
Abstract
This hearing impairment, occurring in a sensitive and critical period during which the child learns to understand and produce language, is suggested to be responsible for adverse effects on speech and language development. Fluctuation in hearing, which is typical of recurrent middle ear diseases, may cause even more problems than a stable mild hearing loss. 6 Because learning to read and spell is dependent on language development, educational problems could also be expected to arise. 7
It has been proposed that any difficulties in speech and language attributed to otitis media-associated hearing loss may become particularly evident when a child reaches school age. Academic skills, particularly language-based subjects like learning to read and spell, may then be affected. 8
Bond, 9 as early as 1935, reported a sample of 128 children in New York schools and noted that hearing loss was approximately 15 times more common among children who were having reading problems than among those whose reading performance was normal. Since this pioneer study, much interest has been expressed in the effects of otitis media and middle ear effusion on speech and language development. Despite extensive literature suggesting a relationship between otitis media in early childhood and later learning problems, controversy exists whether this link is casual. 10
Several studies have demonstrated that middle ear disease is associated with significantly lower reading scores and academic achievement in school. 1 , 4 – 6 , 11 – 13 Other studies have found no such correlations or only minor effects of middle ear disease in early childhood on later learning and academic achievements without any significant importance. 2 , 3 , 7 , 8 , 14 – 19
Lous 2 reviewed 19 studies aiming to answer the question: “What is the evidence of sequelae from otitis media on reading abilities?” The studies reviewed gave inconsistent and often disparate and contradictory results, partly because of numerous different methodological problems. In most of these studies, the correlations that has been found between middle ear disease and reading skills were so small that they were found to have no practical importance.
The study presented herein was designed to assess the effects of early recurrent or persistent middle ear problems with their associated hearing loss on reading performance among first and second graders. We also studied the time the children spent with MEE, the degree of the hearing impairment, and the number of episodes of AOM, and estimated their contribution to the scores of the reading tests. Similar studies were performed by other researchers among English-speaking and among non-English-speaking children from different countries, but never have been performed before on Israeli, Hebrew-speaking children.
SUBJECTS AND METHODS
Eighty children were included in the study group ranging in age from 6.5 to 8 years. They were selected from a large group of more than 2,000 children who were consistently followed at the Department of Otolaryngology-Head and Neck Surgery at the Rambam Medical Center due to recurrent episodes of AOM or prolonged periods of MEE. Middle ear diseases were the only medical problems of these children who were otherwise completely healthy and normal. Only children who met the following criteria were selected from the large ‘otitis media' group, and were included in the study: their medical records showed systematically documented middle ear diseases, both parents were born in Israel and their mother tongue was Hebrew, Hebrew was the only language used at home and in the kindergartens, high parental level of education (college/university), upper-middle socioeconomic status as determined by family income, area of residence, and parental professional status.
Data was collected from the medical records of these children regarding the number of episodes of middle ear infection, the duration of effusions in the middle ear, the results of the hearing tests and tympanometry, and the various treatments given to these children. Only children who had at least 10 episodes of AOM during their first 5 years of life and/or prolonged periods of MEE with an average hearing loss for the speech frequencies range (500–2000 Hz) of 25 dB or more, or speech reception threshold (SRT) of at least 25 dB, were enrolled in the study.
In all of the children, middle ear pathology was most of the time bilateral. These children were carefully matched with 80 healthy children with no previous middle ear diseases, from the same schools and classes, based on age, gender, and socioeconomic status (based on information about parental level of education, occupation, and income). Hebrew was the only language used at home. Subjects with previous diagnosis of learning disabilities were excluded.
Informed consent was obtained from the parents of the children in both groups. Upon entering the study, before reading ability was assessed, both the children in the study group and the control subjects underwent a neurological and ophthalmological evaluation to exclude possible neurological or visual dysfunction that may affect reading. Subsequently, a complete otorhinolaryngological examination, pure tone audiometry for air and bone conduction, SRT, and tympanometry were performed. Each child underwent 5 special reading tests designed by Dr. Balgur and Mr. Karni for Hebrew-speaking children. These tests were performed twice during the period of the study in an interval of 4 to 6 months, at the end of the first year and during the second year in school. The tests were presented to the children by a qualified special education teacher and a speech pathologist. Both were unaware of the children's history of middle ear diseases or the results of the previous and the recent audiological findings. The total number of possible reading mistakes in all of these tests was 160. Achievement in reading was determined as the ratio between the child's reading score (number of mistakes made) and a predicted reading score based on the child's age and school grade (number of possible mistakes) expressed in percentages. Analysis of the results obtained from the reading tests in both groups was done by the Student t-test.
