
Abstract
To delineate a technique that avoids the complications associated with surgical closure of long-term or permanent tracheostomy (LTT).
A case series that describes the technique and clinical outcomes.
Thirty-seven of 300 patients with a previously established LTT underwent primary surgical closure of their stoma after their underlying disease had been resolved. The surgical technique combined a turnover flap with medialization of fibroadipose tissue, followed by additional closure with an advancement skin flap.
After a mean follow-up of 3.2 years, no patient developed major complications. Four patients developed minor complications, which responded to conservative treatment. In all patients, the functional results were satisfactory, as were the cosmetic results, with the exception of 1 case. None required retracheostomy.
This simple and reliable new surgical technique for closing LTT avoids the potential failures and complications encountered in previously published procedures.
A “long-term” or “permanent” tracheostomy (LTT) is, by definition, an intentional noncollapsing and nonstenosing stoma. It is usually performed whenever prolonged maintenance of a tube-free, self-sustaining stoma is anticipated. 1 - 6 The establishment and long-term maintenance of LTT is relatively new and hitherto not fully appreciated. For more details on LTT, the reader is referred to the manuscript published in 2000 by Eliachar. 3
The phrases “long-term” or “permanent” do not imply irreversibility, and surgical closure of a permanent stoma may be contemplated whenever the underlying disease had been resolved. For example, a stoma may be performed at the beginning of a complex staged laryngotracheal reconstruction and may be surgically closed after successful completion of this process. 1 - 3
Long-term tracheostomy cannot and should not be compared to persistent tracheocutaneous fistula (PTCF). To the best of our knowledge, with the exception of 1 reference in the literature, 7 all reports in the literature relate to closure of PTCF. Such a fistula is commonly regarded as a pathologic complication of “temporary tracheostomy,” resulting from failure of the tracheostomy tract to close spontaneously when the cannula is intentionally withdrawn. 8 - 16 This is in contrast to a permanent tracheostomy, which is a predetermined procedure intended to establish a tracheocutaneous communication until timely surgical closure is indicated. Indeed, a tracheostomy is performed in a manner that avoids the typical features of a fistulous tract by shortening the distance between the trachea and the skin, removing all the intervening tissues, and establishing a tight circumferential permanent mucocutaneous junction. 1 - 3 Techniques for closure of PTCF range from fistulectomy with closure by secondary intention to multilayered closure of de-epithelialized local tissue. 7 - 16 As reported, it may not be possible to achieve an air- and water-tight closure of the tracheal defect with these techniques. As a result, the positive air pressures generated by coughing or speaking can dissect through the suture line and penetrate surrounding tissues. Air and secretions are trapped and prevented from exiting through the skin. The positive pressure builds, forcing the trapped air into the fascial planes of the neck and chest through establishment of a 1-way valvelike mechanism. Infection may follow the spread of contaminated air, blood, and secretions. 10 , 11 Subcutaneous emphysema, pneumothorax, pneumomediastinum, and respiratory compromise may develop. Other potential complications of surgical closure techniques include local wound infection, bleeding, hematoma or seroma formation, and suture granuloma. Cosmetic deformity is a common complication that often requires additional surgery. Tracheal stenosis and/or malacia are prone to develop at the closed tracheostomy site with consequent airway obstruction. 7 - 9
To resolve these problems, a new surgical technique was developed. It combines a turnover flap with medialization of fibroadipose tissue, followed by additional closure with an advancement skin flap. This report discusses the operative technique and the clinical results.
Study population
LTT, long-term tracheostomy; LTR, laryngotracheal reconstruction.
METHODS
Three hundred patients underwent the LTT procedure between 1991 and 2002. Thirty-seven of these patients underwent primary closure of their stoma after their underlying disease had been resolved (Table 1). Because spontaneous closure was not likely, surgical closure of the stoma was indicated.
