
Abstract
PURPOSE: This study evaluated the feasibility of fiberoptic CO2 laser soldering for the repair of esophageal injuries under tight temperature feedback control in an animal model. Healing was compared to conventional suture closure.
MATERIALS AND METHODS: A CO2 soldering system equipped with infrared transmitting silver halide fibers was used. The soldered tissue temperature was monitored continuously, and laser power was adjusted to provide constant temperature. The procedure was done with 50% bovine serum albumin solder. Longitudinal incisions measuring 8 to 10 mm were made under general anesthesia in the cervical esophagus of 25 rats. Twenty rats (group I) underwent laser tissue bonding; 8 of which were tested in a preliminary study to determine optimal laser parameters. In the remaining 5 rats (group II, controls), closure was performed with 1 layer of 6/0 Vicryl sutures. The rats were sacrificed 2, 3, 4, and 6 weeks postoperatively, and the esophagus was examined histologically.
RESULTS: Optimal temperature was found to be 65 to 70° C and optimal exposure time, 150 to 200 seconds. Laser soldering was successful in 9 of the 12 rats (75%) treated under optimal settings; suturing was successful in 4 of the 5 control rats (80%). There were no significant differences between the groups in healing or complication rates.
CONCLUSIONS: These results indicate that the CO2 laser soldering technique is a valid option for the correction of esophageal tears or incisions in rats. The confirmation and extension of these findings in further studies with larger animals may ultimately lead to the routine in vivo use of temperature-controlled laser repair for the esophagus and other organs. This method lends itself to endoscopic bonding of tissues.
Laser tissue welding has been used to date in the repair of hollow or tubular structures, such as arteries and veins, 1,2 intestines, 3,4 ureters, 5 and trachea. 6 Several authors have reported that temperature control improves results for rat intestinal, vascular, and bladder welding. 7–11 Other researchers have attempted to improve sealing with the use of biological solder. 12–14 Our review of the literature revealed 2 experimental studies of laser-assisted repair of esophageal incisions. Eby et al 15 used a rigid CO2 laser, and Auteri et al 16 combined diode-laser activation of tissue solder with hand-sewn anastomosis.
We hypothesized that laser soldering combined with tissue-surface temperature feedback control may be more effective than standard sutures in promoting closure of esophageal lacerations.
MATERIALS AND METHODS
Instrument
We used a CO2 laser (Model 48 soldering system; Synrad, North Inn Creek, WA) 17 consisting of an infrared detector, and 2 optical silver halide (AgClBr) fibers, each measuring 1 M in length and 0.9 mm in diameter. These fibers are highly transparent in the infrared range. One fiber delivered the CO2 laser beam to a small target on the tissue. The heated target then emitted infrared radiation which was in proportion to its temperature, and the radiation was transmitted through the second fiber onto the detector. The electrical voltage signal generated by the detector was calibrated to yield the temperature of the heated target. 17 The detector voltage was measured by a computer, which then controlled the laser output. This feedback loop made it possible to control the tissue temperature to an accuracy of ±3° C.
In the present study, laser spot size was approximately 2 mm; the fiber tips were held together at 3 to 4 mm above the heated tissue. The laser power density at the heated area was 10 w/cm2.
Animals
Twenty-five female Sprague-Dawley rats weighing 250 to 300 g were divided into 2 groups. Group I (n = 20) underwent laser repair of the cervical esophagus under temperature feedback control, using 50% albumin biological solder. The temperature was set at 65 to 70° C. Group II (n = 5) (control group) underwent suture closure of the cervical esophagus.
All animals received humane care, and the protocols were approved by the Animal Care and Use Committee of our institution.
Procedure
The animals were placed in the supine position and anesthetized with a mixture of ketamine (90 mg/kg) and xylazine (10 mg/kg). The neck was shaved and cleaned with an antiseptic solution. An intraluminal stent (a nasogastric tube) was introduced into the cervical esophagus. The strap muscles were divided vertically, and the cervical esophagus was exposed. A longitudinally oriented incision measuring 8 to 10 mm was made. The field was kept dry of blood and saliva with sponges. In group I, several drops of 50% bovine serum albumin were applied to the edges of the perforation, which were then approximated with forceps. CO2 laser power was delivered, as explained in the previous section. This process was repeated several times, spot by spot, until the entire incision length was bonded. The procedure lasted 1 to 2 minutes. In group II, the esophageal perforations were closed with 2 layers of 6/0 Vicryl sutures, placed through the mucosa and muscular layers. The average time for this procedure was 5 to 6 minutes. Saline was then infused through the nasogastric tube to check for leakage. We did not use continuous neck drainage after the procedure, and no antibiotics were given. Water was supplied ad libitum starting 24 hours after surgery. No food was given for the first 48 hours postoperatively; thereafter, the animals received their regular diet.
