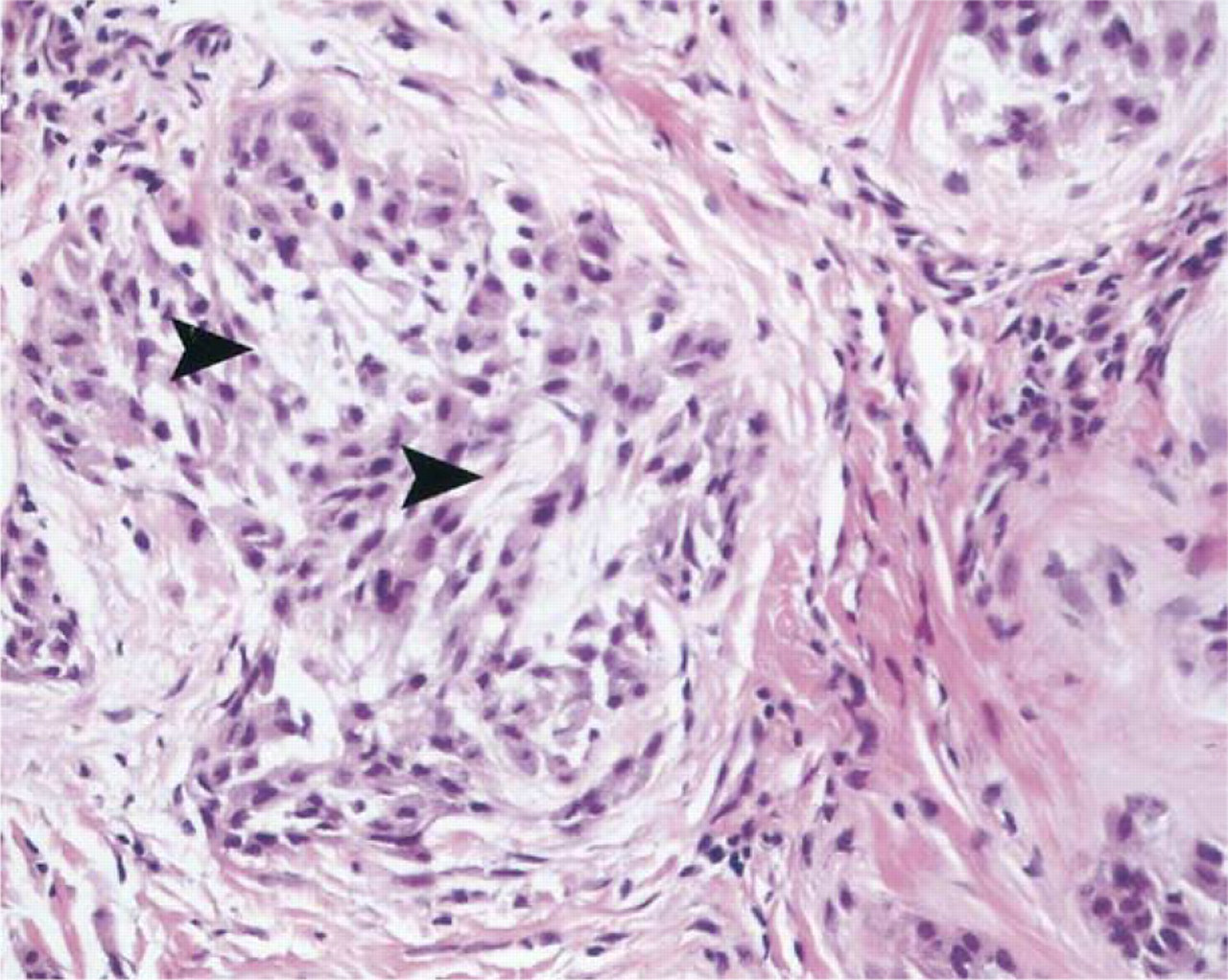
Myxoid variant (x40 view); note presence of loose collagen containing increased mucin (arrows).