The procedure started with close examination of the patient. If hair was present on the intended skin turnover flap, it was removed by electrolysis. The status of the larynx and trachea and the swallowing mechanism were analyzed by fiberoptic laryngoscopy, fluoroscopy, and CT. We have found the imaging studies valuable in determining the relationship between the larynx, trachea, stoma, and digestive tract, to avoid overlooking potential subclinical abnormalities (e.g., narrowing or collapse) that might be missed during endoscopic examination and adversely complicate the post-closure healing process. If the tracheostomy has been performed due to obstructive sleep apnea syndrome, the patient underwent polysomnographic studies with the stoma open and occluded.
Surgical Technique
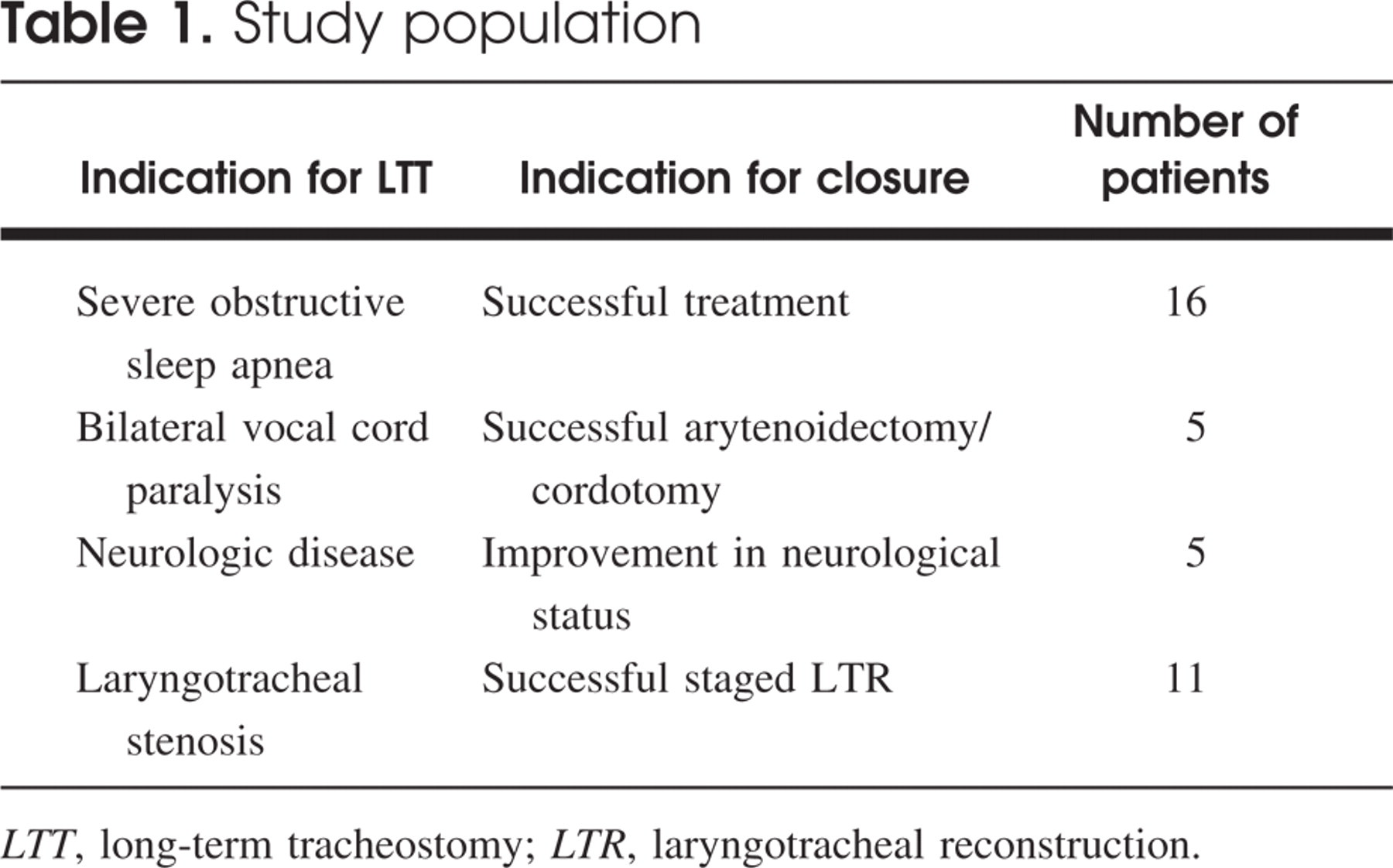
