
Abstract

Parotid edema has not been associated with ACE-I use. Unilateral parotid swelling is more common than bilateral, and its pathogenesis is likely multi-factorial. The primary pathogenesis is a decrease in parotid salivary volume and flow rate. Causes of reduced flow include stones, strictures, external duct pressure, mucus plugging, and congenital abnormalities. Nonobstructive factors include radiation damage and immune mediated diseases. The decrease in salivary flow results in stasis, which can lead to retrograde bacterial contamination of the ductal system. A common consequence of this contamination is opportunistic infection followed by chronic sialadenitis that presents as recurrent painful swellings of the gland. Sialolithiasis is both a cause and consequence of chronic recurring sialadenitis. The present case describes an adult female with recurrent, painless, and unilateral parotid gland swelling initially thought to be recurrent sialadenitis, but resolved after discontinuation of an ACE-I.
CASE REPORT
A healthy 49-year-old white woman first noted swelling in the area of her right parotid 4 months before presentation in our clinic. The parotid swelling was painless and initially thought to be related to a concurrent upper respiratory infection. Her medical history was only significant for hypertension, which was well controlled with a diuretic (hydrochlorothiazide 12.5 mg/day) and an ACE-I (ramipril 5 mg/day). She was seen by her local physician, who placed her on a 2-week course of amoxicillin. The swelling initially responded to this treatment, but rapidly recurred. Her recurrent edema, again localized to the right parotid, was then treated with ciprofloxacin and a decongestant. The swelling resolved completely but again recurred after finishing the antibiotics, at which time she presented to an acute care facility. The patient was treated with another antibiotic and instructed to use sialogogues and warm compresses for the presumed diagnosis of recurrent sialadenitis.
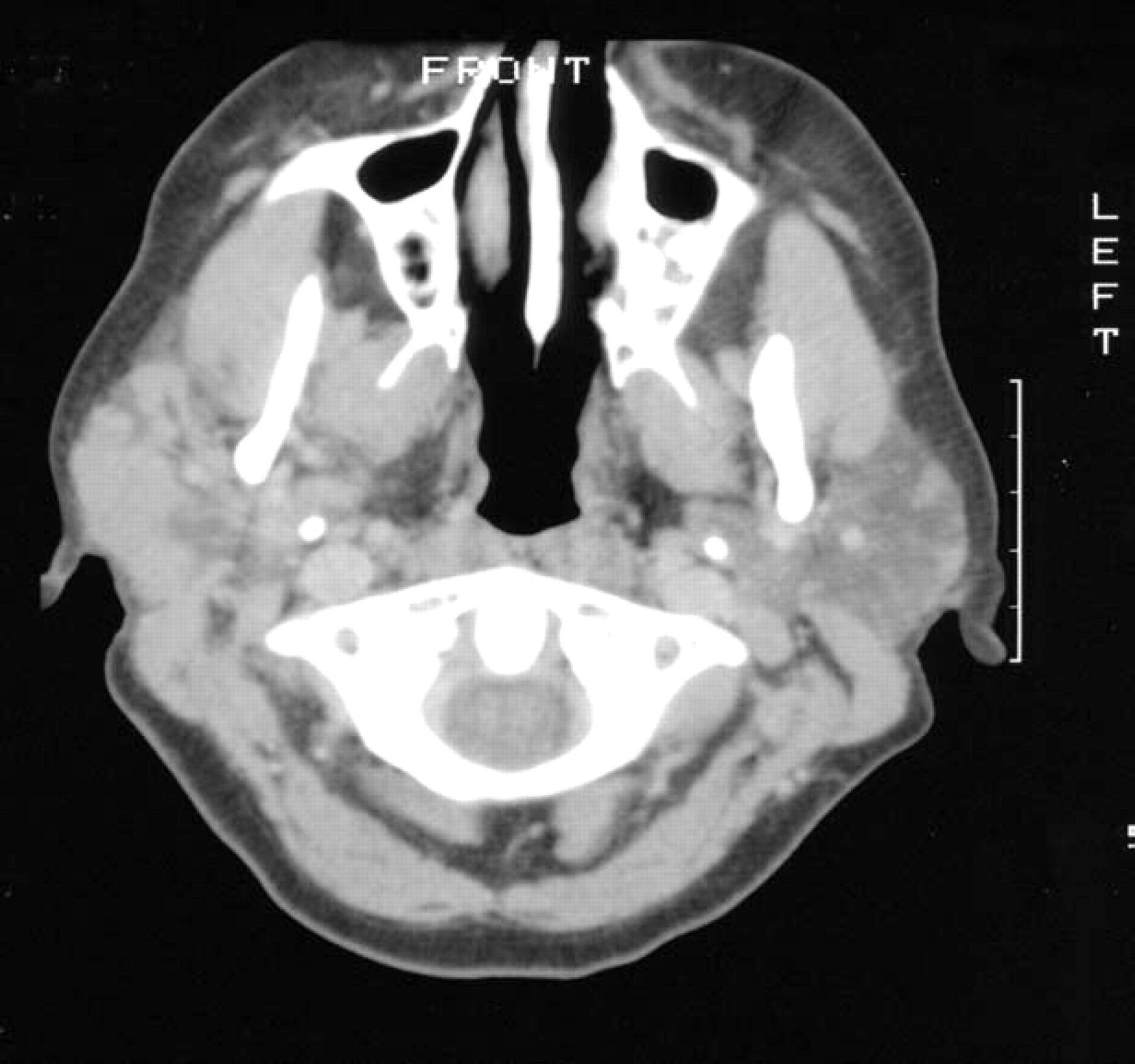
Initial CT scan shows parotid gland swelling
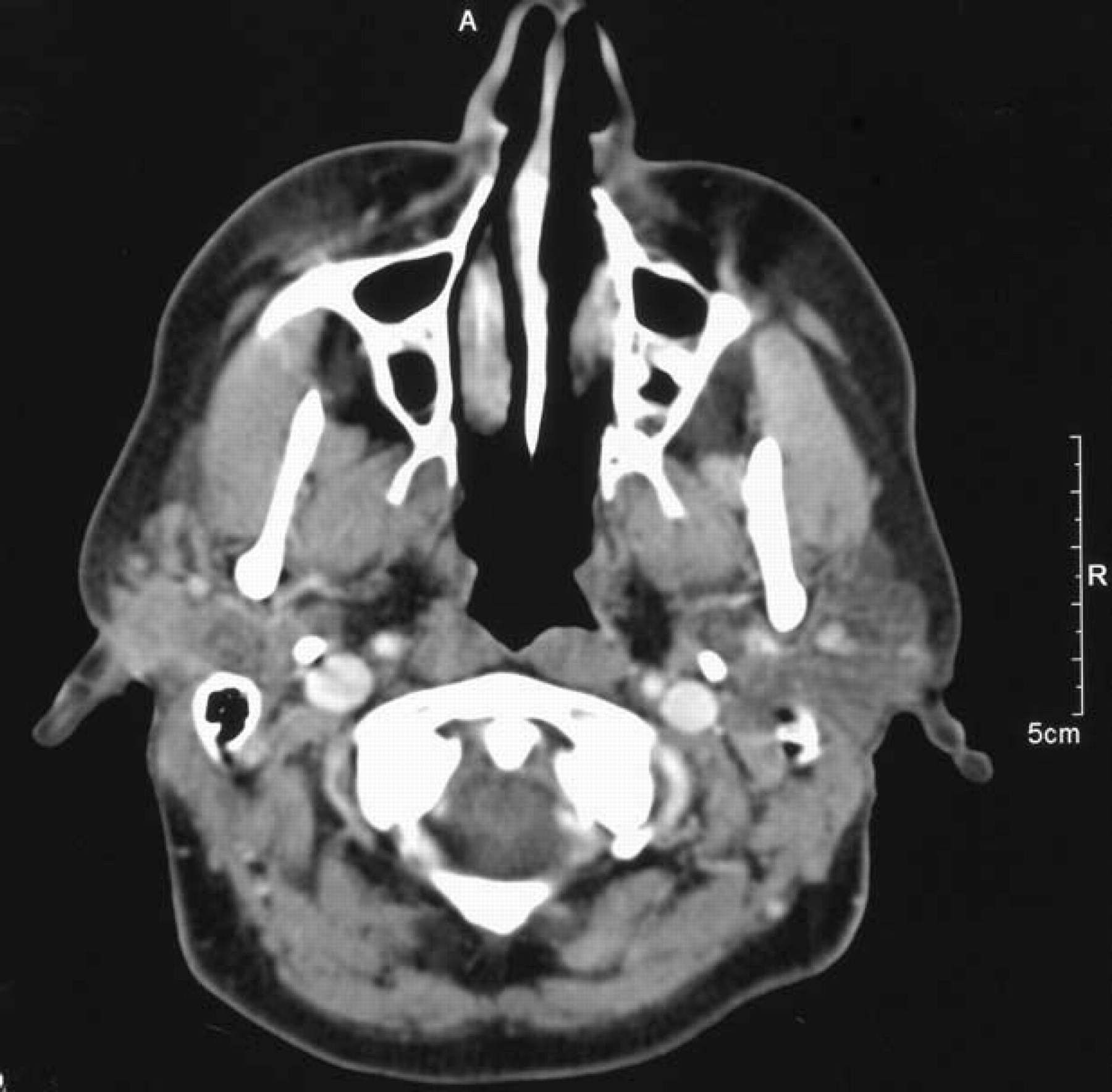
