
Abstract
At the beginning of the 20th century, the major complications of thyroidectomy were hematoma and postoperative infection, and most publications reported some postoperative mortality. 8 , 10 , 11 Currently, the main postoperative complications are vocal cord palsy due to dysfunction of the recurrent laryngeal nerve and hypocalcemia. Postoperative death is rare or even unrecorded. 3 , 8 , 10 – 13 The incidence and severity of complications are linked to the experience of the surgical team and the extent of the operation. 11 , 14
The main purpose of this article is to evaluate the incidence and risk factors of complications in patients undergoing thyroidectomy in a cancer hospital with a surgical residency training program, with a view to propose preventive measures that can result in reduction of costs, period of hospitalization, as well as improvements in the patient's quality of life.
PATIENTS AND METHODS
Between January 1990 and December 2000, 1020 patients underwent thyroidectomy in the Head and Neck Surgery and Otorhinolaryngology Department of the Centro de Tratamento e Pesquisa Hospital do Câncer A C Camargo, in São Paulo, Brazil. There were 888 (87%) female patients and 132 (13%) male patients, with a mean age of 46 years (range, 2 to 88 years). Preoperative evaluation included clinical history and physical examination, thyroid function tests, and radiography of the thorax. All patients had preoperative evaluation of vocal cord mobility by means of indirect laryngoscopy.
The indication for thyroidectomy included 702 (69%) benign thyroid diseases and 318 (31%) malignant tumors. Most surgeries were performed by 3rd to 5th year residents under the supervision of 10 different head and neck surgeons. Surgeons were stratified according to the total number of thyroidectomies they performed or supervised during the study period: Group A (1 to 50 thyroidectomies), group B (50 to 100), and group C (over 100). We routinely identified the parathyroids and recurrent laryngeal nerves before performing the ligation of the inferior thyroid pedicles. An autotransplant of the parathyroid in the sternocleiodomastoid or anterior scalene muscle was performed every time there was vascular supply injury or the glands were accidentally removed. The use of surgical drains varied throughout the study period. Penrose drains were used initially, but it was replaced in 1992 by Hemovac closed drainage to facilitate postoperative care and permit earlier discharge from the hospital. Since 1995, at the surgeon's discretion, the operative wounds of 178 selected patients were not drained. Drains were not used in 138 patients undergoing lobectomy with isthmusectomy, in 14 lobectomy, in 8 subtotal thyroidectomy, in 13 partial lobectomy, and 5 completion of thyroidectomy.
All patients were evaluated with regard to the occurrence of postoperative complications. We routinely performed indirect laryngoscopy or nasofibroscopy before the 30th postoperative day. Recurrent laryngeal nerve dysfunction, hypoparathyroidism, and other complications are analyzed according to the number of operations, type of thyroidectomy, and whether or not drains were used. Postoperative vocal cord palsy was defined as the presence of immobility or decreased movement of the vocal cords. A persisting vocal cord dysfunction after 6 months was considered permanent. Palsies that resulted from inferior laryngeal nerve resection due to neoplastic involvement were considered as sequelae and not computed as complications. Hypocalcemia was considered whenever there was a need for exogenous calcium replacement in order to maintain normal serum levels (8 to 10.4 mg/dL) or to eliminate the clinical signs and symptoms of hypocalcemia. Hypocalcemia was considered permanent when calcium replacement was necessary for over 6 months.
The association between the studied variables with the occurrence of complications was evaluated by the Chi-square test, or Fisher's exact test when applicable. Values of P < 0.05 were considered significant.