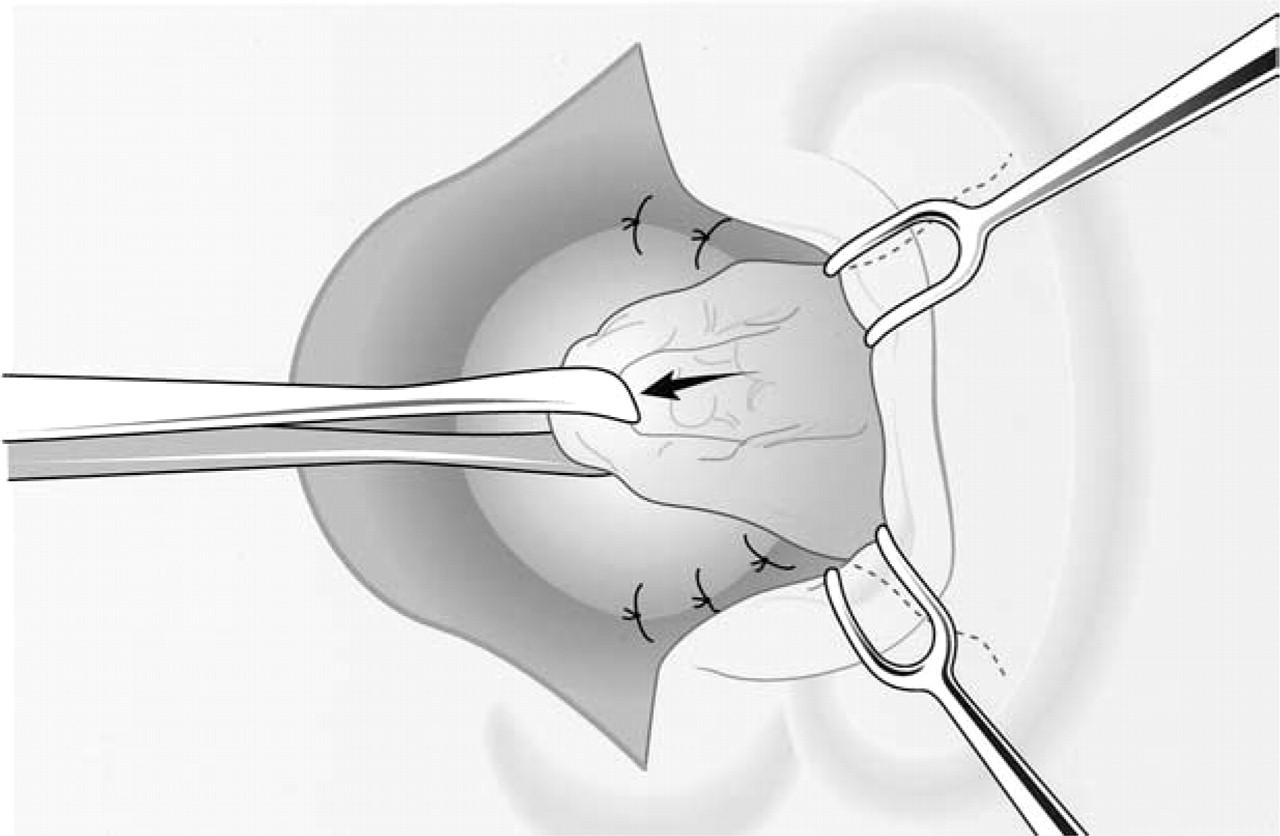
Surgical closure was performed with the patient under either general or local anesthesia. The patient was placed in a supine position, with the shoulders elevated and the neck moderately extended. A vertical midline skin incision was made starting 1 cm above the tracheal fenestration and dipping down to 2 mm lateral to the mucocutaneous junction. The incision was extended along one side, 180 degrees to the 6 o'clock position of the tracheal fenestration (Fig 1). Wide undermining created a laterally based advancement flap (Fig 2). A crescent-shaped skin incision, which was configured according to the dimension of the tracheal fenestra, was then made on the opposite