RESULTS
Of the 13 patients reviewed, 9 were female and 4 were male. The mean age was 30 years (median, 24) with a range of 8 to 58. The locations of the lesions were varied, but the most were on the head and neck, 3 on the scalp, 2 on the neck, and 1 on the face. In addition, 4 lesions were on the extremities, 2 lesions were on the trunk, and 1 lesion was of unknown location. Of the 7 patients treated at M. D. Anderson Cancer Center, 4 were non-Hispanic whites, 2 were Hispanic American, and 1 was African American.
On histopathologic examination, all lesions had a characteristic nested pattern of growth with various degrees of myxoid background. Mitotic figures and marked cellular pleomorphism were not common. However, 2 lesions had atypical features: 1 lesion of the nasal ala had an infiltrative pattern with increased mitotic figures, and a second lesion of the thigh presented with local invasion through the underlying fascia and into the vastus lateralis muscle. Before treatment at M. D. Anderson Cancer Center, the patients had had various histologic diagnoses, including leiomyosarcoma (2 cases), malignant nodular hidradenoma (1 case), and clear cell hidradenoma (1 case). Two patients presented with no definitive diagnosis, and 1 patient presented initially at M. D. Anderson Cancer Center for evaluation and treatment.
All patients were treated with wide local excision. The 2 lesions with atypical features required more aggressive resection and reconstruction approaches. There have been no recurrences with a median follow-up of 8 months (range, 0–35 months).
CASE REPORTS
Case 1
A 43-year-old woman presented in 2001 with an erythematous lesion of the posterior neck with no definitive diagnosis. The lesion was posterior to the sternocleidomastoid muscle and 7.0 mm in diameter. In May 2001, the patient underwent wide local excision with 5-mm margins. Histopathological analysis revealed proliferation of nested cells with pale blue cytoplasm and central round nuclei, extending from the superficial reticular dermis to the deep reticular dermis. Immunohistochemical staining was negative for pancytokeratin, EMA, CD68, smooth muscle actin, S–100, chromagranin, and LCA. In January 2002, the patient was seen for follow-up and had no evidence of disease.
Case 2
An 8-year-old boy presented in 2000 with a raised erythematous lesion of the mid-anterior chest, 1 cm in diameter. The diagnosis at the time of presentation to M. D. Anderson Cancer Center was leiomyosarcoma. In October 2000, he was treated with wide local excision with 1-cm margins. Histopathological analysis revealed aggregates of proliferating spindle cells with oval or elongated nuclei and rare mitotic figures. These cells extended from the superficial reticular dermis to the deep reticular dermis. Immunohistochemical staining was negative for desmin, CD57, and S–100 and positive for actin. The patient was lost to follow-up.
Case 3
A 48-year-old women presented in 2000 with a raised erythematous lesion of the midline scalp posterior to the hairline, which was 3.0 × 4.0 cm. The diagnosis at presentation was probable malignant nodular hidradenoma. In October 2000, she was treated with wide local excision (5.5 × 7.5 cm). All margins were deemed clear by frozen section analysis. The surgical defect was reconstructed with a rotational flap and spit-thickness skin graft. Histopathological analysis revealed pleomorphic oval to fusiform cells in a cellular infiltrative pattern confined to the dermis. Immunohistochemical staining was negative for EMA and CD57 and weakly focally positive for S–100. In June 2001, the patient was seen for follow-up and had no evidence of disease.
Case 4
A 40-year-old woman presented in 2001 with a 3-year history of a 1-cm lump in her distal right thigh. Although painless, the lesion had become pruritic. In April 1999, the lesion was biopsied. In January 2001, the lesion was excised and she was referred to M. D. Anderson Cancer Center for follow-up. Upon review of the biopsy and surgical specimens by the Department of Pathology, the diagnosis of cellular neurothekeoma was given. In April 2001, the patient underwent wide local excision of the previous excision site with 3.0-cm margins. The incision extended to the fascia of the vastus lateralis muscle at the insertion on the quadriceps tendon. The fascia was removed along with a small portion of the vastus lateralis muscle and the distal third of the rectus femoris muscle. The surgical defect was repaired with a right thigh skin advancement flap. Histopatho-logical analysis revealed cellular neurothekeoma of the deep dermis extending into the subcutaneous tissues. In November 2001, the patient was seen for follow-up and had no evidence of disease.