RESULTS
In both the study and the control groups there were 40 boys and 40 girls. The average age of the children in the study group was 7.3 ± 0.33 years, and the average age of the controls was 7.4 ± 0.28 years (not statistically significant). The children of both groups and their parents were born in Israel, the language used at home was Hebrew, and all had a rich home language environment. All the children came from Ashkenazi families (grandparents coming from Western Europe or North America) of upper-middle socioeconomic status.
Reviewing the medical records of the study group children, who were consistently followed in our outpatient clinic, revealed that 27 have had from 10 and up to 30 episodes of AOM, treated with different antibiotics, and 34 children have had only MEE, with no AOM episodes, lasting from 3 and up to 10 months, treated with antihistamines, decongestants, steroids, and antibiotics. Nineteen children have had recurrent episodes of AOM with prolonged periods of MEE between the infections.
The average hearing loss of both ears of the ‘otitis children' during follow-up years
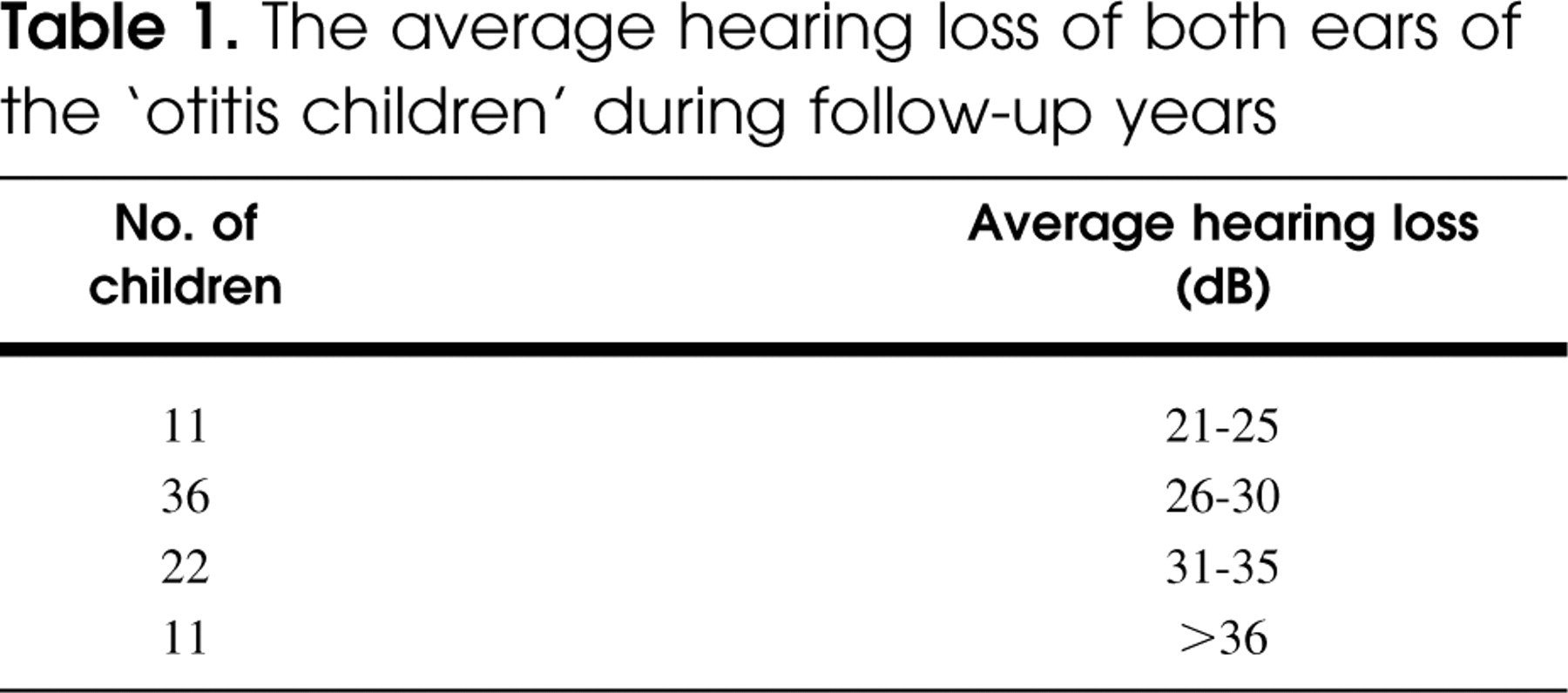
Each child underwent at least 7 hearing tests during this follow-up period (7–18 average, 12.2 ± 3.1). The average hearing loss at the speech frequencies of all the hearing tests performed on these children is summarized in Table 1. Most of the children (72.5%) had an average hearing loss in the range of 26 to 35 decibels. No significant difference was found between the average hearing level of the right and the left ear.