Skin markings and incision lines for surgical closure of a long-term tracheostomy by a medially based turnover flap (dark) and a laterally based advancement flap (arrows). Undermining of the laterally based advancement flap. The mucocutaneous junction on the opposite side remains intact.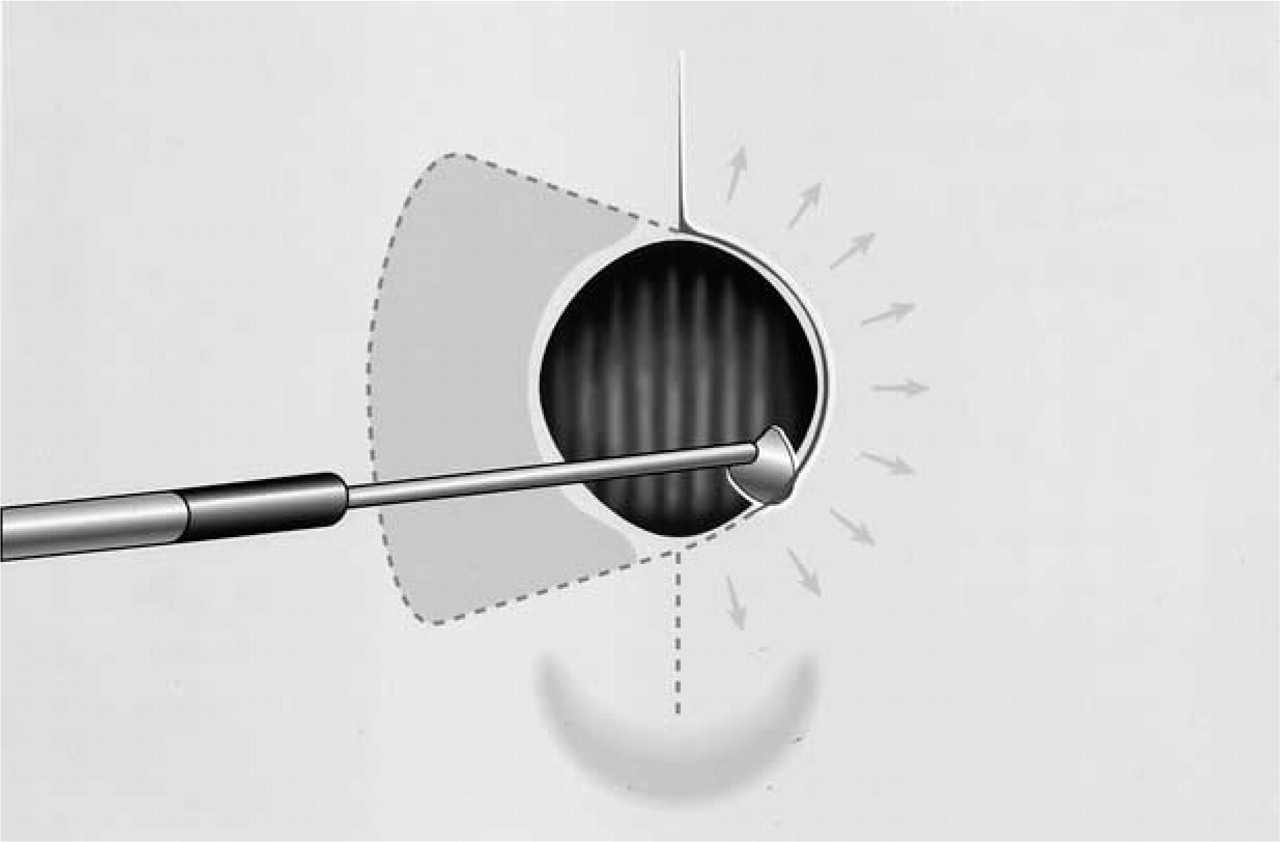
Postoperatively, each patient was observed overnight to rule out hematoma formation or subcutaneous emphysema. Patients were encouraged to protect the wound for 1 week by applying finger pressure locally while coughing or talking. The drain was removed 36 hours after surgery and the skin sutures were removed after 5 to 7 days. Close long-term follow-up of these patients to verify absence of potential late complications such as tracheal stenosis or malacia was routinely performed. The patients underwent flexible fiberoptic endoscopy every 4 to 6 weeks until 6 months after surgery and once a year thereafter.
