
Abstract
Materials and Methods
We accessed the 1998, 1999, and 2000 Nationwide Inpatient Sample (NIS; Healthcare Cost and Utilization Project Central Distributor, Silver Spring, MD), a publicly available database of hospital admissions from over 980 hospitals in 28 states. All records listing a primary admitting diagnosis of epistaxis (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9] diagnosis code 784.7) were extracted. Three separate subgroups were then created based on the type of treatment received by searching each admission for specific ICD-9 procedure codes as follows: (1) ligation group, codes 21.04 (“ligation, artery, ethmoid”), 21.05 (“ligation, artery, maxillary”), 21.06 (“ligation, artery, external carotid”), or 21.09 (“ligation, artery”); (2) embolization group, codes 38.80 (“surgical vessel occlusion NEC”) or 38.82 (“occlusion head/neck vessel NEC”) and 88.41 (“contrast cerebral arteriogram”); and (3) packing group, codes 21.01 (anterior nasal packing) or 21.02 (posterior nasal packing). Records containing more than 1 of the above procedure codes (ie, codes for both packing and embolization) were excluded from the treatment group analysis.
All data were analyzed and the 3 treatment groups compared with the use of the Statistical Package for the Social Sciences software (SPSS; Version 12.0; SPSS Inc, Chicago, IL). Demographic data were analyzed by frequency analysis (patient race, gender, type of admission, primary payer, secondary diagnoses, and procedures performed) or determination of means (patient age, number of secondary diagnoses, time from admission to index procedure, number of procedures performed). To assess outcomes for the treatment groups, we determined mean length of stay (LOS) and mean total hospital charges for each group. Mean total hospital charges reflects only those services billed by the admitting hospital. In addition, procedure codes for each record were searched for transfusion of whole blood (ICD-9 procedure code 99.03), packed cells (ICD-9 code 99.04), platelets (ICD-9 code 99.05), or serum (ICD-9 code 99.07). Lastly, the secondary diagnosis codes were searched for complications potentially related to epistaxis or its treatment, including pneumonia (ICD-9 codes 486, 997.3, and 507.0), stroke (ICD-9 codes 436 and 997.02), myocardial infarction (ICD-9 codes 410.1 to 410.9), angina pectoris (ICD-9 code 413.9), and blindness (ICD-9 codes 369.00, 369.60, 369.67, and 950.9).
Group demographics