CT scan 6 weeks later with resolution of parotid gland swelling
The swelling again resolved, but quickly recurred, and she was referred to a local otolaryngologist. A computed tomography (CT) scan showed a nonspecific mass overlying the right parotid (Fig 1) and a fine needle aspiration of the area revealed benign-appearing lymphocytes and parotid cells with no evidence of malignancy. With the diagnosis of chronic parotitis, she was sent home on Augmentin and scheduled for a superficial parotidectomy. However, the swelling again resolved completely and surgery was delayed. A CT performed 5 weeks later showed the right parotid gland was significantly smaller than the prior CT and there seemed to be greater enhancement in the lateral aspect of the gland, but no discrete mass (Fig 2). Within a month, the swelling recurred on the right side, as in previous episodes.
At this time, the patient was referred to our tertiary care facility for further evaluation and treatment. She reported recent swelling of her right parotid area, and for the first time, she had night sweats and chills but no weight loss. She reported some increased salivation with no history of xerostomia or autoimmune disease. She denied hemoptysis, hematemesis, dysphagia, odynophagia, weight loss, dyspnea, fevers, or voice changes and generally felt well. Physical examination, including nasopharyngoscopy, revealed no abnormalities and she had no palpable parotid masses, edema, or tenderness. Normal-appearing saliva could be expressed from Stensen's duct. She was sent home with a prescription for Augmentin and told to begin a 7-day course at the first sign of parotid swelling. During the next month, she experienced 2 episodes of parotid swelling that resolved within a few days of starting treatment. Clindamycin was later added to the Augmentin, but this did not change the course or presentation of her recurrent episodes. Although usually confined to the preauricular region, 1 episode of right face swelling continued anteriorly until her nasal-labial crease was expunged. By the next morning, the swelling had completely resolved with no airway involvement or complications.
