
Abstract
To compare the swallowing frequency in patients with neurogenic dysphagia with or without tracheotomy tubes (TT) to assess the underlying mechanisms of dysphagia to improve rehabilitation strategies.
Prospective study, 10 patients (64 ± 7 years) with neurogenic dysphagia. Glasgow Coma Scale (GCS) less than 8 points, tracheotomy due to the dysphagia 2 weeks before the examination. The swallowing frequency (1 or less over 5 min) was assessed over 5 consecutive days with or without TT.
The swallowing frequency increased after removal of the TT. These findings did not influence the GCS or the Coma Remission Scale. Over a 5-day period, the frequency of swallowing was increased.
The influence of TTs on swallowing is discussed in the literature but remains controversial. A number of references 1 - 7 suggest that an inflated TT impairs swallowing. The results of clinical series are also conflicting. Leder et al 8 - 11 found no influence of TTs on aspiration (inflated and deflated as well). Other investigators could prove an influence of the TT status on swallowing. 12 - 15
Why do those studies give so contrasting results? On one hand, inhomogeneous patient samples (neurogenic dysphagia vs. dysphagia after excision of malignant tumors of the head and neck) were compared. On the other hand, the beginning of supplying the patients with a TT varied largely in all studies (i.e., supply with TT between 2 weeks and 6 months after the initial event). Finally, different clinical examination methods were applied to assess the influence of the TT on swallowing (e.g., endoscopy, fluoroscopy).
It was therefore the aim of the present study to examine the influence of a TT on swallowing among patients with neurogenic dysphagia during rehabilitation.
METHODS
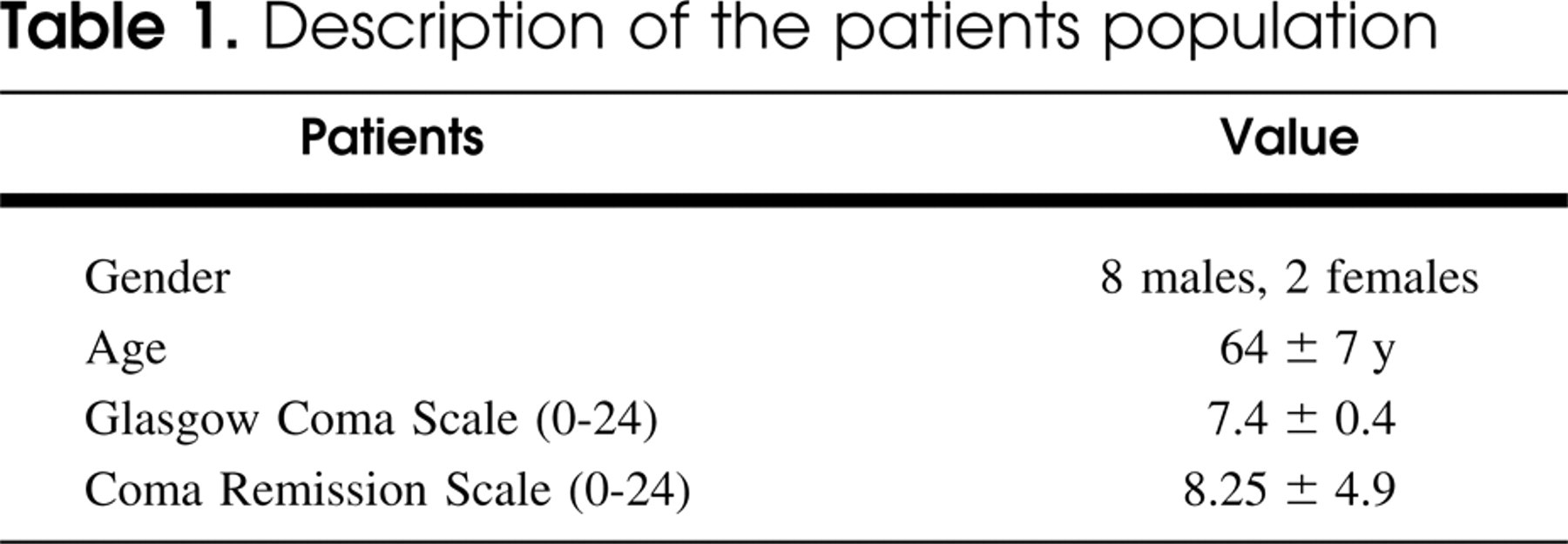
In a prospective study, 10 patients (64 ± 7 years, 8 male, 2 female) with neurogenic dysphagia due to stroke or head trauma were examined. All patients had less than 8 points on the Glasgow Coma Scale (GCS), the swallowing frequency was 1 or less in 5 minutes. These patients had undergone a tracheotomy due to dysphagia 2 weeks before the examination was started (Table 1).