RESULTS
Post-thyroidectomy complications
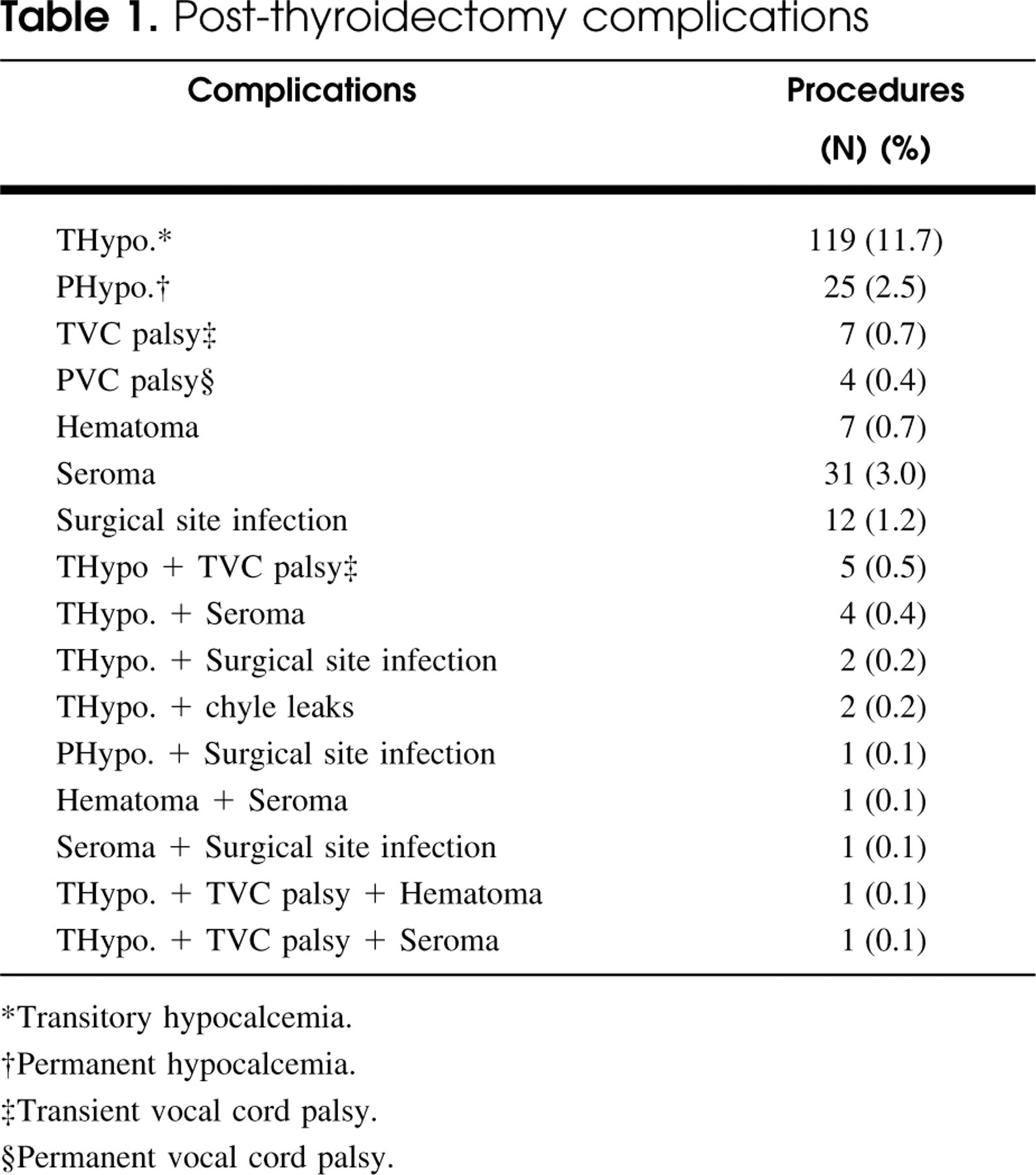
∗Transitory hypocalcemia.
†Permanent hypocalcemia.
‡Transient vocal cord palsy.
§Permanent vocal cord palsy.
The mean duration of hospital stay was 2 days (range, 2 to 30) for the 702 patients with benign tumors and 3 days (range, 2 to 19) for the 318 patients with a malignant tumor. However, complications were most significantly associated with thyroidectomy performed for the treatment of malignant disease (P < 0.05), with hypocalcemia as the most frequent complication. Other less frequent complications were vocal cord palsy, hematoma, seroma, and surgical site infection (Table 1).
The overall rate of vocal cord palsy was 1.8% (Table 2). Transitory palsy occurred in 14 patients with full recovery occurring within 6 months. Four patients had permanent vocal cord palsy. There were no bilateral palsies nor was there a need for tracheotomy. The type of thyroidectomy, the surgeon's experience, patient's gender, diameter of the nodule, and the association or not with neck dissection did not have any significant association with the incidence of vocal cord palsy.
