
Abstract
To determine the feasibility and accuracy of fine-sectioned frozen-section analysis of the sentinel lymph node (SLN) in cN0 oral cavity and oropharynx squamous cell carcinoma.
Thirty-one patients were included and underwent lymphoscintigraphy a day before surgery and marking of the SLN. Intraoperatively, the SLNs were identified using a gamma probe, excised, and analyzed using fine-sectioned frozen section. The remaining SLN tissue was fixed in formalin for further staining and immunohistochemical analysis. An elective neck dissection was performed in all patients and all excised lymph nodes were examined for metastatic disease.
SLNs were identified preoperatively by lymphoscintigraphy as well as by gamma probe intraoperatively in all patients. A total of 82 sentinel lymph nodes were excised and analyzed by fine-sectioned frozen section. Micrometastases were found in 16 out of the 82 SLNs, upstaging 14 out of 31 patients (45%) from cN0 to pN+. Furthermore, a total of 1295 lymph nodes from the neck dissection specimens were analyzed, confirming only one more metastatic disease. Sensitivity and negative predictive value of SLN biopsy were 93% and 94% respectively for frozen section analysis.
Our study shows that SLN biopsy in cN0 neck of patients with oral cavity and oropharyngeal carcinoma is both feasible and accurate. Provided that larger studies confirm our results, an elective neck dissection may become unnecessary if fine-sectioned frozen-section analysis of the SLN shows no nodal metastases in patients with cN0 oral cavity and oropharynx carcinoma.
Furthermore, the risk of occult nodal metastases in patients with squamous cell carcinoma of the oral cavity and oropharynx in the clinically negative neck has been reported between 25% and 45%. 3 - 6 Performing an elective neck dissection in all patients with cN0 neck implies that more than half of all patients are overtreated and exposed to a potential unnecessary morbidity. 7 , 8
The sentinel lymph node (SLN) is the first node to receive drainage directly from the primary tumor site; it is therefore the initial possible recipient of metastatic tumor cells and may predict the histopathologic status of the remaining lymphatic area. 9 Identifying and analyzing the SLN may aid in the selection of patients who will benefit from further surgical treatment of the neck. This concept has already been applied and proven in the management of malignant melanoma and cancer of the breast. 10 , 11 The objectives of this study were 1) to analyze whether the SLN can be identified by lymphoscintigraphy and the use of a gamma probe in all patients enrolled, 2) to assess the accuracy of fine-sectioned frozen-section analysis to detect occult metastases in the SLN, and 3) to determine the predictive value of sentinel lymph node evaluation for the presence or absence of occult metastatic neck disease in squamous cell carcinoma of the oral cavity and oropharynx.
MATERIALS AND METHODS
From March 2002 to August 2003, a total of 31 patients, 16 men and 15 women, with squamous cell carcinoma of the oral cavity (n = 25) and oropharynx (n = 6) were enrolled in a prospective study. Ages ranged from 46 to 84 years, with a mean age of 66 years. All patients provided appropriate written consent as approved by the corresponding Ethics Committee. Inclusion criteria for this study were as follows:
Patients with T1 to T3 histologically confirmed squamous cell carcinoma of the oral cavity or oropharynx. Absence of suspicious metastatic lymph nodes in the neck on clinical examination, on computer tomography scan (CT), and on ultrasound examination. Lymph nodes greater than 1.5 cm in level II and greater than 1 cm in the remaining levels, round shape, central necrosis, and peripheral enhancement were considered pathological.
Exclusion criteria included prior radiotherapy in the head and neck region and/or neck surgery, pregnancy, or lactation.
Lymph node mapping of the neck was acquired preoperatively by lymphoscintigraphy and intraoperatively by the use of a hand-held gamma probe. A day before surgery, lymphoscintigraphy was performed in the department of nuclear medicine and consisted of injecting 15 MBq of technetium Tc-99m-labeled colloidal human serum albumin (Nanocoll, Amersham Health, Piscataway, NJ) into each quadrant around the tumor edge by the otolaryngologist. A total of 60 MBq diluted in 0.4 mL of isotonic sodium chloride solution was applied. Spillage of the radiocolloid in the mouth was avoided to reduce contamination of the oral cavity and oropharynx by asking all patients to use a mouth-wash after injection. Dynamic lymphoscintigraphy of the head and neck region (Gamma camera, Skylight, ADAC Laboratories, Philips, Milpitas, CA) in the antero-posterior projection was performed during the next 20 minutes followed by static acquisitions in the lateral and antero-posterior projections at 30, 60, and 120 minutes after injection of the radiocolloid. In cases where the SLN was not detected after the static views, additional oblique views were performed. The SLN(s) was then identified using a gamma probe (C-Track, Care Wise Medical Products Corporation, AEA Technology, Mergan Hill, CA) and its location marked on the skin using indelible ink.