Neurological and ophthalmological examination revealed no abnormality or any pathological findings in all the children of both groups.
Upon entering the study, all of the children underwent a complete audiological evaluation prior to their reading ability assessment. Twenty-four children (30%) in the otitis group still had some hearing impairment, whereas the other children in this group and the control subjects had normal hearing thresholds (less than 20 dB). The average hearing threshold of these 24 children was 24.4 ± 3.5 dB, and the average hearing threshold of the rest of the ‘otitis children' and of the control subjects was only 12.3 ± 4.7 dB. All of the children in the control group had a type A tympanogram, whereas those of the study group had different types of tympanograms (A, B, and C).
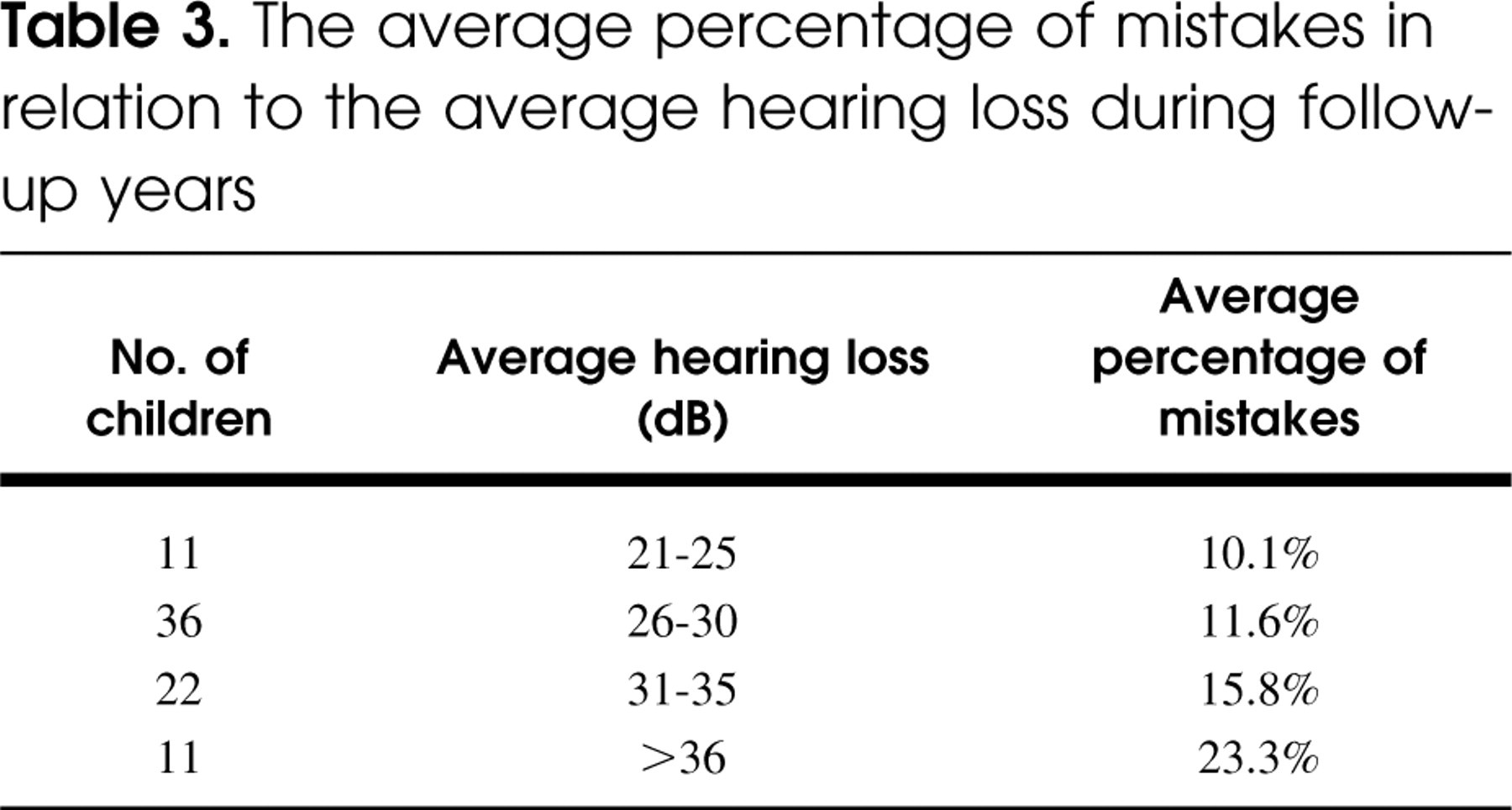
The average percentage of mistakes in the reading tests was 15.2% (SD = 4.6) for the children in the study group, as compared with only 5.8% (SD = 1.2) for the control subjects. An acceptable percentage of mistakes for children of the first and second school grades is considered to be 7%. The difference between these 2 groups is statistically significant (P < 0.001). The reading tests showed a significant trend toward impaired performance with increasing number of AOM episodes and with more severe hearing loss. Those children who had more than 4 episodes of otitis media per year, and the children who had average hearing losses of more than 31 dB, scored worse than those with less AOM episodes and those with an average hearing impairment of less than 30 dB (Tables 2 and 3).