For the statistical analysis, differences in demographic data between the treatment groups were analyzed with either one-way analysis of variance (ANOVA) with Tukey's post hoc test, or the cross-tabulation function of SPSS with the chi-square statistic. Differences in mean LOS and total charges between treatment groups were analyzed using one-way ANOVA followed by Tukey's post hoc test (or the nonparametric Kruskal-Wallis test when the equality of variances did not hold). Complication rate differences were examined with the cross-tabulation function of SPSS and analyzed with the chi-square statistic.
Results
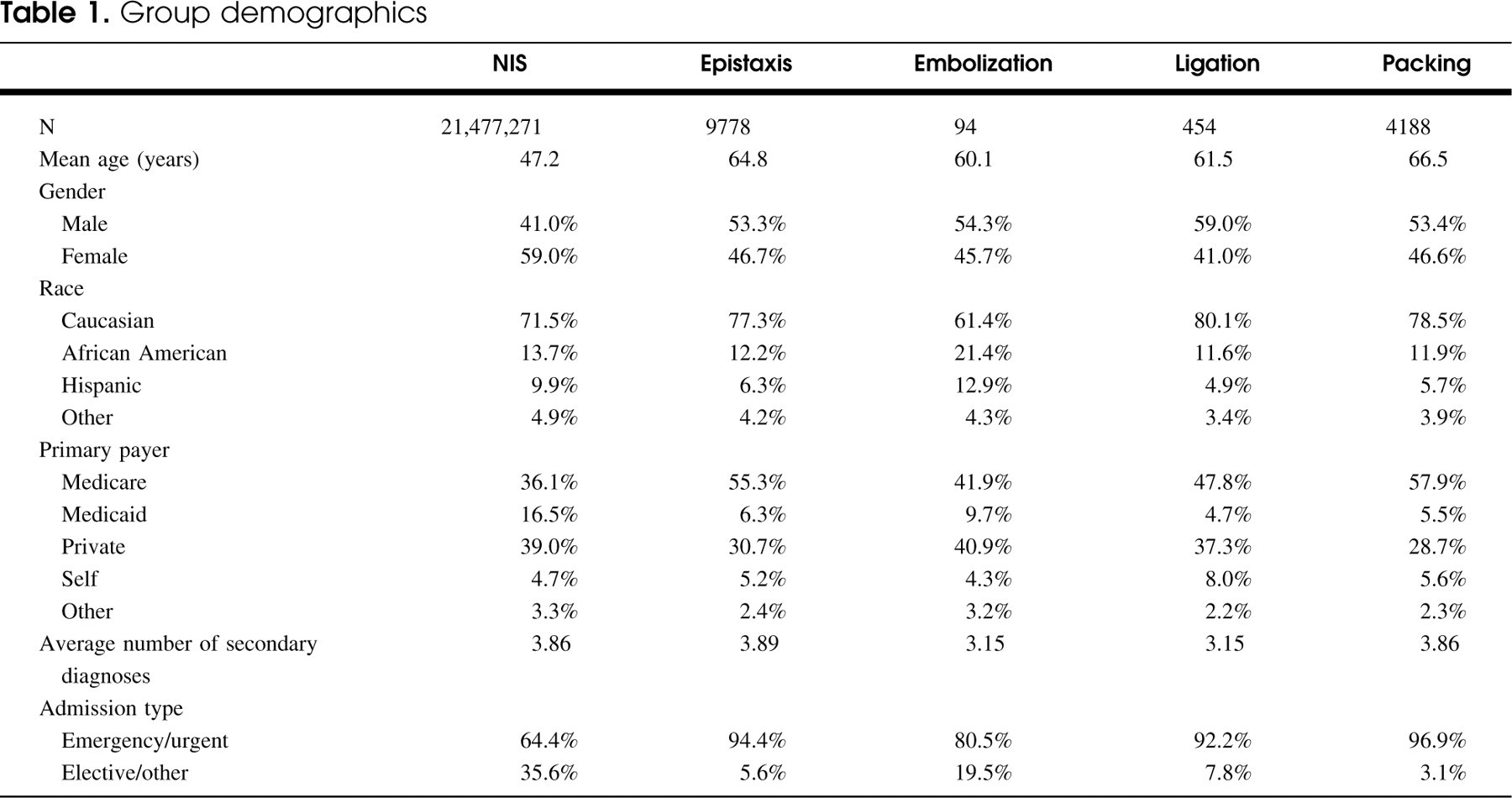
The combined NIS databases for 1998-2000 contained 21,477,271 admission records. Of these, 9,778 records (0.046% of the total) carried a primary diagnosis of epistaxis, referred to hereafter as the epistaxis group. This group was subsequently divided into 3 subgroups based on the type of treatment received: (1) ligation group (n = 454), (2) embolization group (n = 94), and (3) packing group (n = 4188). A total of 5042 records were excluded from the treatment subgroup analysis; 1698 had no procedures listed, 2547 had 1 or more procedures listed but none of the 3 procedures of interest; 797 had more than 1 of the above procedures listed. The demographic data for each group, and for the entire 1998-2000 NIS population, are shown in Table 1. Subjects in the epistaxis group had a higher mean age than the NIS population as a whole. Among the treatment groups, the packing group had a higher mean age than both the embolization and ligation groups (both P >0.005). The epistaxis group had a higher proportion of males than the NIS population, and the 3 treatment groups had similar gender distributions. No statistically significant difference in racial distribution was observed between the 3 treatment groups, although there was a trend toward higher proportions of African Americans and Hispanics in the embolization group. There were significant differences in the distributions of primary expected payers between all 3 treatment groups (all P >0.025, chi-square statistic). The main differences were a higher proportion of Medicare and lower proportion of private insurance in the packing group, and slightly higher proportions of Medicaid and private insurance in the embolization group. The average number of secondary diagnoses was higher in the packing group than in the ligation or embolization groups (both P >0.05). Almost 95% of admissions in the epistaxis group were classified as “emergency” or “urgent,” compared with only 64% “emergency” or “urgent” admissions for the entire NIS. Among the treatment groups, the embolization group had a significantly higher proportion of elective admissions than the other 2 groups (P >0.005).