The rats were killed 2, 3, 4, and 6 weeks after surgery, and the esophagus was removed for histological examination. The soldered and the sutured sites were excised and fixed in formalin, embedded in paraffin, and sectioned. Sections of 5-μm thickness were stained with hematoxylin-eosin and placed under the light microscope.
Statistical Analysis
The statistical difference between the two groups was evaluated by the Fisher exact test and was found not significant (P = 0.46).
RESULTS
In 8 of the 20 rats in group I, soldering was done under various temperatures and exposure times to determine the optimal laser setting. All 8 rats died; the causes of death included total breakdown of the weld, esophageal fistula with massive leakage, and neck abscess. These studies showed that a reliable weld was obtained when temperature was maintained at 65 to 70° C and exposure time at 150 to 200 seconds. In the first 4 of 8 rats, the tensile strength test (TST) was performed immediately after soldering in an attempt to better define the factors influencing optimal soldering. However, the aggressiveness of the test for the delicate esophageal mucosa combined with the death of all 4 animals regardless of the TST results led to our conclusion that there was apparently no correlation between the TST findings immediately after soldering and the later durability of the soldered area. The TST was therefore discontinued.
Of the remaining 12 rats that underwent laser soldering under optimal conditions, results were successful in 9 (75%). Three rats died after 1 to 2 weeks because of neck abscess and necrosis.
In the 2 rats of the soldering group sacrificed 2 weeks after operation, macroscopic study showed a thin, delicate scar site. Microscopically, the luminal surface of the tissue was reepithelialized with mature squamous epithelium. The submucosa and muscular layers consisted of granulation tissue, with ingrowths of new blood vessels and reduced inflammatory reaction. One week later, 2 more rats were sacrificed and microscopic examination showed a normal mucosal layer and fibrotic changes in the submucosa and muscular layer (Fig 1). The same findings were noted at 4 and 6 weeks.