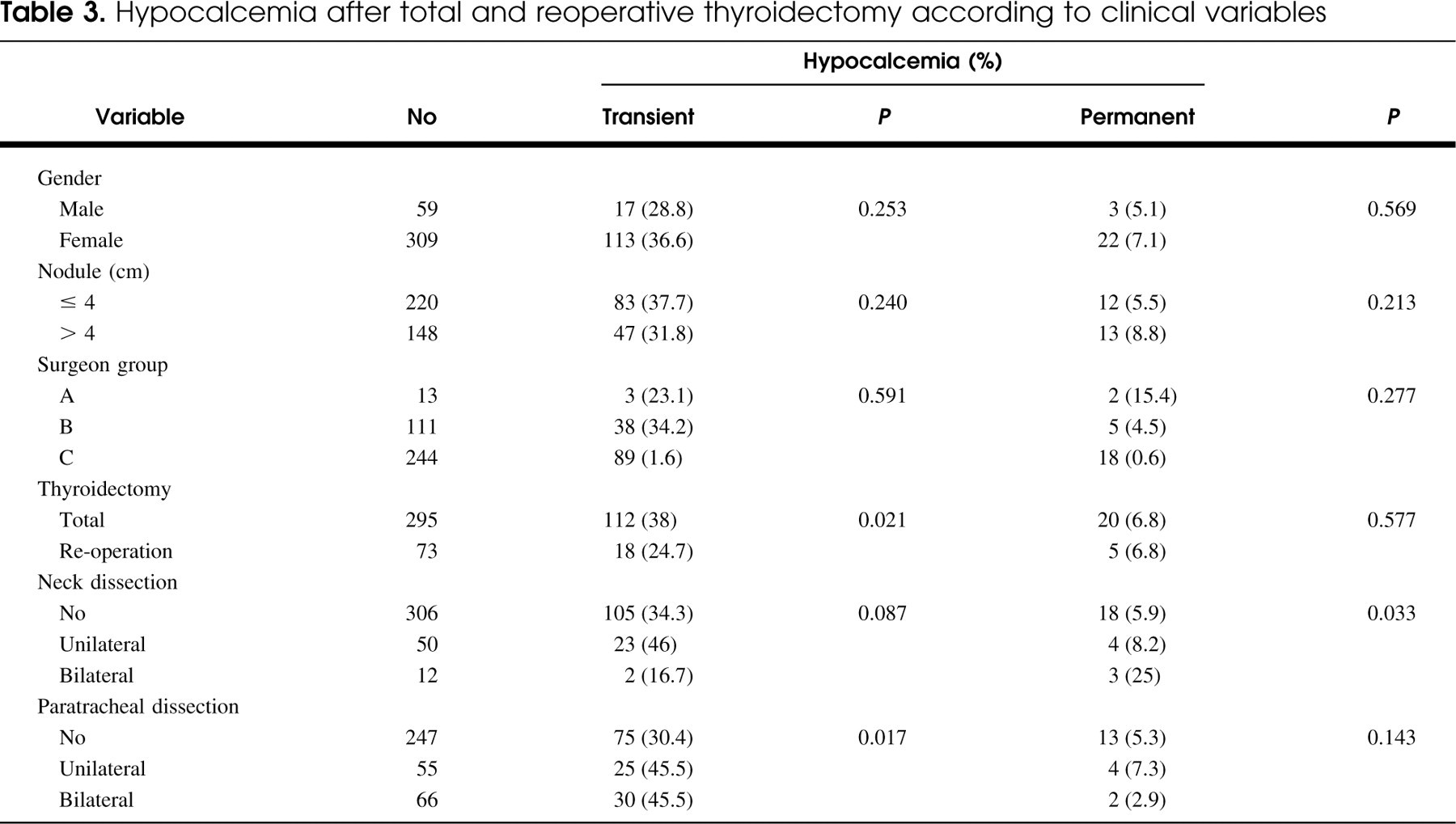
Postoperative hypocalcemia occurred in 15.6% patients (Table 2). Permanent hypocalcemia occurred in 26 patients (2.5%) and transitory hypocalcemia was found in 134 (13.1%) patients. The rates of postoperative hypocalcemia was higher after total thyroidectomy as compared with other procedures (Table 2). Temporary hypocalcemia was significantly associated with total thyroidectomy (P = 0.021) and paratracheal lymph node dissection (P = 0.017). In the same way, neck dissection was significantly associated with permanent hypocalcemia (0.033) (Table 3). There were no significant associations among surgeons classified per number of thyroidectomies performed or supervised and temporary or permanent hypocalcemia rates. Similarly, there was no significant association of hypocalcemia with gender or nodule diameter (Table 3).