Most common secondary diagnoses, epistaxis group (N = 9778)
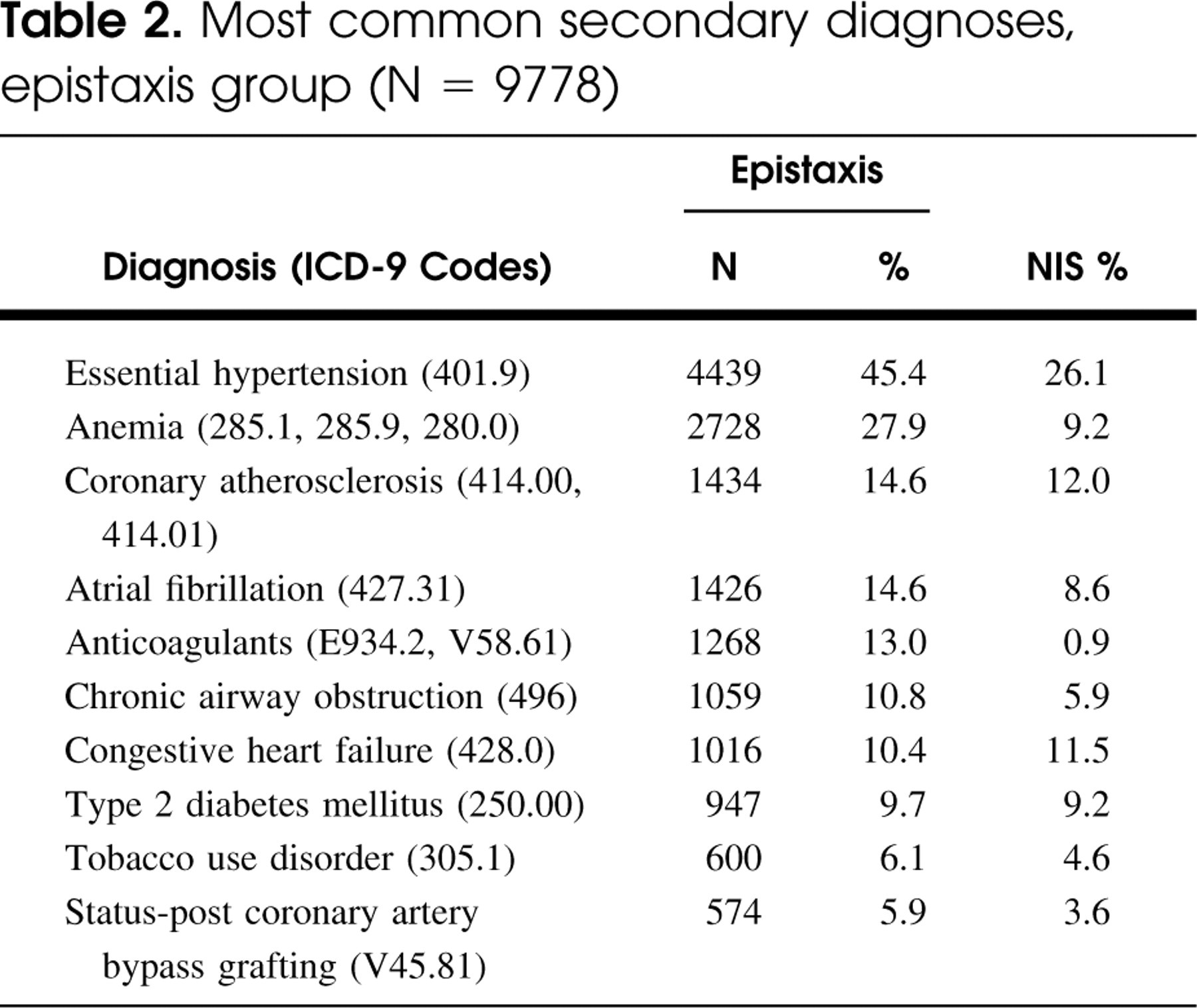
The most common secondary diagnoses for the epistaxis group are shown in Table 2. A high prevalence of hypertension and various cardiovascular disorders associated with anticoagulant or anti-platelet drug therapy was noted.