Patients were taken to the operating room the next day, placed under general anesthesia, and prepared for surgery. The primary tumor site was always excised before the cervical lymph nodes to decrease background radioactivity. Shielding the primary tumor site with a malleable sterilized lead plate further reduced the radioactivity signal.
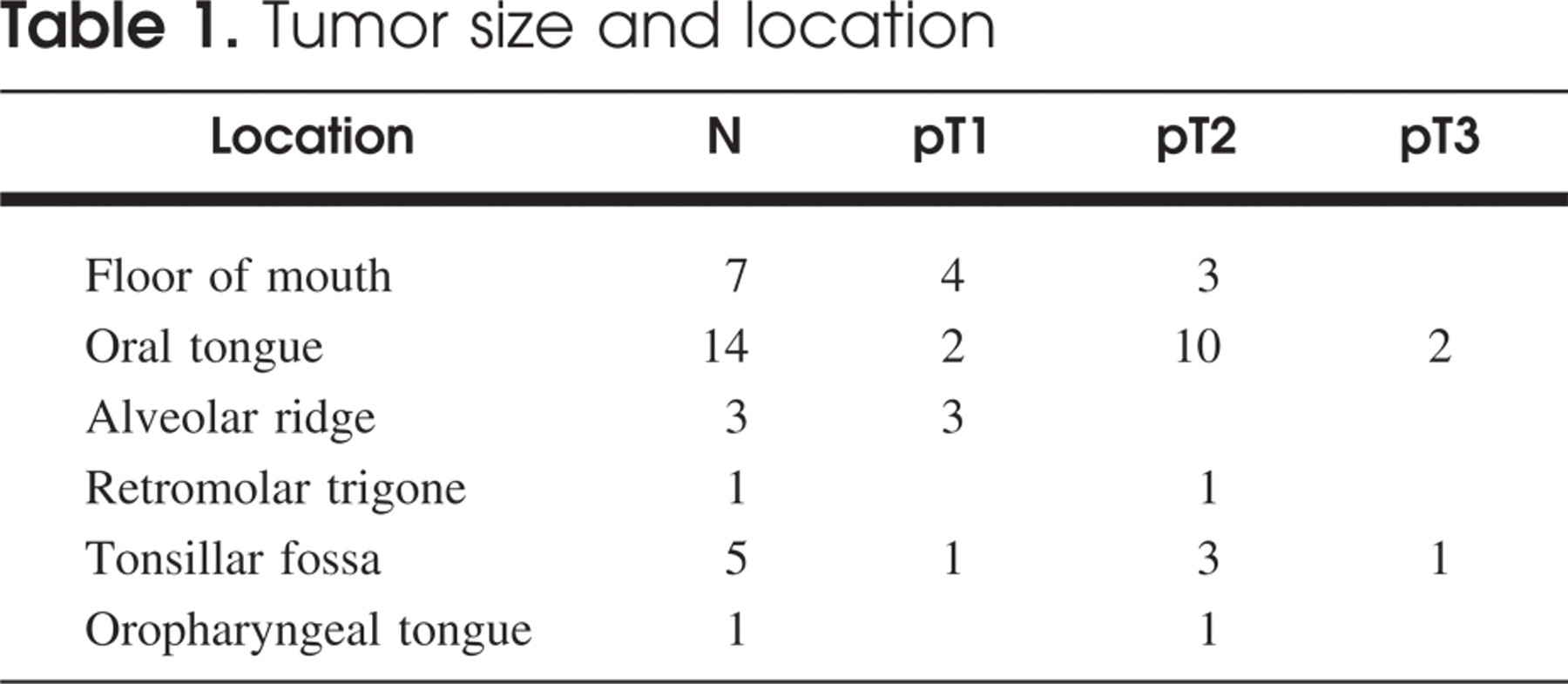
Tumor size and location
Every excised SLN was specially transected every 1 to 2 mm to provide slices for fine-sectioned frozensection histologic examination. The remaining transected tissue of the sentinel nodes was then fixed in a 4% neutral buffered formalin solution, embedded in paraffin, and further cut to obtain 3 more slices for hematoxylin-eosin staining and 2 slices for pancytokeratin immunohistochemical staining.