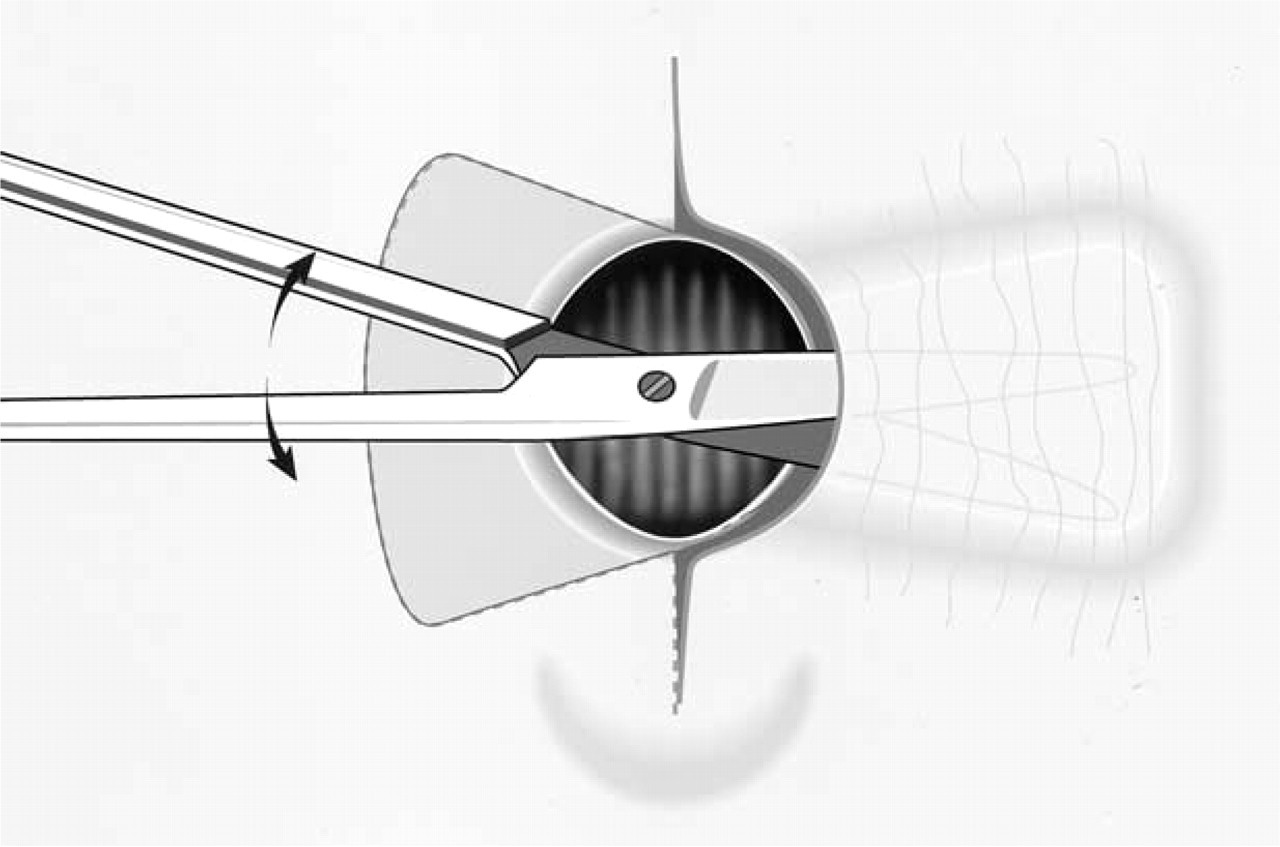
The medially based turnover flap is flipped over (skin inside, facing the lumen) and is sutured to the opposite free margins.
