
Abstract
There are a number of techniques described that use autologous cartilaginous grafts, whether simple or composite, to reconstruct segments of the laryngotracheal wall. Grafts free of nasal or auricular cartilage with or without perichondrium or mucoperichondrium have been used frequently as anterior and posterior separators, but are used less often when it is necessary to cover large defects or surgical wounds. Although it is possible to revascularize and to re-epithelialize these inserts starting from around the margins, the consensus is that the recipient area must not exceed 1 to 1.5 cm.1 The tracheal wall, covered with respiratory mucosa with circular structure and semirigid cartilaginous support, appears to be the ideal donor tissue for extensive laryngeal defect reconstruction. However, the use of isolated segments of trachea presents problems of revascularization since the small tracheal vessels are not adequate for microvascular anastomoses2 nor is it possible to induce neovascularization starting with material from the neighboring tissue of the neck that is relatively poorly vascularized.3 To overcome this limitation, several methods have been developed for tracheal revascularization not only in animals but also in human beings that make it feasible to use auto- or allo-grafts. Good results have been obtained covering tracheal segments with well-vascularized flaps that provide external neovascularization. Omental flaps have been used in animals to cover isolated portions and devascularized thoracic trachea either separated completely and newly reanastomosed in situ or allo-grafted to another recipient animal. Although some results have been negative,4,5 Fujiwara et al6 demonstrated that the covering with epiploon improved the scarring at the anastomosed site because of the rapid re-establishment of tissue blood flow.
Delaere et al7 developed a new technique of auto-transplant in rabbits and also achieved good results in cancer patients.8 The first 2 cm of the cervical trachea of the rabbit was isolated from the paratracheal tissues and the lateral thoracic fascial flap was used to wrap the isolated trachea. In a subsequent surgical intervention, the tracheal segment was sectioned and transformed into a newly vascularized patch capable of being used to reconstruct the surgical defect of the extended hemilaryngectomy. In human beings, 4 cm of the cervical trachea can be separated from the esophagus and from the thyroid gland and wrapped by a radial free fascial flap microanastomosed to the superior thyroid pedicle. At 2 weeks, this segment is separated from the trachea and fixed like a vascularized patch in reconstructing the extended hemilaryngectomy and that includes the extirpation of the thyroid wing and the hemicricoids. Subsequently, laryngotrachea continuity is re-established with an anastomosis between the distal trachea and the reconstructed cricoids. The microsurgery techniques of Delaere et al7 made the method of reconstruction of extended hemilaryngectomy feasible and included the resection of the hemicricoids.
Another method described for partial replacement of the laryngeal wall consists in elevating the proximal trachea to make a trachea-thyroid anastomosis. In this way, a reconstructed cricoid ring is achieved in cases of subglottal stenosis. Pearson et al9 and Grillo et al10 performed primary tracheathyroid anastomosis after complete resection of the cricoid ring and part of the posterior cricoid plate. The cricoid was satisfactorily replaced with the circular cartilaginous trachea. The length of the resection was up to 6.5 cm with maneuvering to achieve supraglottis release. Grillo et al11 described a more extended resection of the larynx in cases that had lateral tumors of the trachea, including extensions beyond the cricoids. In this case, the distal trachea was designed to substitute for the lateral wall of the trachea thus conserving the structure and the stability of the extirpated area that had included the cricoid cartilage and the larynx wall below the level of the vocal cords.
From the anatomic studies of Salassa et al2 it has become accepted that the trachea receives its principal blood supply from the inferior thyroid artery. The supply that is distributed by the superior thyroid pedicle to the trachea across from the thyroid gland could be sufficient to guarantee vascularization of the tracheal segment without recourse to vascularized flap covers. Ganon et al12 isolated long tracheal segments in dogs while maintaining only the relationship with the thyroid gland and the superior thyroid pedicles. The tracheal segments were then re-implanted to achieve a normal circulation. Similarly, Gender et al13 used vascular microanastomoses from the superior thyroid pedicle, autotransplanted tracheal segments isolated 2 hours previously, and achieved revascularization.
These studies suggest that the proximal trachea can be used to cover wounds resulting from extended laryngectomy. To evaluate this possibility, we developed an animal model in rabbits. We extirpated half of the anatomic structure of the larynx (including the hemicricoids) and reconstructed the surgical defect by elevating the proximal trachea into the required position.
