
Abstract

CASE REPORT
A 20-year-old woman with no significant medical history presented with a severe sore throat, dysphagia, and odynophagia. She denied any respiratory distress or dysphonia. In addition, there was no recent history of foreign body ingestion, violent coughing, retching, substance abuse, or dental procedures.
Vital signs on presentation were normal with no evidence of fever. Physical findings were remarkable for neck crepitance with exquisite tenderness on palpation. The rest of the head and neck examination was within normal limits. Fiberoptic laryngoscopy revealed a patent supraglottic and glottic airway with normal vocal fold movement.
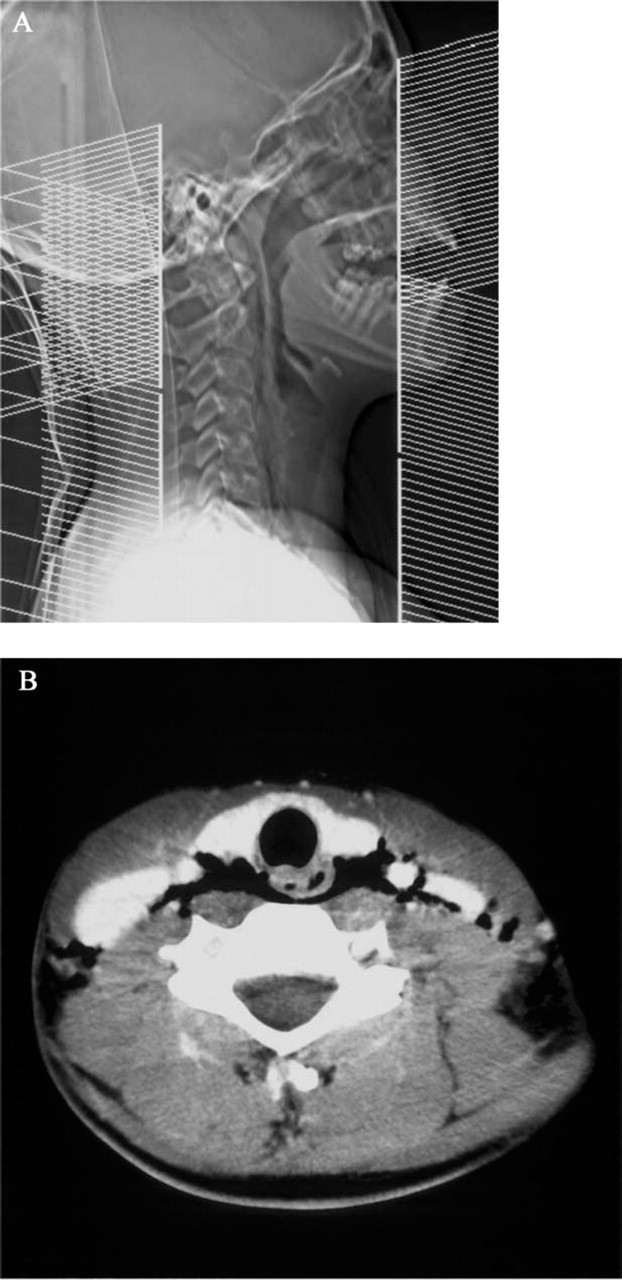
Chest roentgenogram showed air lucency in the retropharyngeal soft tissue with no associated pneumothorax. Computed tomography of the neck confirmed extensive cervical emphysema involving preferentially the retropharyngeal space with no evidence of fluid collection or foreign body (Fig 1).
The patient was diagnosed with SRE and admitted to the hospital for observation. She was placed on nothing by mouth and intravenous hydration. Her symptoms gradually resolved with no further investigative studies. She was discharged on the third hospital day with a regular diet.