Extent of thyroidectomy and complications
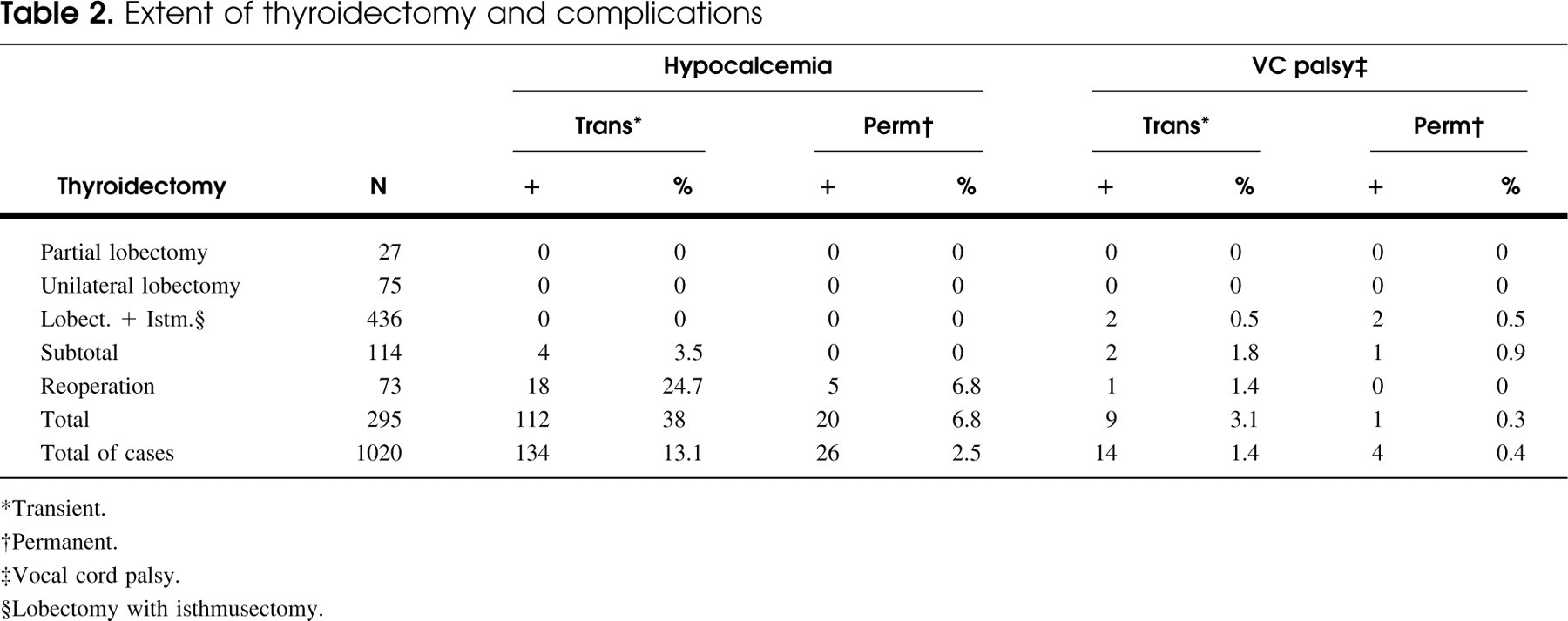
∗Transient.
†Permanent.
‡Vocal cord palsy.
§Lobectomy with isthmusectomy.
Seroma was a postoperative complication found in 38 (3.7%) patients. Seroma developed in 8 (3.6%) of 222 patients drained with a Penrose drain, 22 (3.5%) of the 622 drained with Hemovac, and 8 (4.5%) of the 178 patients in whom no drain was placed. Sixteen (1.6%) patients developed postoperative surgical site infections. Nine (0.9%) patients were reoperated on as a result of a hematoma. Chyle leaks occurred in 2 (0.2%) patients undergoing neck dissection. No significant differences were observed between these complications and the presence of drain, type of thyroidectomy, and number of thyroidectomies performed or supervised by the surgeon (P > 0.05).
DISCUSSION
Thyroidectomy is a very common therapeutic procedure worldwide and is performed by surgeons with varied training and backgrounds: general surgery, thoracic surgery, endocrine surgery, otolaryngologic surgery, oncologic surgery, and head and neck surgery. The Head and Neck Surgery and Otorhinolaryngology Department of the Centro de Tratamento e Pesquisa Hospital do Câncer A C Camargo is part of a surgical oncology training program, where the greater part of such operations are performed by 3rd to 5th year residents in surgical oncology or head and neck surgery fellows under the direct supervision of a head and neck surgeon. Although some reports 11 , 14 in the literature relate the complications of this operation directly to the surgeon's experience, there are also several reports 3 , 4 , 11 , 15 – 17 that point out the safety of this operation performed at residency training centers, with acceptable complication rates, when performed under the supervision of an experienced surgeon. In our study, 69.7% of the thyroidectomies were performed by 4 surgeons, 27.3% by 3 surgeons, and 3% by 3 surgeons. However, no statistically significant differences were observed between the groups. These results differ from other reports possibly because it is a single institution experience. All the members of the staff have similar backgrounds and the junior assistants are constantly supervised by more experienced surgeons. Similarly, Bergamaschi et al, 18 in a series of 1192 thyroidectomies performed by 11 surgeons, also did not observe significant differences between patient volume per surgeons and the complication rates.