Material and Methods
Ten New Zealand white rabbits weighing between 2.25 and 2.8 kg were medicated with xylocaine hydro-chloride (intramuscular; 6 mg/kg) and ketamine hydro-chloride (30 mg/kg via an indwelling venous catheter in the ear). Halothane-oxygen was used as anesthetic via an inhalation facemask and spontaneous breathing was maintained throughout the procedure. Prophylactic antibiotics (ceftriaxone 40 mg/kg) were administered. The skin anterior to the neck was shaved and prepared with a betadine solution. The animal was placed in the supine position with the neck hyperextended using a support under the shoulders. A medial cervical incision was made extending between the hyoids and the supra-sternal notch. The pre-laryngeal muscles were separated along the median line exposing the larynx, the trachea, and both lobes of the thyroid gland. On the side of the hemilaryngectomy, the medial thyroid vascular pedicle was located and freed from the neighboring areolar tissue of the thyroid gland up to its origin in the common carotid and the internal jugular. This maneuver proposes to avoid tension of the vascular pedicle so as to mobilize the thyroid gland and the trachea. The inferior thyroid pedicle is not manipulated. The thyroid lobe on the hemilaryngectomy side is maintained intact above the trachea but separated from the adjacent cricoids. The end of the inferior laryngeal artery and the branches to the sternocleidomastoid muscle arising from the medial thyroid artery are ligated and sectioned. The thyroid isthmus is sectioned in the medial line. On the contralateral side, the thyroid lobule is separated from the trachea but its relationship to the cricoid cartilage is retained intact. The thyroid vascular pedicles are not manipulated. The recurrent laryngeal nerve extending from this side is conserved.