Case 5
A 17-year-old girl presented in October 2000 with a lesion of the left nasal ala and a 5-mm scar. In August 2000, an excisional biopsy was performed, and a histopathologic diagnosis of clear cell hidradenoma was made. Immunohistochemical staining was negative for mucin, desmin, S-100, synaptophysin, and cytokeratin and focally positive for SMA and MCA. In late August, the lesion grew rapidly. In early September, the patient underwent a second excisional biopsy, and a histopathologic diagnosis of an unclassified malignant neoplasm was made. Immunohistochemical staining was negative for HMB45, keratin, actin, EMA, and S-100. The patient was then referred to M. D. Anderson Cancer Center, where the lesion was confirmed as cellular neurothekeoma. In October 2000, she was treated with re-excision of the lesion by using 4 stages of Möhs micrographic surgery. Histopathology revealed cellular neurothekeoma with focal myxoid change, infiltrative pattern, and increased mitotic figures atypical in shape. The surgical defect was repaired with a left nasal labial transposition flap with primary repair of the nasal lining. In April 2001, the patient was seen for follow-up and a revision of the flap. She was had no evidence of disease in November 2001 when she was seen for follow-up again.
Case 6
A 22-year-old man presented in 1986 with a lesion of the right mastoid area and a previous diagnosis of leiomyosarcoma. In May 1986, the lesion was excised by punch biopsy. Histopathological analysis revealed neurothekeoma. The lesion was then removed with wide local excision. Histopathological analysis revealed no residual tumor. The patient was lost to follow-up.
Case 7
A 58-year-old woman presented in 1993 with a lesion of the right posterior neck. In December 1993, the lesion was partially excised during an excisional biopsy. Histopathological analysis revealed a spindle cell neoplasm with neuroid features. Immunohisto-chemical staining was negative for S-100 and HMB45. In January 1994, the lesion was treated with wide local excision. Histopathology revealed neurothekeoma. Immunohistochemical staining was negative for S-100 and positive for actin. In December 1996, the patient was seen for follow-up and had no evidence of disease.
Cases 8 through 13
Cases 8 through 13 were reviewed by the Department of Pathology at M. D. Anderson Cancer Center for diagnosis only. The findings from all 13 subjects are summarized in Table 1.
DISCUSSION
In this study, the pathologic and clinical findings of a series of neurothekeoma cases are presented. We believe that although neurothekeoma is a benign neoplasm, these lesions should be treated with wide local excision and frozen section assessment of margins because of the possibility of local invasion and recurrence. Although none of the cases reviewed here suffered a recurrence, atypical features were found in 2 of the cases, 1 with extension into subcutaneous fascia and muscle and 1 with increased mitosis and an infiltrative pattern. Atypical features described in neurothekeoma include size greater than 1 cm, cellular atypia, mitotic activity, deep penetration, and infiltrative margins, and cases involving invasion of fat, skeletal muscle, and vasculature have been reported. 5 As previously reported by Busam et al, 5 wide excision appears to be curative even in cases with atypical features, although such lesions may require more extensive resection and reconstruction. Although cases arising in the oral mucosa, paranasal sinuses, and eyelids have been reported, 6 - 8 the vast majority of cases reported in the literature as well as all of those reported here were cutaneous in origin and most are located within the head and neck region. Care must be taken in the diagnosis of spindle cell neoplasms, and neurothekeoma should be considered in the differential diagnosis for such lesions involving the skin. Although none of the cases treated at our institution were previously diagnosed as melanoma, two were incorrectly classified as leiomyosarcomas and such a misdiagnoses are a concern. The fact that neurothekeoma typically stains negative for S-100 and HMB45 may be of value in correct classification. Although such lesions are also treated surgically, the work-up, prognosis, and follow-up of these entities differ, therefore correct diagnosis is critical.