In group II, closure with a 1-layer interrupted suture was successful in 4 of the 5 rats (80%). After 3 weeks, the luminal surface had reepithelialized with mature squamous epithelium. The scar consisted of a cellular connective tissue devoid of inflammatory infiltrate. Foreign body reaction was observed around the suture (Fig 2).
There were no significant differences between the groups in incidence and types of complications. Nearly all complications occurred within the first 72 hours.
DISCUSSION
In the past decade, only two studies have investigated the use of laser heating for esophageal repair. Eby et al 15 did not use a biological solder or temperature control, and the laser-bonded specimen demonstrated a significant thermal burn that resulted in a delay in epithelialization of the esophageal mucosa. Only after 1 month was there no significant histological difference in healing between the laser-repaired and sutured groups. In 1992, Auteri et al 16 observed that the laser activation of tissue solder in single-layer hand-sewn intrathoracic esophageal closures in dogs increases bursting pressure and may lessen the prevalence of dehiscence. Biological solders have been widely used for laser repair of other tissues to promote adhesion between the bonded edges. These 2 studies show that laser repair is possible for esophageal tissues, with and without biological solder. As for other organs, the quality of the soldered incision depends on the temperature at the soldered site. 7–10
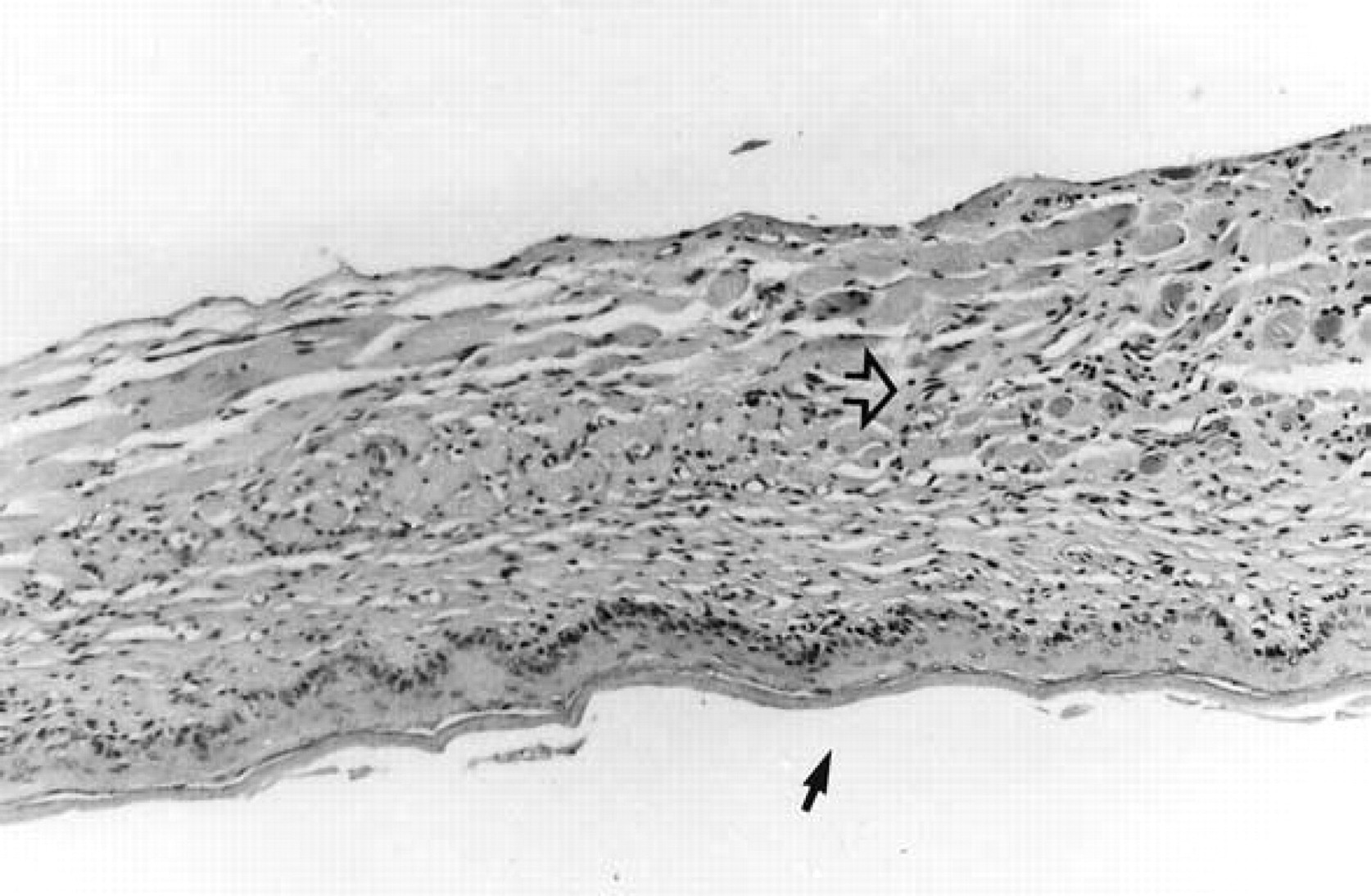
Esophageal wall 3 weeks after laser soldering: luminal surface covered with mature epithelium (full arrow); minimal fibrotic changes in submucosa continuous to muscular layer (empty arrow).
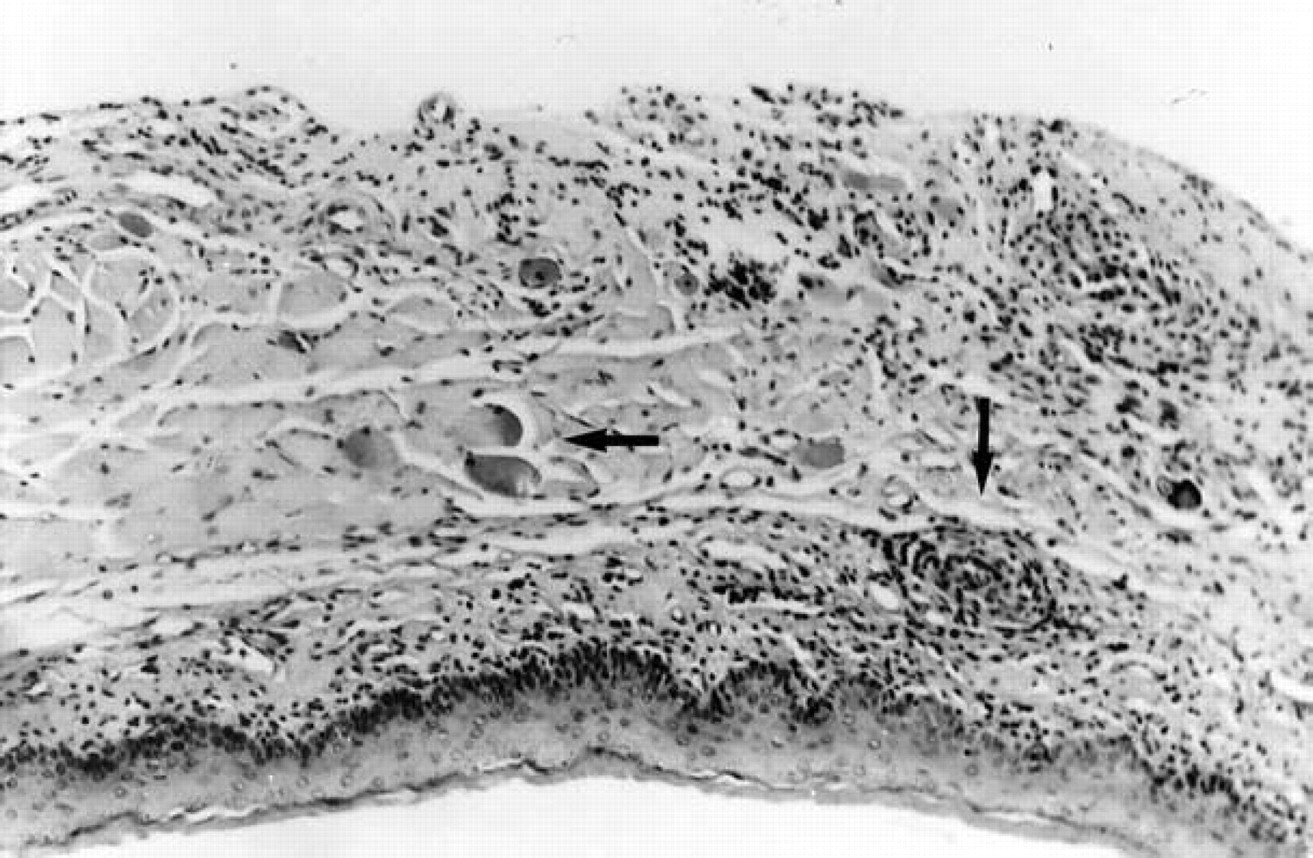
Esophageal wall 3 weeks after closure by 2-layer interrupted sutures: foreign body reaction around sutures (arrow).
The present work introduces the use of the fiberoptic CO2 laser for repairing esophageal incisions. CO2 laser soldering is still an experimental technique in neck surgery, with the potential advantages of providing immediate watertight closure and lack of foreign body reaction. To enhance the technique, we used a 50% biological solder and temperature feedback control. Results showed that the system is feasible for repair of the esophagus in an animal model. The desired temperature of the laser-heated tissue was