The change in swallowing frequency (SF) was assessed as the major parameter of the study. The underlying neurogenic disorder excluded the application of additional invasive methods. The SF was assessed by counting the movement of the larynx over 5 min at 5 consecutive days with and without TT inserted. The observations were video taped and repeatedly evaluated by 2 independent investigators.
Description of the patients population
All patients or their relatives gave their informed consent to participate in the above study protocol. It was approved by the Free University of Berlin Institutional Review Board. Statistical significance was considered at P = 0.001 (Wilcoxon's test, SPSS 10.0).
RESULTS
Swallowing Frequency
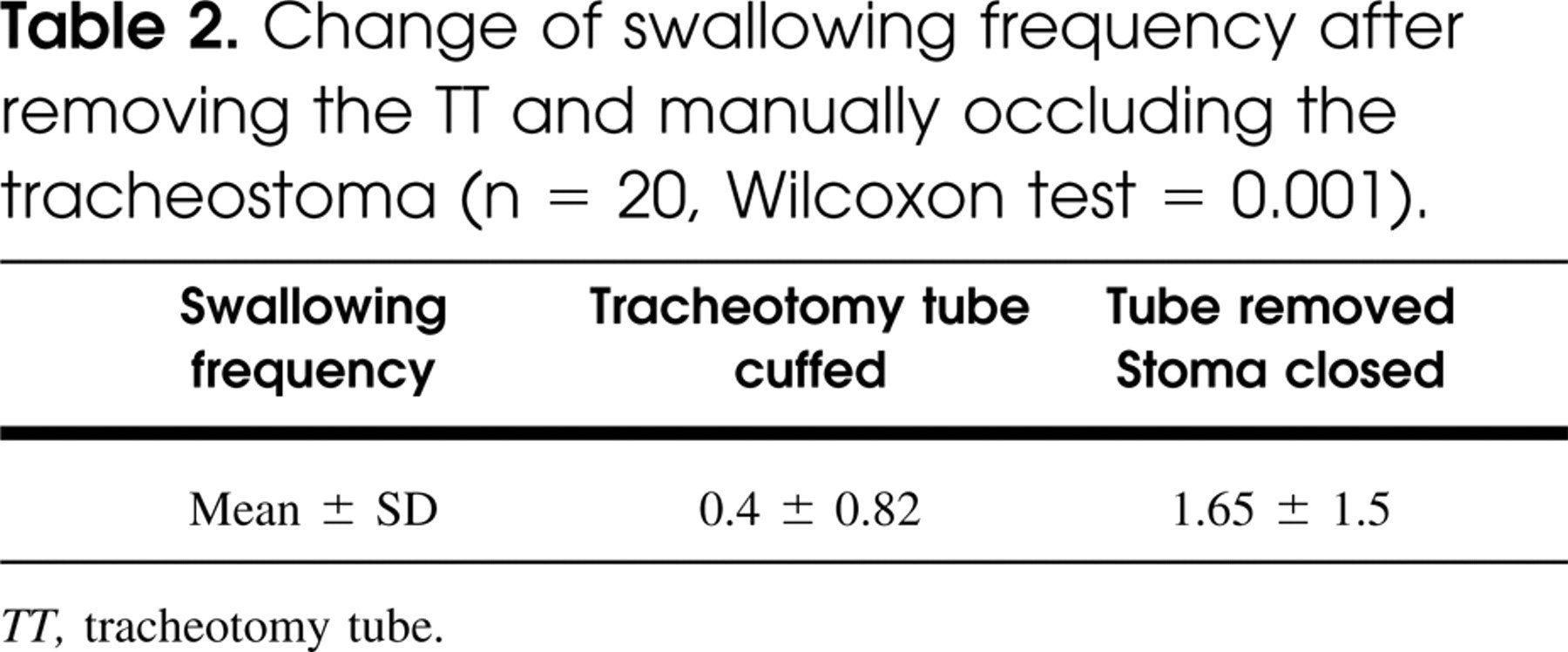
The result of 20 examinations shows a statistically significant increase in the SF after removal of the TT (Fig 1, Table 2). There was no statistical correlation between the SF and the different levels of consciousness of the patients as measured by the GCS and the Coma Remission Scale.