Demographics and clinical characteristics and treatment/follow-up
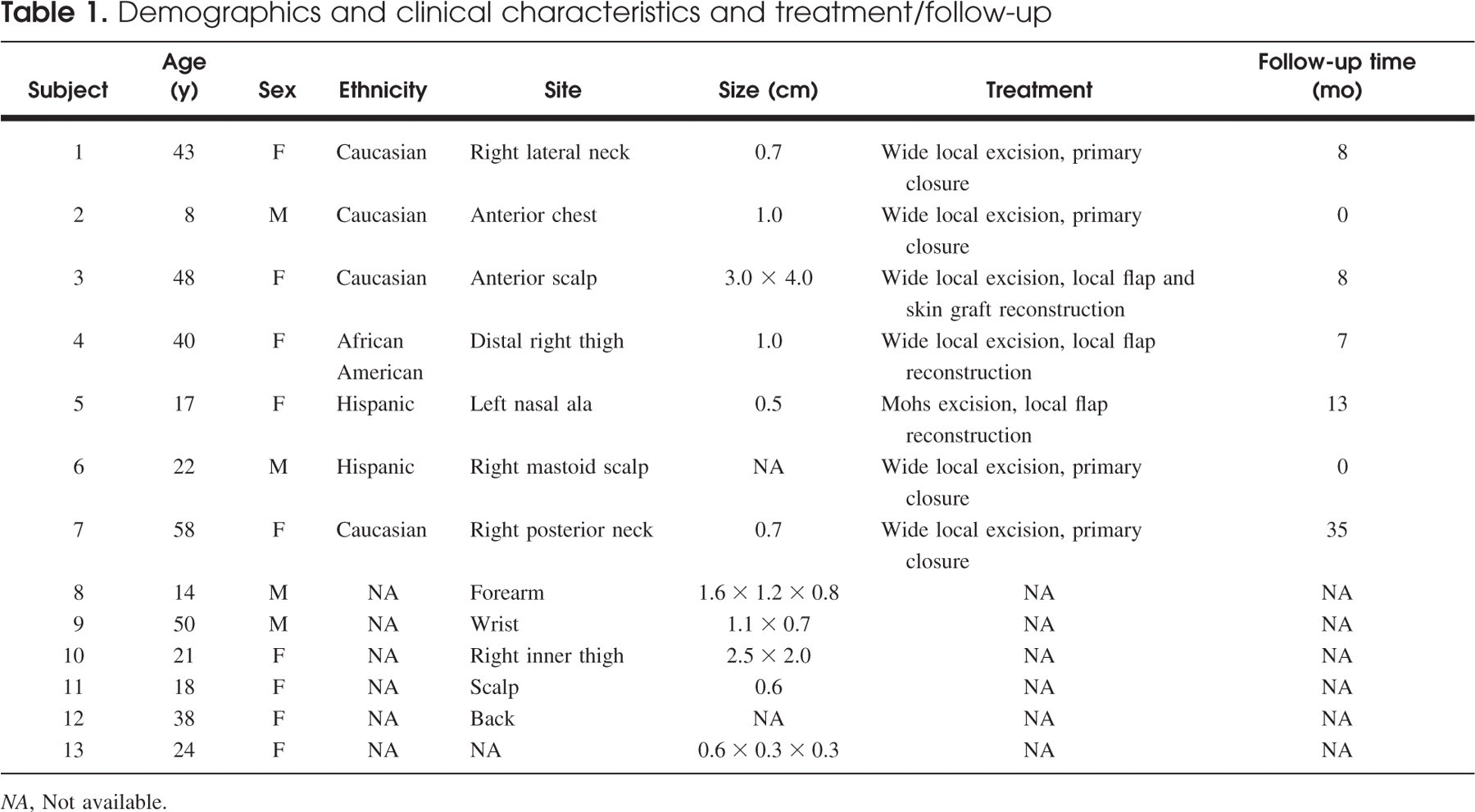
NA, Not available.
We would like to thank Dr Maureen E. Goode for manuscript editing and Ms Deanna Thomas for manuscript preparation.