The neck dissection specimens were fixed in 4% neutral buffered formalin solution and carefully searched for lymph nodes. Every single identified lymph node was then cut to provide 1- to 2-mm slices, embedded in paraffin, and further trimmed to provide 3 slices for hematoxylin-eosin staining.
RESULTS
The primary tumor site and the tumor size are summarized in Table 1. Lymphoscintigraphy demonstrated a SLN in all patients. The SLNs were visualized during the dynamic sequences within 15 minutes after tumor injection with the radiocolloid in 30 cases. In only one patient the SLN, located very close to the primary tumor site, was detected 3 hours after injection in an oblique static imaging view. Bilateral lymph drainage occurred in 3 patients with a primary tumor site located in the midline or close to it. The mean number of SLN per patient detected by lymphoscintigraphy was 2.2, and ranged from 1 to 4 per patient. Twenty-eight patients (90%) had a sentinel lymph node biopsy (SNB) performed unilaterally and 3 (10%) bilaterally. The intraoperative mean number of SLNs identified and excised using the hand-held gamma probe was 2.7 (1-5 per patient).
The mean time to evaluate the SNL by fine-sectioned frozen section by an experienced pathologist was 22 minutes (macroscopic evaluation and cutting 3 minutes, technical work 11 minutes, microscopic evaluation 5 minutes, and telephone call and information 3 minutes). Depending on the number of SNLs, time ranged between 15 to 30 minutes.
Fine-sectioned frozen-section analysis of the SLNs demonstrated occult metastatic disease in 16 out of 82 sentinel lymph nodes, upstaging 14 out of 31 patients (45%) from cN0 to pN+. Further lymph node micrometastases in 2 cases were detected on hematoxylineosin staining of the remaining tissue of the SLNs that were not identified by fine-sectioned frozen-section analysis. One patient had a metastasis detected by fine-sectioned frozen-section analysis in a second SLN. Thus, one further patient had to be upstaged from cN0 to pN+. The immunohistochemical analysis of the SLNs revealed no further metastases. Finally, 15 out of 31 patients (48%) were upstaged from cN0 to pN+.
A total of 34 neck dissections in 31 patients were performed. An average of 38 lymph nodes per neck dissection specimen were analyzed. Of all 1295 examined lymph nodes, only one further lymph node containing a micrometastasis, near a positive SLN, was found.
In summary, fine-sectioned frozen-section analysis of the SLN upstaged 12 patients from cN0 to pN1 and 2 patients from cN0 to pN2b. After further histologic analysis of the remaining tissue of the SLN, an additional patient was upstaged from cN0 to pN1. Only one patient with a positive SNB was upstaged from pN1 to pN2 after histologic analysis of the neck dissection specimens. The true sensitivity and negative predictive value of the SLN biopsy using fine-sectioned frozensection analysis were 93% and 94%, respectively, and 100% in permanent histological analysis.
DISCUSSION
Lymphoscintigraphy has been shown in the literature to be a fairly reliable method of detecting sentinel lymph nodes. Nieuwenhuis et al 12 demonstrated a drainage pattern in 78 out of 82 patients with head and neck cancer using lymphoscintigraphy. In this large study, the SLN was visualized within the first 20 minutes after dynamic imaging in 73 out of 82 (89%) patients. In our series, the identification of the SLN within the neck using lymphoscintigraphy was possible in every case, demonstrating an average of 2.2 SLN per patient. Regarding the time of visualization, the SLNs were identified within the first 15 minutes after the injection of the primary tumor site in 30 out of 31 (97%) patients. The lack of flow of the tracer in 4 patients in the Nieuwenhuis series probably arises from the proximity of the SLN to the primary tumor or injection site and underlines the importance of late static oblique views to detect a SLN close to the primary tumor site as demonstrated in our study.