DISCUSSION
The anatomy of the cervical spaces was described by Grodinsky and Holyoke. 1 Only relevant features of the deep cervical fasciae and fascial spaces are presented here (Fig 2. The retropharyngeal space is located between the middle and deep layers of the deep cervical fascia. It extends from the skull base to a level varying between the sixth cervical and the fourth thoracic vertebrae, where the alar and the visceral divisions fuse. Posteriorly the alar division separates the retropharyngeal space from the danger space, which is in turn separated from the prevertebral space by the prevertebral fascia. Laterally the retropharyngeal space is in continuity with the parapharyngeal space. Understanding the retropharyngeal space and surrounding fascial compartments has important clinical implication, for deep neck infection involving this space may spread to the mediastinum with significant morbidity and mortality.
Patients with SRE usually present with sore throat, dysphagia, and generalized neck pain. Physical findings include crepitance in the neck, chest, and facial areas. Roentgenograms reveal air streaks within cervical tissue and free air in the retropharyngeal region. When the mediastinum is involved, symptoms also include dysphonia and retrosternal pain radiating to the back. Classic signs of pneumomediastinum include mediastinal crunch (Hamman's sign) and decreased cardiac dullness. Our patient presented with typical features of retropharyngeal emphysema. Given the rapidity of symptom development and substantial cervical emphysema with little mediastinal involvement, the patient likely had SRE with early stage of dissection into the mediastinum.
(
The differential diagnosis of retropharyngeal emphysema is extensive. Traumatic injuries such as intubation, foreign body impaction, esophageal instrumentation, dental procedures, and Boerhaave's syndrome can lead to retropharyngeal emphysema. Deep neck infection with gasforming agents can also cause emphysematous changes in the retropharyngeal space. Pediatric patients are especially at risk because of a higher incidence of retropharyngeal lymph node suppuration from upper respiratory infection. In addition, substance abuse is a recognized cause of retropharyngeal emphysema. Marihuana, cocaine, heroin, and amphetamine have been implicated where sustained Valsalva maneuvers may result in intra-alveolar hyperpressure with subsequent pneumomediastinum and retropharyngeal emphysema. 2
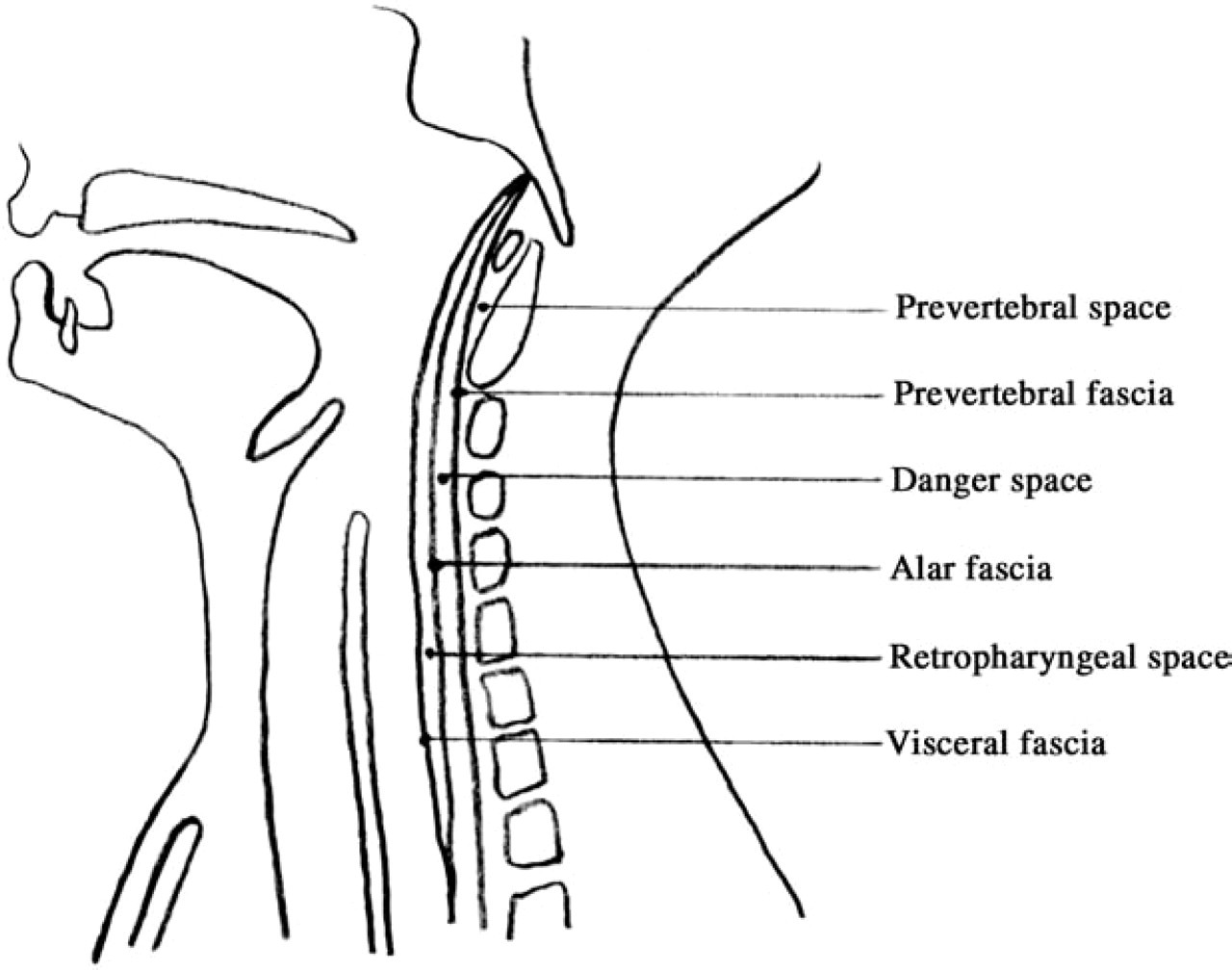
Midsagittal section of the neck demonstrates the retropharyngeal space and its relationship with surrounding fasciae and fascial spaces.