Subsequently, the trachea is sectioned between the cricoids and the first ring and separated completely from the larynx. An indwelling endotracheal tube is put in place to maintain the anesthesia. The first 2 cm of the trachea are freed from the esophagus leaving the pedicle to the thyroid lobe conserved, as are the medial thyroid vessels. The extended hemilaryngectomy is commenced with an anterior laryngeal slit across the thyroid cartilage and cricoids, conserving 2 to 3 mm of the upper border and another 2 to 3 mm of the upper third of the posterior border (Fig 1). The edges are separated to expose the endolarynx. The mucosa and the posterior cricoid lamina are sectioned along the medial line so as to preserve the esophageal mucosa intact. The incision in the mucosa is extended laterally over the arytenoids and the proximal aryepiglottal fold while conserving the upper mucosal surface of the arytenoids to facilitate the subsequent reconstruction. The constrictor muscles are sectioned on the posterior border of the thyroid wing and the mucosa of the piriform sinus freed from the internal surface. The posterior surface of the cricoid lamina is separated from the esophagus. The hemilarynx, united only to the aryepiglottal fold, is separated at this level, and the thyroid wing and the hemicricoid are extirpated.
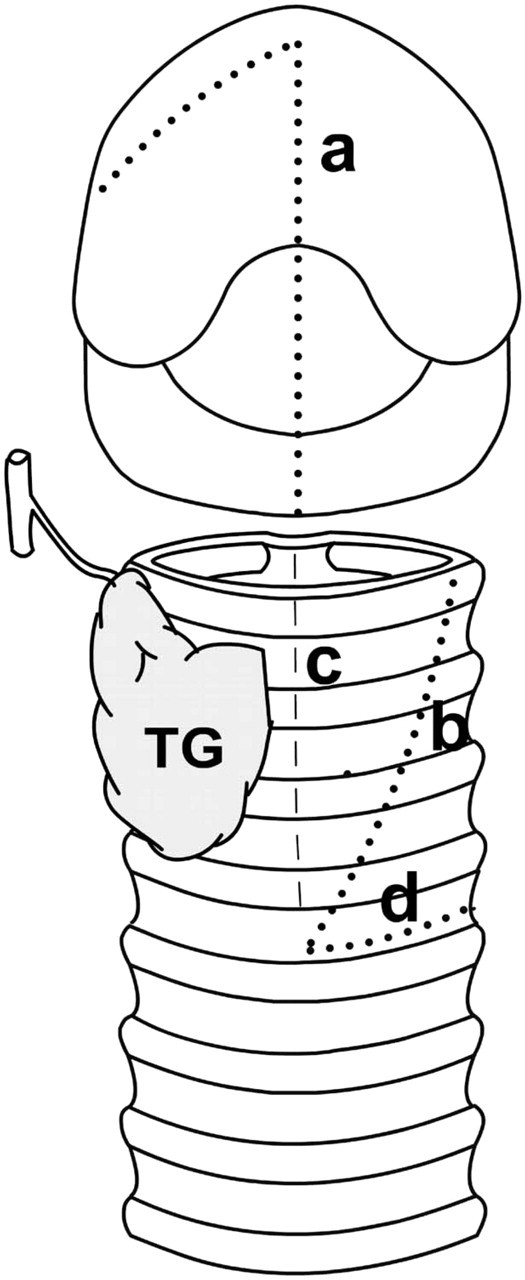
Incision schemes. The larynx and the trachea have been separated at the level of the cricothyroid membrane (a, anterior median incision along the thyroid and cricoid cartilages conserving the upper border of the thyroid cartilage; b, dotted line along the trajectory of the vertical-oblique incision on the anterior face of the trachea; c, discontinuous line projecting along the incision posterior to the trachea at the level of the pars membranosa; d, dotted line along the horizontal section between 2 tracheal rings that join the anterior and posterior incisions (b and c); TG, thyroid gland conserved on the tracheal flap).
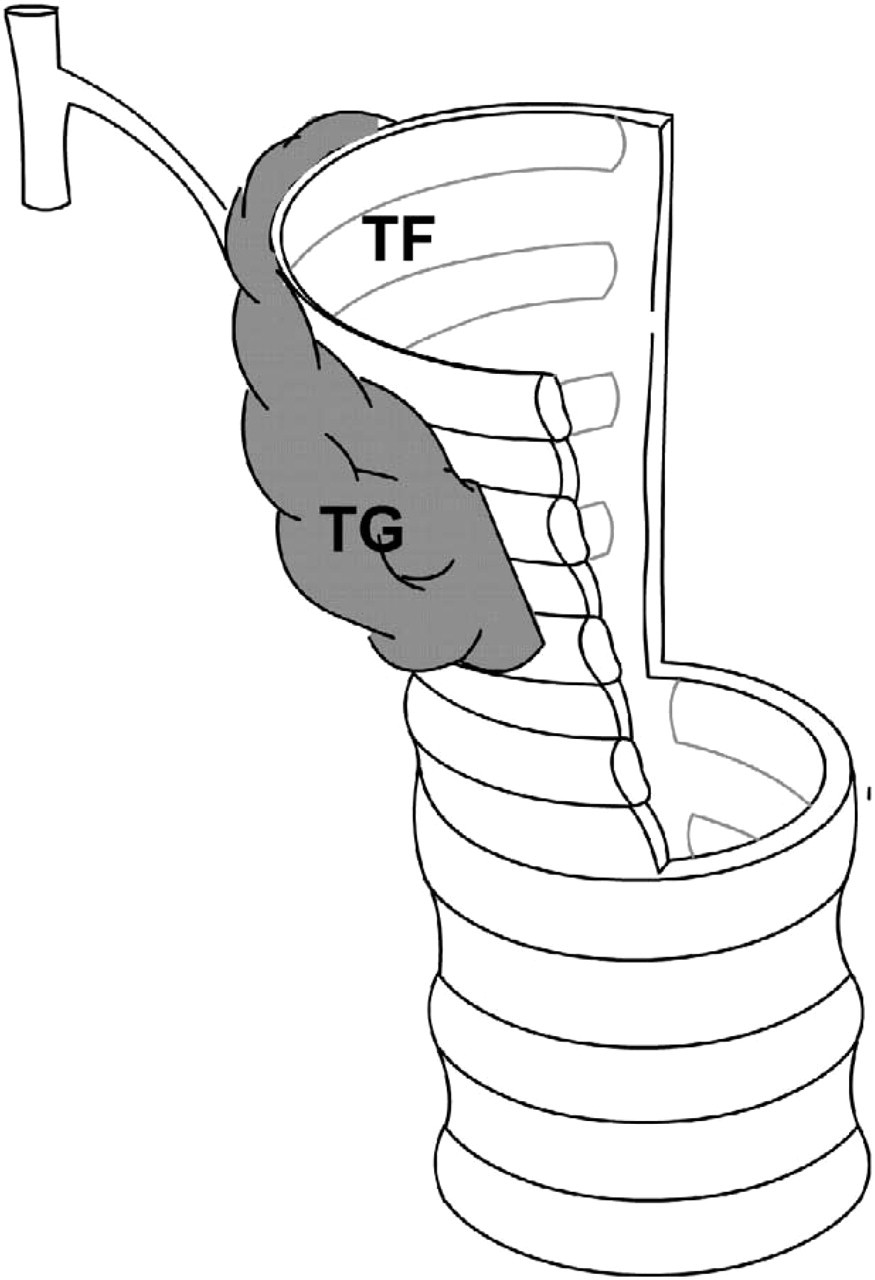
Design of the tracheal flan (TF, tracheal flap; TG, thyroid gland preserving the vascular pedicle).