There has been a significant reduction in the incidence of complications and mortality in thyroid surgery since the beginning of the 20th century, currently making thyroidectomy a surgical procedure with low acceptable morbidity and mortality rates. Postoperative mortality with thyroidectomy has become an extremely unusual complication. 4 – 7 , 10 , 13 , 14 , 19 , 20
Postoperative death was also not observed in our series. Pederson et al 15 had 0.4% deaths and Herranz-Gonzalez et al, 21 in a series of 335 thyroidectomies, observed a mortality rate of 0.8%. The rates of postoperative complications reported in literature are variable (7.4% to 53%). 3 – 5 , 10 , 15 In our series, we observed postoperative complications in 226 (22.2%) patients, the most frequently found complication being hypocalcemia.
Hypocalcemia after total and reoperative thyroidectomy according to clinical variables
The most common and feared complications in thyroid gland surgery are vocal cord palsy and hypocalcemia, and there are various factors involved in their occurrence. 4 , 5 , 10 , 18 , 21 – 23 The incidence of recurrent laryngeal nerve injury found in literature vary from 0% to 4.8%, 3 , 4 , 15 , 17 , 19 , 21 and are greater in extensive resections and in the cases of reoperation. 5 , 6 , 8 , 13 , 14 In our series, only 4 patients (0.4%) showed permanent vocal cord palsy. We observed that the patients with transitory vocal palsy presented recovery of the normal vocal cord mobility within 6 months. The patients who remained with vocal cord palsy for more than 6 months continued after 1 year of follow-up without improvement in the vocal cord mobility. Two patients showed an improvement in the dysphonia for discrete hoarseness and 2 other patients evolved with moderate hoarseness. Pezzullo et al 8 found permanent vocal cord palsy in 2.8% of the cases. Chao et al 20 observed a 2.6% incidence of transitory palsy and a 1.7% rate of permanent vocal cord palsy in cases of reoperation for benign and malignant neoplasias. In our group, the dissection and identification of the recurrent laryngeal nerve is performed as a routine manner before the ligation of the inferior pedicle vessels, thus reducing the risk of nerve injury. This early identification of the recurrent laryngeal nerve is also advocated by several other authors. 3 , 11 , 13
Hypocalcemia was an important complication in our series (13.1% transitory and 2.5% permanent). On reviewing recent thyroidectomy literature, we found an incidence of symptomatic postoperative hypocalcemia ranging from 4% to 42%. 3 , 5 , 6 , 10 , 15 , 18 , 21 , 23 In this series, all the patients with transitory hypocalcemia were treated with oral calcium or vitamin D analog supplementation for a period of 1 to 6 months. However, all the patients that needed supplementation for more than 6 months presented permanent hypocalcemia. In the same way, in 1998, Lo et al 24 reported in their series that of 35 patients with transitory hypocalcemia only 3 (8.5%) patients needed a calcium supplement after 6 months. In the same year, Pattou et al 25 in a prospective study observed that all patients with transitory hypocalcemia became normocalcemic within 1 week to 6 months after thyroidectomy. Permanent hypocalcemia occurs with a lower incidence (0% to 8%). 3 , 4 , 7 , 10 , 11 , 15 , 21 , 23 Neck dissection and paratracheal dissection (ipsilateral or bilateral) were the most important risk factors for the occurrence of hypocalcemia. Paratracheal dissection has been implicated in the increase of the risk of both vocal cord palsy and postoperative hypocalcemia. 3 , 8 , 21
In view of the results of this study, we conclude that thyroidectomy, whether or not associated with neck dissection, is an operation that has low morbidity with hypocalcemia as the most important postoperative complication. Paratracheal lymph node dissection was the most significant predictor of hypocalcemia in patients who underwent total thyroidectomy. Thyroidectomy may be safely performed in resident training centers, provided that it is performed under the supervision of an experienced surgeon.