Fibroadipose tissue or muscle are advanced medially to fill the craterlike depression.
RESULTS
The follow-up period ranged from 6 months to 7 years (mean, 3.2 years; Table 2). Four minor complications occurred. Two patients developed a small hematoma, which resolved with pressure dressing and antibiotics. In 1 of these patients, the drain was prematurely pulled out 12 hours after surgery. The third patient developed local subcutaneous emphysema after the negative-pressure drain malfunctioned and was pulled out. One patient with diabetes developed a wound infection that resolved with antibiotic treatment.
The subcutaneous layer and skin are advanced and closed with interrupted sutures. A final vertical suture line is presented as this was performed in the majority of cases.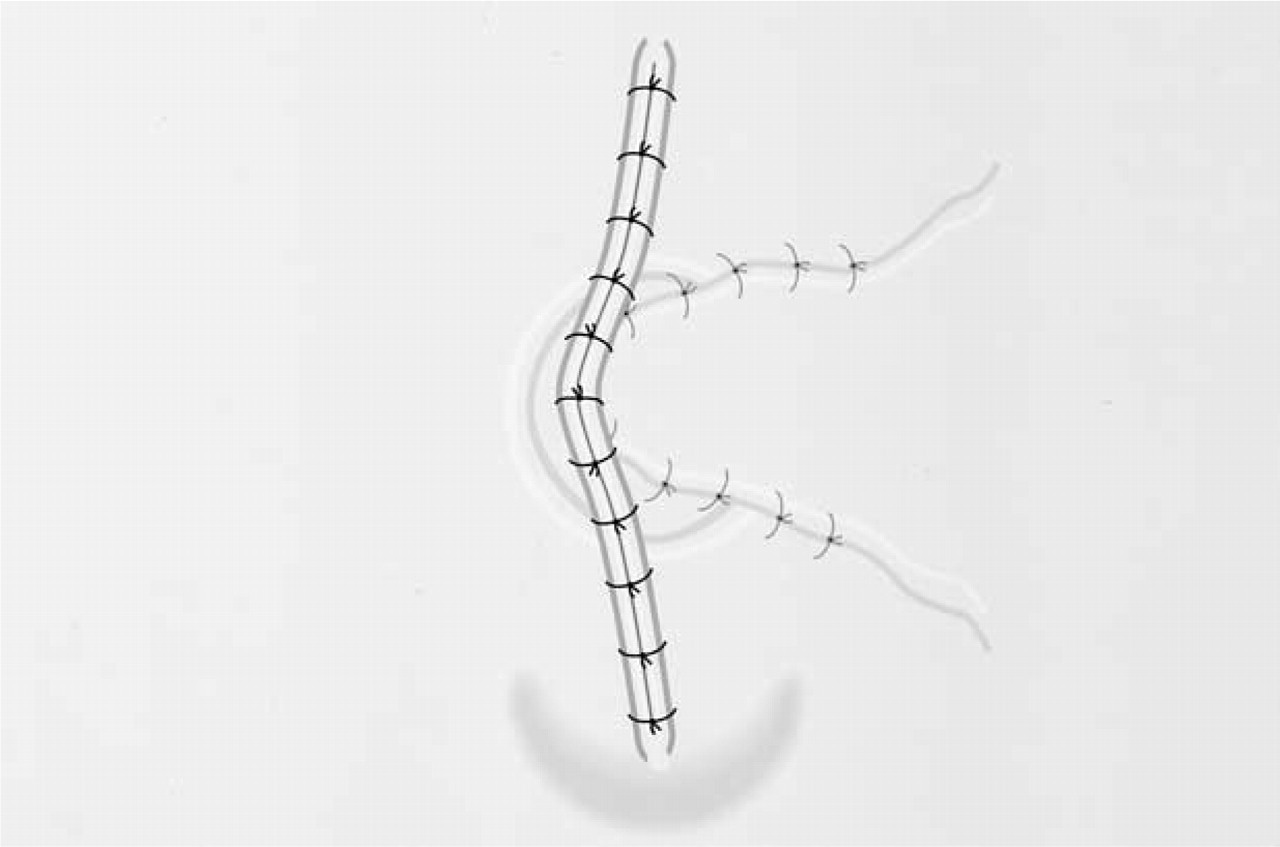
DISCUSSION
Long-term tracheostomy is by now an established way to provide prolonged maintenance of a tube-free, self-sustaining stoma. As more patients recover from their underlying disease due to improved health care, we might anticipate a growing number of candidates for surgical closure of LTT.