The next stage is to shape the tracheal flap for the reconstruction of the hemilaryngectomy wound so that it is wider at the cranial than the cricoid level. The trachea is sectioned longitudinally at the level of the pars membranosa for a length of 15 mm. This incision is continued with another transversal incision between 2 tracheal rings from the pars membranosa to the anteriomedial line. From this point, a third vertical-oblique incision is extended up to the cephalic border of the lateral face (Fig 1). In this manner, a trapezoidal tracheal flap is created attached to the trachea at its distal extreme and with the lobe of the thyroid gland attached to the external surface (Fig 2). The reconstruction commences with suturing the posterior border of the tracheal flap at the level of the membranous pars to the posterior surgical border of the conserved cricoid lamina using 4 separate stitches (Prolene 5.0 Ethicon). The mucosa conserved from the arytenoids and the piriform sinus is sutured to the border over the posterior upper cartilage ring of the tracheal flap. The remaining upper border of the flap is sutured to the upper border saved from the thyroid wing and to the aryepiglottal fold. The opening of the piriform sinus is checked with endoscopy. The laryngotracheal contiguity is restored by suturing the distal tracheal ring to the lower border of the conserved contralateral cricoids. Finally, the larynx is closed completely by suturing the anterior borders of the tracheal flap and the conserved thyroid cartilage (Figs 3 and 4). The sutures pass through the full thickness of the laryngeal wall and include cartilaginous tissue whenever possible. All the stitches are tied externally. Small breaches of the mucosa are closed with extra stitches to preclude cervical emphysema formation. An endoscopic examination is performed to confirm that the glottal and subglottal space is maintained. The surgical wound is washed with betadine solution and physiologic saline solution. The prelaryngeal muscles are not sutured, and the incisions in the skin are closed with staples. A single, postoperative dose of 6-metylprednisone (2 mg/kg) is administered. Food and water are withheld for the initial postoperative 24-hour period but allowed ad libitum subsequently. Ceftriaxone (intramuscularly; 40 mg/kg) is administered as a single daily dose for 5 days.
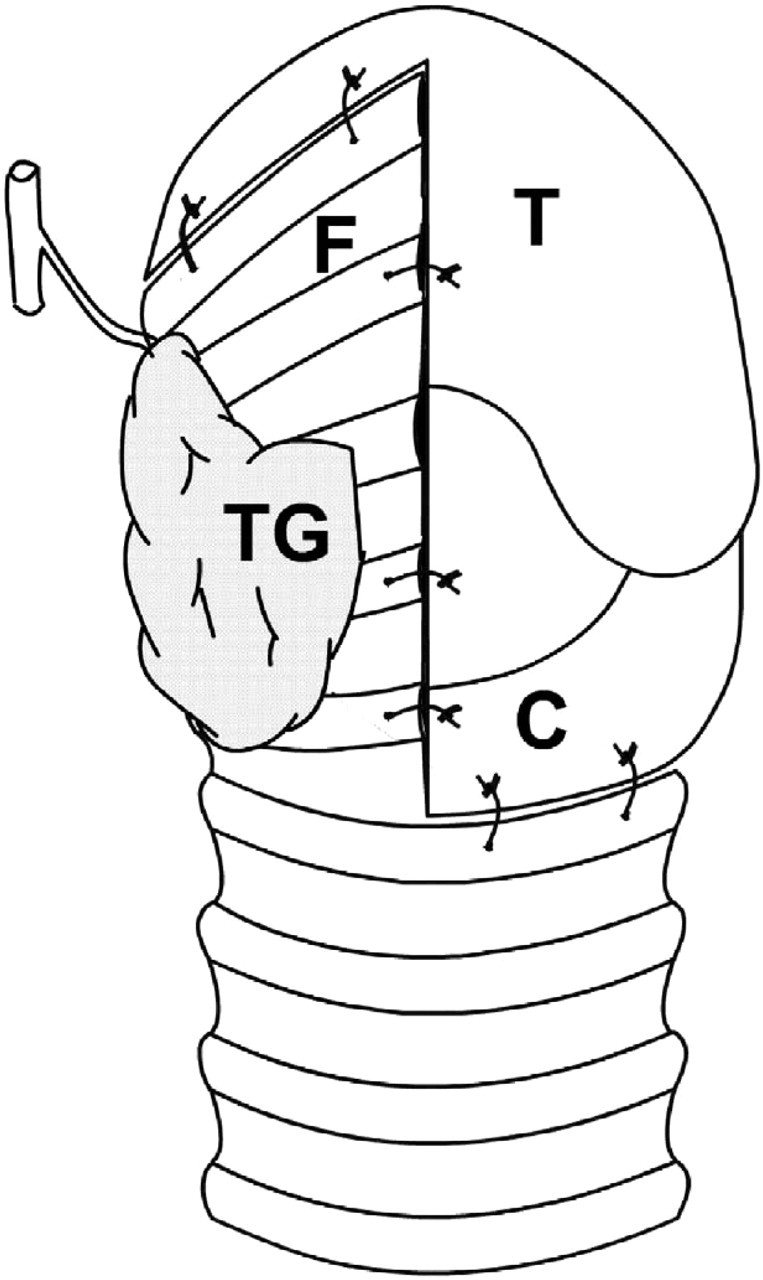
Frontal view of the tracheal flap sutured to the surgical wound of the hemilaryngectomy (T, thyroid cartilage; C, cricoid cartilage; F, tracheal flap; TG, thyroid gland).
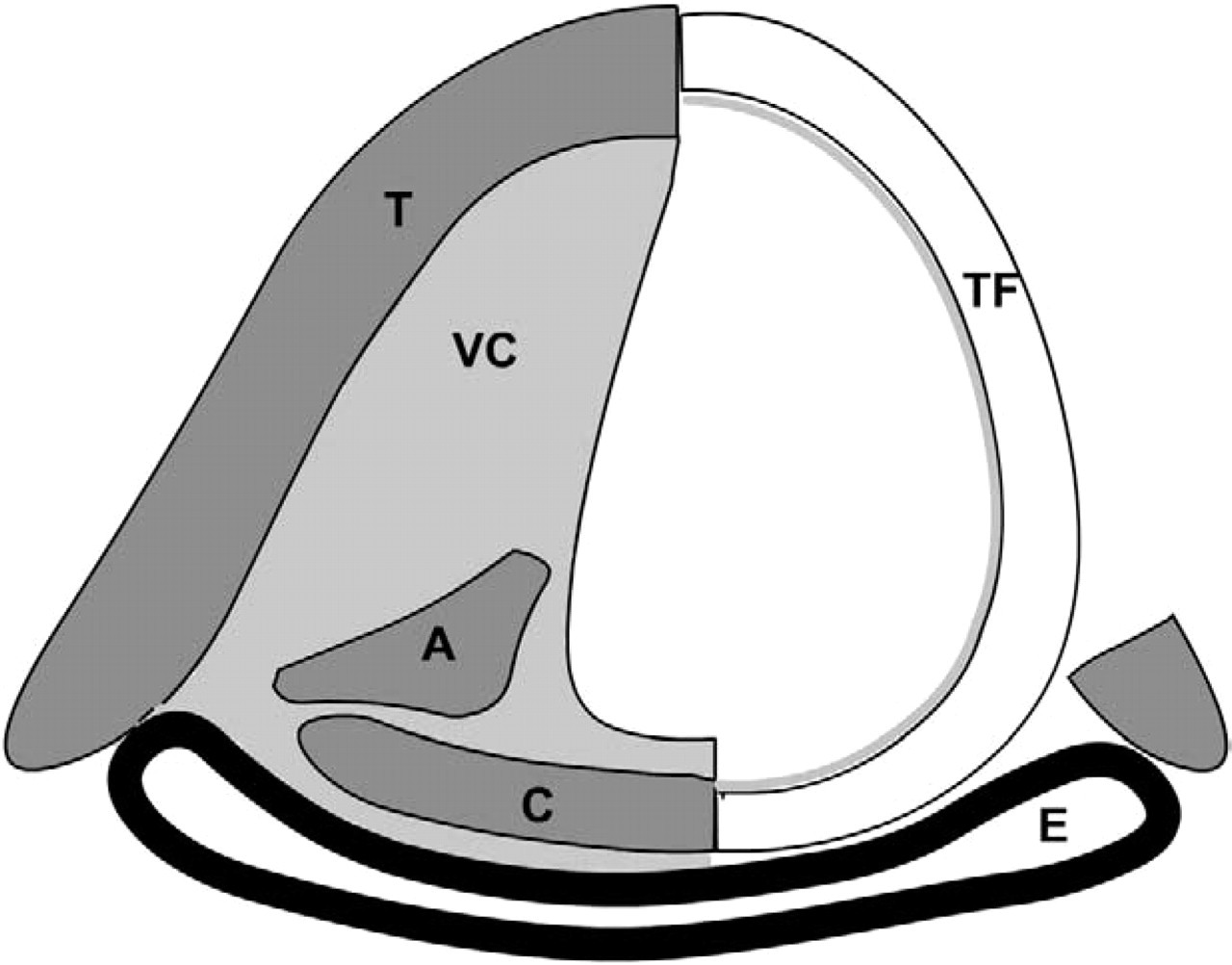
Diagram of the cut at the level of the glottis (T, preserved thyroid cartilage; A, preserved arytenoid; TF, tracheal flap covering the hemilaryngeal wound; P, posterior border of the resected thyroid lamina; VC, vocal cord; E, esophagus).
The animals were monitored for 4 weeks, after which they were sedated with a combination of ketamine and xylocaine. A laryngotracheal endoscopy was performed to evaluate the wall of the reconstructed larynx and to observe any laryngeal stenoses. The animals were then sacrificed with an overdose of sodium pentobarbital; the laryngotracheal specimen was removed and placed in 10% formalin and prepared for histologic examination. Transverse sections at the level of the glottis, subglottis, and trachea were embedded in paraffin wax and processed for optical microscopy by staining with hematoxylin-eosin. The variables noted were mucosal status, necrosis of the cartilage, submucosal inflammatory components, and status of the thyroid gland. In case of premature death of the animal from postoperative complications, the lungs were also removed and sent for histologic examination.
All the animals received humane care in accordance with the Principles of Laboratory Animal Care as stated by the National Society for Medical Research and the Guide for the Care and Use of Laboratory Animals published by the National Institutes of Health (NIH Publication Number 85-23, revised in 1985).
Results
By the end of the scheduled observation period, 8 of the 10 rabbits continued without significant respiratory or deglutitory alterations. One animal did not achieve standard weight-gain, and 2 animals had died at 6 and 7 days after surgery, respectively.