The average percentage of mistakes in relation to the number of AOM episodes during follow-up years
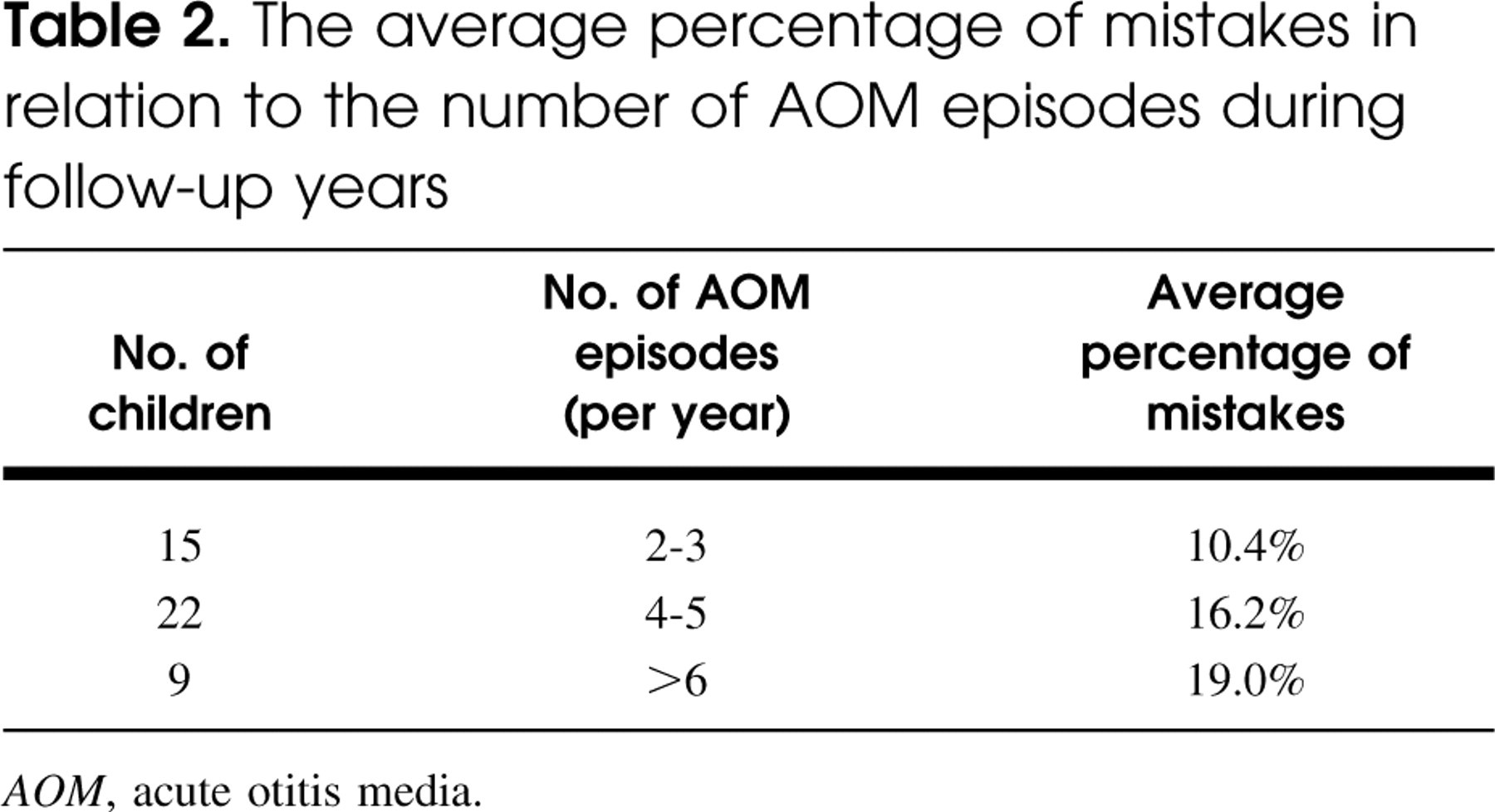
AOM, acute otitis media.