Based on our experience, we have found our technique to be safe and reliable. In addition, it is more advantageous than other techniques in a variety of ways:
When meticulously executed and properly planned, even a very wide stoma with large craterlike depressions may be successfully closed applying this single-staged procedure. The tracheal defect is mended at the site of the fenestra with a well-perfused, randomly vascularized skin flap. This provides a viable, immediate, and sustained continuous epithelial lining of the intraluminal defect in the anterior tracheal wall surface, thereby preventing future complications such as granulation tissue formation and tracheal stenosis. None of the other flap techniques described in the literature provides immediate re-surfacing of the inner tracheal wall with smooth epithelial-lined viable skin while simultaneously securing the integrity of the tracheal walls at the level of the fenestra. Unfortunately, there is no long-term follow-up in other flap techniques published thus far.
7
-
15
The fibrous scar tissue surrounding the stoma is beneficially applied in resisting prolapse of the flap during the ventilatory cycle. The postoperative period is free of significant complications. The creation of a secure watertight closure of the tracheal defect prevents air and secretions from escaping into the chest or neck. Meticulous hemostasis and mini-drains providing effective continuous negative pressure prevent subcutaneous emphysema and hematoma formation. Perioperative antibiotics prevent cellulitis, abscess formation, wound dehiscence, and septicemia. No patient developed a major early postoperative complication reported with some of the other techniques,
7
-
15
and attributed to “closure in layers.” Yet, for the sake of safety, we continue to insist on overnight postoperative observation. Advancement of viable, randomly vascularized muscle or subcutaneous fibroadipose tissue fills in the craterlike depression at the stoma site and prevents potential “empty spaces” that tend to promote seroma, hematoma, or abscess formation. It also prevents cosmetic deformities resulting from these craterlike depressions. Primary tension-free closure of the skin results in consistently acceptable cosmetic results. Although the final closing skin suture lines were vertical in 21 of the 37 patients, the cosmetic result was satisfactory in all patients except the 1 who developed keloid.
Results of surgical closure of long-term tracheostomy

N, number of patients; F.U., follow-up period; SCE, local subcutaneous emphysema; He., hematoma formation; Good funct., good functional result; re-trach, required re-tracheostomy. The number in parentheses is the mean.
Tracheomalacia or collapse of the skin flaps during inspiration was of concern initially. Indeed, after the wounds completely healed, the skin covering the stoma bulged out or retracted inward in synchrony with the ventilatory cycle. This phenomenon has not been associated with airway restriction or obstruction in any of the patients in this series, obviating the need to apply any rigid supportive grafts. The tight and highly fibroelastic nature of these flaps (which double or triple upon each other), and their lateral attachments to the indurated and fibrosed noncollapsing stomal margins, in effect expand the lumen at the level of the closed stoma, rather than constrict it.
CONCLUSIONS
A safe, reliable, and simple technique for primary surgical closure of LTT was presented. It can be performed on any patient with a long-term or a permanent tracheostoma, regardless of the original tracheostomy technique or of the size of the stoma.