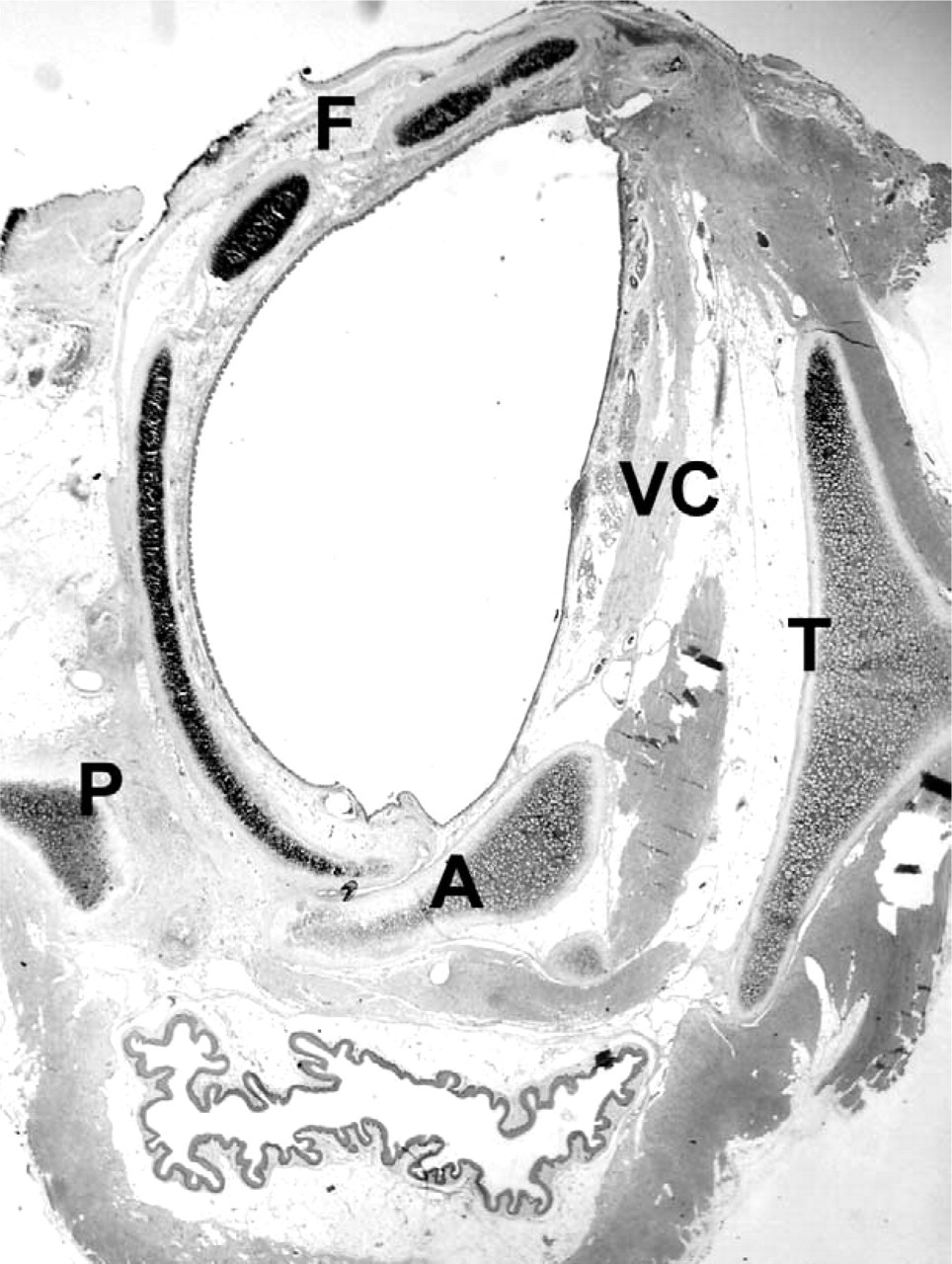
Cross-section at the level of the glottis (hematoxylineosin stain) (T, preserved thyroid cartilage; A, preserved arytenoid; F, tracheal flap covering the hemilaryngeal wound; P, posterior border of the resected thyroid lamina; VC, vocal cord).
Animals Sacrificed As Programmed
No severe alterations were observed in the endoscopy before sacrifice. Only minor alterations were observed in 3 cases: 1 vestibular inflammatory granuloma in the aforementioned case of low weight-gain, edema of the reconstructed arytenoids in another animal, and a small inflammatory granuloma along the suture line in another animal. The rest of the animals had suture lines that had healed well and with a normal aspect to the reconstructed hemilaryngeal wall. We did not observe any signs of infection, partial re-absorption of the flap, or laryngotracheal stenosis.
The histologic examination of the mucosal layer showed focal ulceration without necrosis in 1 case and a foreign-body inflammation reaction along the suture line in another. In the rest of the animals, the mucosa covering the tracheal patch was normal and the ciliated surface was conserved (Fig 5). There were no submucosal inflammation reactions. The cartilage of the tracheal patch showed neither partial reabsorption nor necrosis in any of the cases. The thyroid glands attached to the trachea were observed to be partially atrophied in the case that had presented with focal ulceration of the mucosa. In the rest of the cases, the gland did not show growth alterations related to vascularization.