Changes in Swallowing Frequency
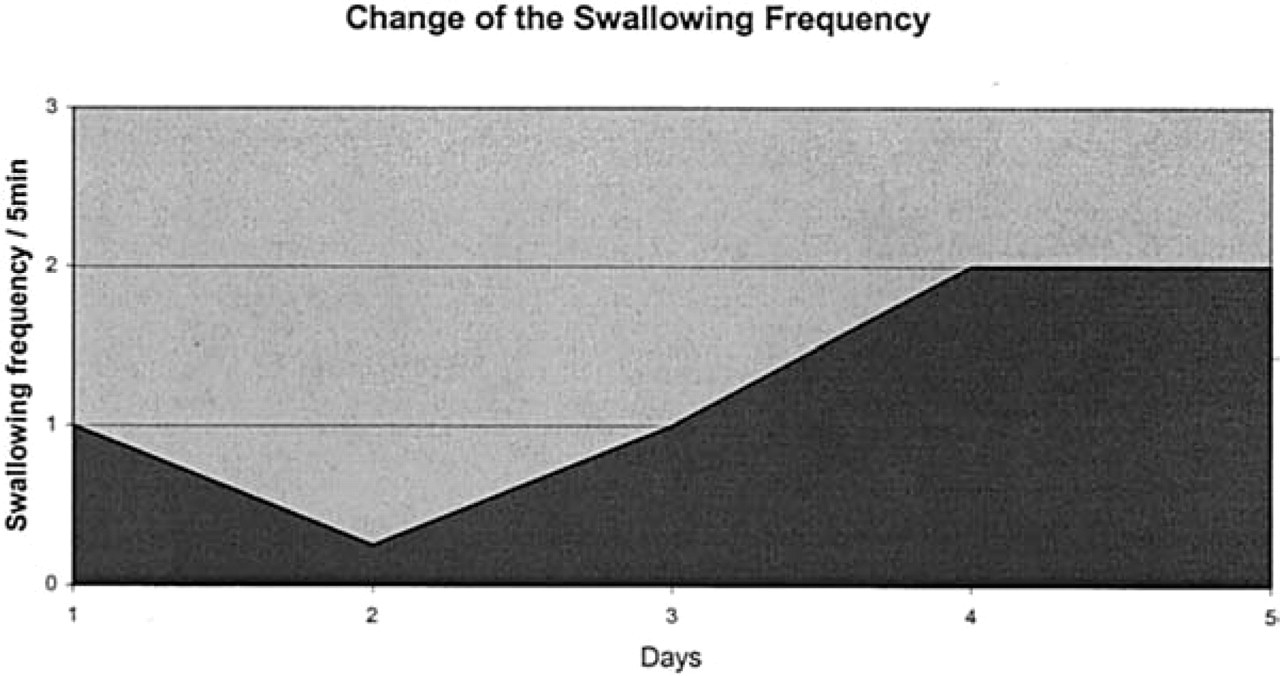
To exclude purely accidental findings, the examinations were repeated in each patient at 5 consecutive days of 1 week. This protocol demonstrated that the increase of the SF was reproducible. In addition, there is an increase in SF over the period of examination of 5 consecutive days (Fig 2).
DISCUSSION
There are contrasting and controversial reports in the literature on the dependence of TTs and swallowing:
Muz et al 12 found a decrease in aspiration in patients with cancer of the head and neck after deflating the cuff and occluding the TT opening. Dettelbach et al 13 and Stachler et al 14 confirmed these findings. Eibling et al 15 and Stachler et al 14 hypothesized that the change in subglottic airway resistance is responsible for the improved swallowing after TT removal. It was also reported that the fixation of the TT leads to decreased laryngeal mobility with a secondary inadequate opening of the upper esophageal sphincter. 1 , 2 The cuff pressure can reduce the esophageal passage and cause an overflow of saliva into the larynx and the trachea. 3
Some reports did not find any correlation between TT and swallowing/aspiration (e.g., Leder et al
8
-
11
). Nevertheless, the same group recommended fiberoptic
Influence of the TTs on the swallowing frequency (n = 20 patients, mean ± SD). Change of swallowing frequency after removing the TT and manually occluding the tracheostoma (n = 20, Wilcoxon test = 0.001).