obtained without vaporization or carbonization of the esophageal wall. Histological comparison with suture closure revealed a similar regeneration of the epithelial lining of the mucosal surface of the esophagus wall. Suture closure, however, was associated with a more intense inflammatory process, with foreign body reaction. Survival was relatively high in both groups (75–80%), and complication rates were similar. Most of the complications were a direct result of the small and thin rat esophagus, which is approximately 2.5 to 3 mm wide, and therefore caused technical difficulties during the laser bonding or suturing procedures. Because of its size, we used a laser spot diameter of approximately 2 mm; 2-layer soldering was unfeasible. In future experiments, we plan to use larger animals (e.g., rabbits) to compare 1-layer and 2-layer closure.
The TST probably causes small openings in the soldered tissue, necessitating resoldering that leads, in turn, to further thermal injury to the incision site mucosa as well as nonhomogeneous welding of the albumin. The latter appears clinically as small bulks/crusts of albumin at the soldering site.
In conclusion, this study shows that the combination of the CO2 laser with laser-activated biological solder and temperature control for esophageal repair may ensure strong closure with minimal thermal damage. Compared with suturing, there is less foreign body reaction and fibrosis. The procedure can also be performed much more (2–3 times) rapidly than suturing. The confirmation and extension of these findings in future studies may ultimately lead to the routine use of laser soldering in vivo for the esophagus and other organs. Finally, it should be emphasized that the thin and flexible silver halide fibers could be easily inserted through the ancillary channel of an endoscope. This may pave the way towards the use of laser soldering endoscopically.
CORRECTION
In the September 2003 issue of the Journal, in the article by Sadick et al titled “Plasma surgery and topical estriol: Effects on the nasal mucosa and long-term results in patients with Osler's disease” (2003;128:233–8), the correct order of the authors' surnames is as follows: Haneen Sadick, MD, Ramin Naim, MD, Jasmina Oulmi, MD, Karl Hormann, MD, and Wolfgang Bergler, MD.