Animals That Died Prematurely
The necropsy showed the presence of residual food in the trachea and the bronchus, and considerable pulmonary autolysis. An intense inflammation process with necrosis was observed together with loss of integrity of the mucosa and the cartilage of the tracheal flap and of the contralateral hemilarynx. No alterations were observed in the thyroid glands. Food aspiration was the most probable cause of death.
Discussion
The technique of reconstruction with an animal model, as presented in this study, has the advantage of being performed in a single surgical session and does not require provision for additional vascularization of the tracheal wall to be used as a flap. This is based on the observation that several centimeters of the trachea can be mobilized without creating excessive tension and can be sufficient to cover extended surgical defects resulting from hemilaryngectomy. The deglutitory function of the larynx was maintained while conserving the epiglottis and the aryepiglottal fold. Further, the mucosa of the superior border of the extirpated arytenoids was conserved so as to provide volume to the internal surface of the piriform sinus, as had been recommended by Delaere.7 It was not necessary to design procedures for glottis reconstruction in order to augment the volume of the glottis at the reconstructed site. The most difficulties encountered were in the reconstruction of the piriform sinus to avoid its collapse. This was probably the cause of the food aspiration in the 2 animals that died prematurely. Conserving the thyroid gland attached to the flap of the tracheal wall ensured a good vascular supply as was described by Ganon et al.12 However, we did not assess whether this was indispensable since the flap was not separated completely from the distal trachea but, instead, remained pedicled as an extension that approximated to half of the tracheal circumference. It is possible that this pedicle would be sufficient to achieve an adequate vascular provision. We are currently evaluating this hypothesis.
The anatomic characteristics of the rabbit are the bases of some uncertainties with respect to the possible applicability of the technique to human beings. In the rabbit, the thyroid gland covers the first 8 rings of the trachea and receives its vascular supply principally from the medial thyroid artery, originating in the common carotid, and via a medial descending branch, also irrigates the membrane and the lateral wall of the trachea. This branch proceeds to anastomose with the ascending branch of the tracheal-esophageal artery on both sides of the membranous section.14 Apart from this multiple and abundant tracheal vascular supply, the medial thyroid pedicle can be freed easily from the neighboring areolar tissue and allows for considerable elongation so that the elevation of the trachea does not compromise the vascularization. The human cervical trachea is irrigated principally by the inferior thyroid artery that contributes significantly to forming the lateral longitudinal tracheal anastomosis.
The superior thyroid artery does not supply branches directly to the trachea, except from across the thyroid glands, and irrigates a tracheal territory between 2 and 5 cephalic rings (1.7 ± 0.5 cm).2,15 It anastomoses with the inferior thyroid artery and can supply practically all of this territory.
The tight relationship that exists between vascularization of the thyroid gland and the trachea is the argument for maintaining the relationship intact between the glandular lobe and the tracheal wall, which is destined to cover the laryngeal wound.
The trachea of the rabbit is larger and more flexible that that in human beings and does not require any releasing maneuvers for it to be mobilized to cover the laryngeal wound. The human trachea can be elevated some 2 cm without requiring any freeing maneuvers.16 Delaere et al17 estimated that the mean length of an extended hemilaryngectomy wound is about 4 cm and that, in the technique of tracheal autotransplantation, it was not necessary to manipulate the trachea free so that it can be raised this distance to re-establish the laryngo-tracheal union.
The technique can be used in cancer patients with unilateral tumors of the glottis, with reduced or absent mobility of the vocal cords, but without anterior or posterior commissural involvement. It is also applicable in those cases with a subglottis extension that reaches, or proceeds beyond the upper border of the cricoid cartilages. Currently, the only conservative surgical technique for this type of tumor is that developed by Delaere et al.8 Furthermore, it can expand the indications for the use of the primary tracheal anastomosis technique described by Pearson et al9 and Grillo et al10 for those cases with benign subglottis stenosis but with concomitant involvement at the level of the glottis; both groups of authors indicate this as being the limiting factor of the technique.
Conclusions
The tracheal wall constitutes the donor tissue-of-choice for the reconstruction of surgical or trauma wounds of the larynx. The limitations of its use arise out of the necessity for revascularization with regional or free flaps. We have described a reconstruction technique in rabbits that covers extended surgical laryngeal wounds with the use of the tracheal wall and preserves normal vascularization. The technique is relatively simple and requires only 1 surgical session.