TT, tracheotomy tube. Change of the swallowing frequency after removal of the tracheotomy tube. (n = 10 patients, follow-up 5 days).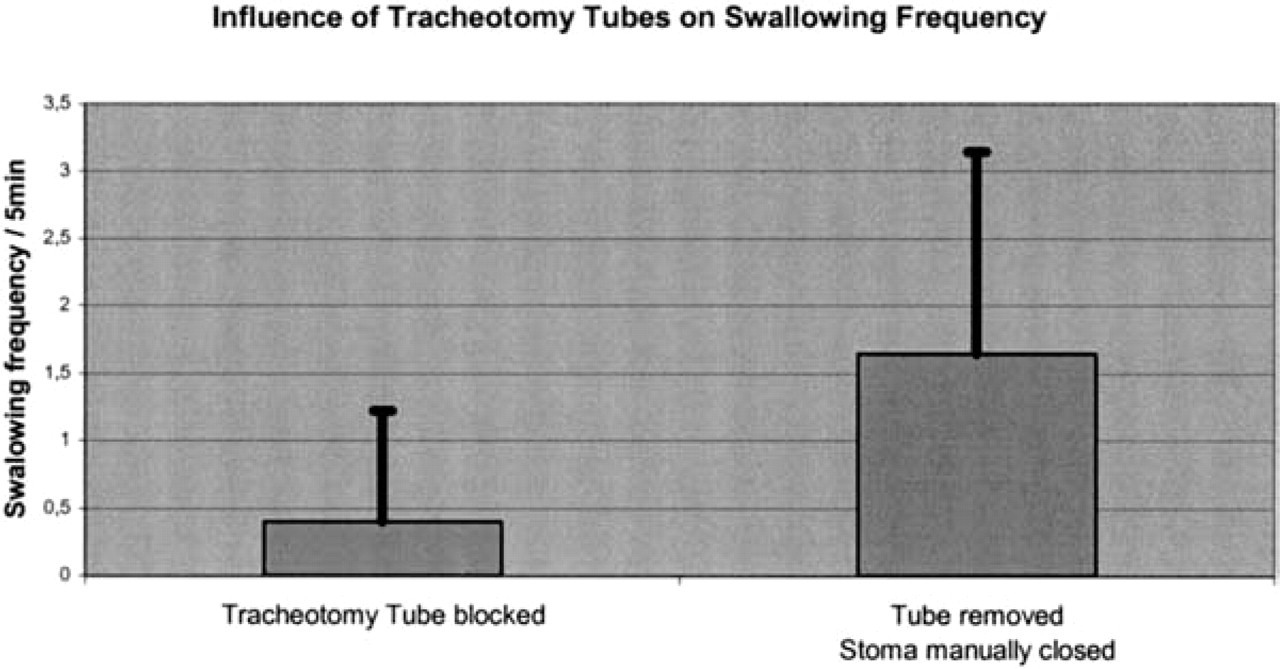
One of the main reasons for these conflicting results seems to be the inhomogenicity of the patient samples that were reported about. We therefore included in the present study patients with neurogenic dysphagia only. In this way, we can definitely exclude the influence of a mechanical obstruction within the pharynx as frequently found after tumor excision for cancer of the head and neck. Mechanical influences of TTs on the upper esophageal sphincter 3 or the pharyngeal mucosa 1 , 2 are usually minimized today. Technologically improved TTs and less invasive surgical strategies for tumor excision reduce those effects. 11
One major finding in our study is the effect that removing the TT and the occlusion of the stoma opening redirect the expiratory airflow through the lumen of the larynx with consequences for swallowing. We suggest that the redirection increases the perceptive sensitivity of the laryngotracheal mucosa as evidenced earlier. 4 - 6 This could be the initiating trigger for the patients to increase the SF. 7 Moreover, the glottic closure is reduced in time during swallowing. 6 The severity of the underlying neurogenic disorder was not correlated to the changes in SF. This provides additional evidence for the great impact of the redirection of airflow to increase the mucosal sensitivity and to stimulate an increase in SF. Further investigations with f-MRI are necessary to explain the phenomenon in full detail. However, our results cannot be compared to those of patients with cancer of the head and neck. 8 - 11 Swallowing in these patients is largely mechanically impaired by scars, the effects of irradiation and the tissue defects.
CONCLUSION
TTs decisively influence the swallowing behavior of vegetative patients with neurogenic dysphagia. This phenomenon could be based on an improved perceptive sensitivity of the pharyngolaryngeal mucosa after renewed physiological expiration following the removal of the TT. We strongly favor to removing or deflating the cuff of the TT under therapeutic conditions in the rehabilitation of vegetative neurogenic patients.