SRE is a diagnosis of exclusion. The more serious disorders discussed here should be ruled out during the evaluation. Historical information may indicate the presence of trauma to upper aerodigestive tract from foreign body impaction or medical and dental instrumentation. Any increase in intrathoracic pressure related to coughing, pulmonary barotrauma, or Valsalva maneuver should be elicited. Clinical signs may reveal fever or leukocytosis, suggesting an infectious process in the retropharyngeal region. When pharyngoesophageal perforation is suspected, contrast studies or endoscopy or both are indicated. In one report, gastrograffin contrast study had a sensitivity of 50% in detecting esophageal perforation. Yet it was the preferred initial tool of investigation because of minimal damage to mediastinum in the presence of a perforation. A barium swallow study would improve the diagnostic yield and was recommended after a negative gastrograffin study. Esophagoscopy alone was not a definitive test in that it only detected 30% of subsequently proven esophageal perforations. Pollack et al 3 suggested esophagoscopy after a negative gastrograffin study but before a barium swallow since the latter may lead to long-term complications such as mediastinum fibrosis. When all these causes are excluded as in the case presented, a diagnosis of SRE is reached. Because the suspicion of esophageal perforation was low in our patient, no contrast study or endoscopy was performed.
SRE is usually a benign process and carries a good prognosis. The self-limited nature allows a conservative therapy and an uneventful recovery. When there is significant mediastinum involvement, however, severe complication such as respiratory distress with decreased venous return and cardiac output may occur. 4 Hence, hospital admission with close observation is essential. Patients should be placed on intravenous fluid support and nothing by mouth until perforation of the upper aerodigestive tract is ruled out. Prophylactic antibiotics are not necessary unless evidence of infection is present. Surgical intervention is indicated only when there is progressive airway compromise from retropharyngeal emphysema despite the proper medical treatment. 5 Throughout the hospital course, our patient's airway remained stable. There was no evidence of pharyngoesophageal perforation. She tolerated oral intake with dramatic improvement of symptoms before she was discharged on the third hospital day.
In conclusion, SRE is only diagnosed after other more serious causes for retropharyngeal emphysema are excluded. A detailed history and physical examination are of paramount importance in narrowing the differential diagnosis. When perforation is suspected, further investigation such as swallow studies are indicated. Most patients with SRE recover well with conservative therapy.