
Abstract

Introduction
The brachiocephalic trunk is the largest branch of the arch of aorta. Normally, this artery is 4–5 cm long, arising from the aortic arch convexity in midline, ascending posterolaterally to the right, at first anterior to the trachea, then on its right, and dividing into the right common carotid artery and right subclavian artery posterior to the right sternoclavicular joint. 1
The brachiocephalic trunk can be abnormally long reaching up to the level of trachea. In about 12% of cases, the right common carotid artery arises above the level of the sternoclavicular joint. 2 When the brachiocephalic trunk divides higher, it may incline to the left rising in front of the trachea above the sternum, and therefore complicates tracheotomy. 3
We describe a patient with the brachiocephalic trunk ascending to an abnormally high level of the second tracheal ring.
Case Report
A 62-year-old woman was hospitalized for adenoma of the right inferior parathyroid gland with consequential hyperparathyroidism and hypercalcemia. On ultrasonography of the front of the neck, the right thyroid lobe was inhomogeneous and isoechogenic, measuring 40 × 13 × 16 mm (length × width × thickness). A markedly hypoechogenic node of 22 × 9 × 12 mm was observed behind the lower pole of the right lobe. The left lobe, also of inhomogeneous structure, measured 43 × 13 × 14 mm.
The level of parathyroid hormone (PTH) was 130.0 (reference range 10–65) pg/mL in peripheral blood, and 2,300 pg/mL in the node biopsy specimen. Serum calcium concentration was 3.26 (reference range 2.3–2.8) mmol/L. The finding obtained by the aspiration biopsy cytology of the node was consistent with the picture of parathyroid adenoma.
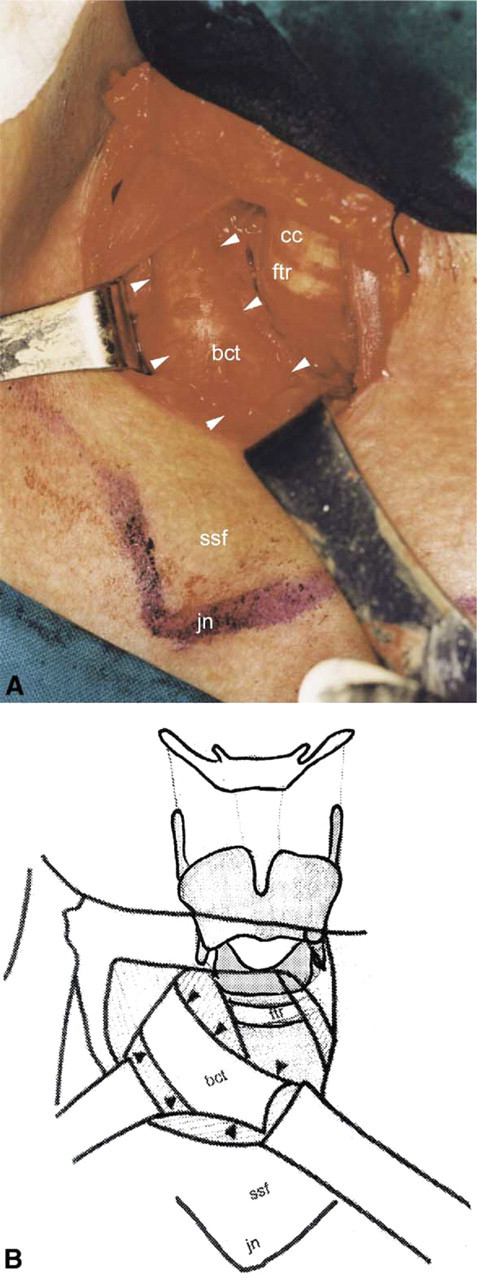
On the operating field preparation, pulsations in the region of suprasternal fossa synchronous with cardiac action were observed, suggesting flow abnormality in one of the large blood vessels of the neck and superior mediastinum. A horizontal incision was made through the skin and subcutaneous tissue above the site of pulsation and 3 cm above the suprasternal fossa. Pretracheal muscles were bluntly dissected and moved apart along the midline to expose the right lobe of the thyroid gland. The abnormally highly located brachiocephalic trunk of 8 mm in diameter was found prominating in front of trachea. The concave segment of the arch reached the first tracheal ring (Fig 1). The trunk was lateralized by a blunt hook, to allow for extirpation of the inferior parathyroid gland adenoma.
The postoperative course was normal. Serum calcium concentrations decreased to 2.35 mmol/L on postoperative day 2. The patient was discharged on day 8 postoperatively.
(
Discussion
Although hospitalized for quite a different reason, our patient with the brachiocephalic trunk overlying the second to fifth tracheal rings, adjacently to the lower edge of the cricoid cartilage, is presented to illustrate the possible hazard of fatal complications that may occur on operative procedures in the anterior and lateral regions of the neck, with special reference to tracheotomy.
Tracheotomy is the most important and most successful procedure in the operative prevention of respiratory insufficiency, which should be performed without delay when the disease or injury is suspected to cause breathing difficulties. In this way, the number of emergency tracheotomies is decreased, and untroubled and composed work in the operating theater (classic tracheotomy) is ensured, thus reducing the rate of complications related to the procedure. Bleeding is one of the most common complications, which may occur intra- or postoperatively due to vascular wall erosion with inappropriately placed metal cannula.
Tracheostoma is usually done between the second and fourth tracheal rings, as this position does not interfere with the surrounding structures, primarily blood vessels. On tracheotomy, caution must be exercised for a number of structures that may bleed during the procedure. Most important of these are brachiocephalic trunk (innominate artery), anonymous vein, and inferior thyroid plexus.
Innominate artery runs over the trachea already in the region of thoracic cavity, however, cases of innominate artery of normal width reaching the region of suprasternal fossa are not rare, and depend on the individual's neck length and on the state of inspiration/expiration. Therefore, we emphasize the importance of upward tracheal opening.
Krmpotic describes a case where the innominate artery was positioned at only about 2 cm below the lower edge of the thyroid gland. In such cases, there is not only the risk of intraoperative arterial injury but also of the arterial wall erosion during prolonged cannula insertion. 3 In our patient, the high position of the brachiocephalic trunk, with the concave segment of its arch reaching to the first tracheal ring, posed a great risk on tracheotomy, as it may lead to arterial lesion and lethal outcome due to massive bleeding. 4
This and other similar abnormalities of the aortic arch vessels are usually manifested by respiratory symptoms from early childhood (irritation cough, shortness of breath on exertion, hoarseness), which were not present in our patient. 5 Therefore, there were no history data pointing to this potential risk. Preoperative clinical examination failed to reveal any innominate artery pulsations, as it was performed in sitting position. It was only in supine position with hyperextension of the neck that pulsations of the anterior region of the neck warned us of the potential risk of abnormalities of the large blood vessels of the neck and superior mediastinum.
Therefore, even in case of emergency tracheotomy or any other operative procedure of the anterior region of the neck, the possible abnormalities of the large blood vessels of the aortic arch and their collision with the operating field should always be considered in order to prevent the life-threatening complications of massive bleeding.