During sentinel lymph node biopsies we often encountered 2 SLN in close proximity even though the images of the lymphoscintigraphy disclosed only one hot spot in the area where the SLN were excised. An average of 2.7 SLN per patient were excised, more than those demonstrated by lymphoscintigraphy.
Identification of the SLN in cancer of the head and neck may be more demanding compared to other tumors and body areas such as for melanoma or breast cancer. The close proximity of the SLN to the primary site, especially when the primary site is in the floor of the mouth, makes identification of the radioactive nodes in level I difficult. To provide a more accurate and faster identification of the SLN, Hyde et al 13 defined specific anatomical points using a computer's electronic marking facility and a 57 Cobalt pencil during lymphoscintigraphy. Thereafter, they electronically fused the electronic images with those obtained by lymphoscintigraphy to generate an anatomically referenced image. We believe that this method can significantly facilitate and reduce the excision time of the SLN. The use of PET/CT fusion will eventually make the identification of the SLN faster and more accurate, the more accessible this technology becomes. 14 , 15
The main goal of fine-sectioned frozen-section analysis of the SLN is to determine whether occult metastatic disease is present in cN0 patients and to potentially avoid an unnecessary neck dissection, causing a better cost-effectiveness and a lower morbidity. We consider an intraoperative waiting time of 22 minutes for the analysis of fine-sectioned frozen section of the SNL not to be a significant factor for costs and morbidity; with 45% occult metastasis in our series we have found a higher rate of metastasis in cN0 than previously reported, and this shows the importance of fine-sectioned frozen-section SNL analysis to eventually guide the necessary additional therapy requirements in each particular case. Nevertheless, the reliability of frozensection analysis of the SLN has yet to be studied extensively.
Conventional frozen-section techniques do not yield very good results. In a series of 18 patients Civantos et al 14 found 4 SLN to be negative on frozen section and positive after full pathologic analysis. In their study, frozen-section analysis was performed with only 2 cuts through the sentinel lymph node, easily overlooking micrometastases. Performing fine-sectioned frozen-section analysis of the SLN (transected every 1-2 mm) in our study failed to detect metastatic disease in only one case. Further histological analysis of the remaining tissue of the SLN confirmed one more micrometastasis, upstaging the cN0 neck to pN+. Thus detecting occult metastatic disease in the neck by fine-sectioned frozen section of the SLN yields results as accurate as the histological analysis of the neck dissection specimens. 3 - 6
The surgical neck dissection technique and the histological workup of neck dissection specimens are very important to determine the future accuracy of SLN biopsies. The significance of a disease-free SLN increases if large numbers of lymph nodes have been excised and examined in each neck dissection specimen. This point was emphasized by Koren et al 16 in a series of 21 patients. They described a “lymph node revealing solution” that helps to detect small lymph nodes in neck dissection specimens. At first, the entire surgical specimen was searched for lymph nodes using the traditional method. Thereafter, the remaining tissue was treated with the “revealing solution,” allowing 72 further lymph nodes from 21 neck specimens to be examined. Among them, 8 lymph nodes were positive for metastatic disease and 2 cases were upstaged from pN0 to pN1. In their study, an average of 15 lymph nodes per neck dissection specimen were analyzed. In our study, an average of 38 lymph nodes per neck dissection were identified and analyzed. This great result is due to the close collaboration between the same motivated and experienced pathologist and surgeons. The evaluation of the SLN biopsy should be performed by an experienced team.
With a true sensitivity of 93% after fine-sectioned frozen sections and 100% after full histological analysis, our results are similar to those of other authors 17 , 18 who performed SLN biopsy without frozen-section analysis and a neck dissection in a second stage if needed.
It is also important to underline that most of the neck dissection specimens with the SLNs found to be positive for metastatic disease did not disclose any further lymph node metastases in the neck dissection specimens.
CONCLUSION
The SLN biopsy in head and neck cancer is a feasible method. With a sensitivity of 93%, fine-sectioned frozen-section analysis of the SLN will be a reliable method to determine if a neck dissection is further indicated. Our one-stage procedure concept is more cost-effective and carries less morbidity compared to the full histological analysis of the SLN biopsy and a possible elective neck dissection in a second step.
We gratefully acknowledge the Cancer Foundation of Bern, Switzerland, for their financial support in this study.