The average percentage of mistakes in relation to the average hearing loss during follow-up years
Comparing the scores of the children from different schools and classrooms, we found that reading performance did not differ from school to school and from classroom to classroom.
The 24 children from the study group that still had conductive hearing loss at the time of their reading assessment, did not perform less well than the other children from this group that had restored normal hearing.
Girls performed slightly better than boys in all reading tests and in both groups, but the differences were not statistically significant.
DISCUSSION
An early, much quoted study of Holm and Kunze, 20 from 1969, demonstrated a negative effect of otitis media on language development, reading, and academic achievements. There has since been an intensive debate in the literature about the degree of language disability that may result from otitis media and the linkage of history of early otitis media during childhood to later language, speech, reading, and academic skills is not as obvious today as it was in early studies. Recently reported studies have given mixed, inconsistent, and often disparate and contradictory results. 14 , 15
The results of this study are in accord with the results found by many other researchers 1 , 4 – 6 , 11 – 13 but are inconsistent with the results of others. 2 , 3 , 7 , 8 , 14 – 19
Our groups of ‘otitis-children' and control subjects were large enough to provide satisfactory statistical power. The study is free from any methodological bias, a problem reported by many researchers in previous studies, 2 because the children in this study represent relatively homogeneous groups with regard to age, gender, socioeconomic status, rich home language learning environment, and ethnical and cultural background, and because great care was taken to pair-match the subjects in each group. In view of the fact that the otitis children differ from the control subjects only in their previous middle ear diseases, the difference in reading skills between these groups can be attributed only to the presence or absence of early AOM and MEE and not to other causes.
Even though most of the otitis children had normal middle ears and restored normal hearing at the time of their reading assessment, they still performed less well than the control subjects who were free from middle ear diseases in their early childhood. Moreover, the children that still had conductive hearing loss at the time of their reading assessment did not perform less well than the children from the control group that had restored normal hearing. From this finding, we can conclude that previous middle ear pathology, with the associated various degrees of hearing losses, was actually responsible for the impaired performance in reading found in the study group children.
We found a clear-cut correlation between the number of AOM episodes, the duration of MEE, and the degree of hearing losses associated with these diseases, and the reading scores of the children. These results are similar to those found also by Teele et al 1 and by Luotonen et al, 13 but not to the findings of other studies. 17 We also did not find any significant differences in reading performance between boys and girls, in contrast to the finding of other researchers. 6 , 11 , 13 , 15 , 16
Some authors have found that middle ear diseases, if persistent enough during early childhood, may adversely affect children's language, speech, and academic achievements later in life well after they resolve and hearing returns to normal. A nation-wide Finnish study concluded that the detrimental effects of early otitis media may last in some cases up to the age of 9 years in spite of active treatment, 12 and a large longitudinal study from New Zealand found that otitis media in early life was associated with delayed reading ability even up to the age of 15 years. 21
On the other hand, the results of other studies 2 , 15 , 17 demonstrated that most children overcome the effects of otitis media as soon as the disease resolves, even when it has been long lasting, and whenever there are some detrimental effects of recurrent middle ear disease in children at school age, they appear to be minor, and in any event disappear during later years at school.
Follow-up studies using the same children from our study group in 2 to 4 years' time may reveal whether the differences in reading abilities between children with history of middle ear disease and healthy children will persist, or whether the otitis children will catch up in their reading skills once they will grow older.
CONCLUSIONS
The results of this study indicate that recurrent AOM and/or MEE during the critical early years of language development affect reading performance in the first 2 years of school. Recurrent middle ear disease in young children should be regarded therefore not only as a medical problem, but also as having a potential education risk for young reading beginners.
Parents of children with middle ear disease should be encouraged to provide a language-rich environment with intensive auditory stimulation to their children. This approach together with appropriate medical treatment can minimize the possibility of auditory deficits and reading problems in early school years.