As her episodes of parotid swelling were transient with no evidence of infection or long-term response to therapy, we considered her angioedema could be secondary to ACE-I use. Her hypertensive regimen was changed to exclude ACE inhibitors, and 4 weeks later she returned to clinic with no further episodes of parotid swelling. She has not had any parotid swelling for more than 8 months after ACE-I discontinuation.
DISCUSSION
ACE inhibitors are used to treat hypertension and congestive heart failure. They are frequently given to patients with diabetes, particularly in the presence of microalbuminuria, as they can delay progression to end stage renal disease. As a group, ACE inhibitors have relatively few side effects. Adverse effects include dizziness (4%), dry cough (up to 10%), headache (2.5%), and hypotension. Angioedema is an uncommon but potentially life-threatening side effect associated with all ACE inhibitors and may occur soon after the onset of treatment or be delayed for years. Angioedema has also been associated with the use of angiotensin II receptor blockers, often in patients who have had ACE-I-induced angioedema. 5 ACE-I-associated angioedema is responsible for a significant portion of angioedema presentations, and patients should be warned that angioedema may recur with repeated use of these 2 classes of drugs.
Although our patient was Caucasian, ACE-I-induced angioedema is more common in African Americans, and all 7 deaths reported in a series from Ohio were African American. 2
Unilateral parotid swelling is typically a manifestation of duct blockage from salivary calculus, tumor infiltration, autoimmune disease, or infectious causes. Until now, isolated parotid swelling has not been associated with ACE-I-induced angioedema. However, these drugs are widely used and may be a relatively common but unrecognized cause of paroxysmal parotid edema. Although our patient did not have significant progressive edema or evidence of airway obstruction, patients with ACE-I-induced angioedema can have escalating episodes if the underlying agent is not discontinued. Drug-induced angioedema should be considered in cases of recurrent parotid swelling without other obvious causes.