The mean length of hospitalization within the epistaxis group was 3.14 days (n = 9771), and the mean total charges per admission were $7616 (n = 9474). There were no significant differences between the mean lengths of stay for each of the treatment groups (Table 3). The mean time interval (in days) from admission until the index procedure was determined for each of the 3 groups (Table 3). Although the differences in this time interval between the 3 groups were all less than 1, all differences were found to be statistically significant by Student's t test (P >0.05). Mean total hospital charges were lowest for the packing group, and highest for the embolization group. The differences in total charges between the packing and ligation groups, and between the packing and embolization groups were significant (both P >0.05), whereas the difference between the ligation and embolization groups was not (P >0.25).
The packing group was also subdivided into admissions for anterior (n = 1859; ICD-9 code 21.01) or posterior (n = 2208; ICD-9 code 21.02) nasal packing. The mean LOS was 2.75 days for the anterior packing group and 3.53 days for the posterior packing group; the mean total hospital charges were $1269 less for the anterior packing group than for the posterior packing group (both differences significant by ANOVA, P >0.001).
Death rates in all groups were less than 1% (Table 3). This was lower than the death rate seen in the entire NIS population (2.4%). In the epistaxis group, the incidence of transfusion of whole or packed cells was 10.3%, whereas the incidence of serum or platelet transfusion was 3.5%. None of the differences in transfusion rates between the treatment groups achieved statistical significance (P <0.30), nor were there significant differences in the incidence of any of the complications analyzed between the treatment groups (all P <0.35).
Discussion
The present study seeks to assess the cost effectiveness and outcomes of commonly used methods for treating epistaxis in the inpatient setting. We chose to examine three treatments for epistaxis: nasal packing, arterial ligation, and intra-arterial embolization. This decision was prompted by the relative frequency with which these treatments are employed both in our own practice and in the literature, as well as our ability to segregate admissions into homogeneous treatment groups based upon the coding available in the NIS database.
In order to compare outcomes of the 3 treatments, we analyzed the mean total hospital charges, LOS, and complications for each group. The packing group was found to have significantly lower total hospital charges than either the ligation or the embolization groups. It should be noted that in all groups, the total charges include those accrued for the management of coexisting medical conditions, not just those charges associated with management of epistaxis. However, as the packing group had a higher mean number of secondary diagnoses than either of the other treatment groups, we can postulate that non—epistaxis-related charges should have been higher in this group. As the total hospital charges for this group were actually lower, we can conclude that the hospital charges associated with the management of epistaxis were indeed lower. A previous small retrospective study showed lower costs associated with posterior nasal packing compared with either angiography or surgical management, except in those patients requiring intensive care unit monitoring.1 However, Klotz et al,5 found that when used as first-line therapy for intractable epistaxis, surgical ligation is less costly than nasal packing. However, in their analysis, there was a significant difference in duration of hospitalization between those treated with nasal packing (5.29 days) and those treated surgically (2.1 days), which might account for the higher costs in the former group.5 Similarly, Wang and Vogel6 demonstrated that hospitalization times for patients treated with surgery alone was 2.2 days less than for patients receiving only nasal compression packing. In contrast, LOS in the present study was similar among the 3 treatment groups. We did find small but significant differences in the time interval from admission to procedure between our 3 treatment groups (Table 3). This suggests that patients in the embolization and ligation groups might have incurred additional hospital charges prior to treatment while necessary preparations were made, pre-procedure anesthesia evaluation was performed, or waiting for subspecialty personnel to become available before treatment could be provided. However, the rather small magnitude of the difference in this time interval and the rather large difference in total charges between the 3 groups makes it unlikely that the small differences in treatment timing alone accounted for all of the observed differences in mean charges. In addition, practitioners deciding between treatments for patients with epistaxis must also weigh the potential impact of such “real world” treatment delays. As such, inclusion of the likely small amount of hospital charges associated with initiation of invasive treatments might be considered appropriate for purposes of this analysis.
Outcome measures
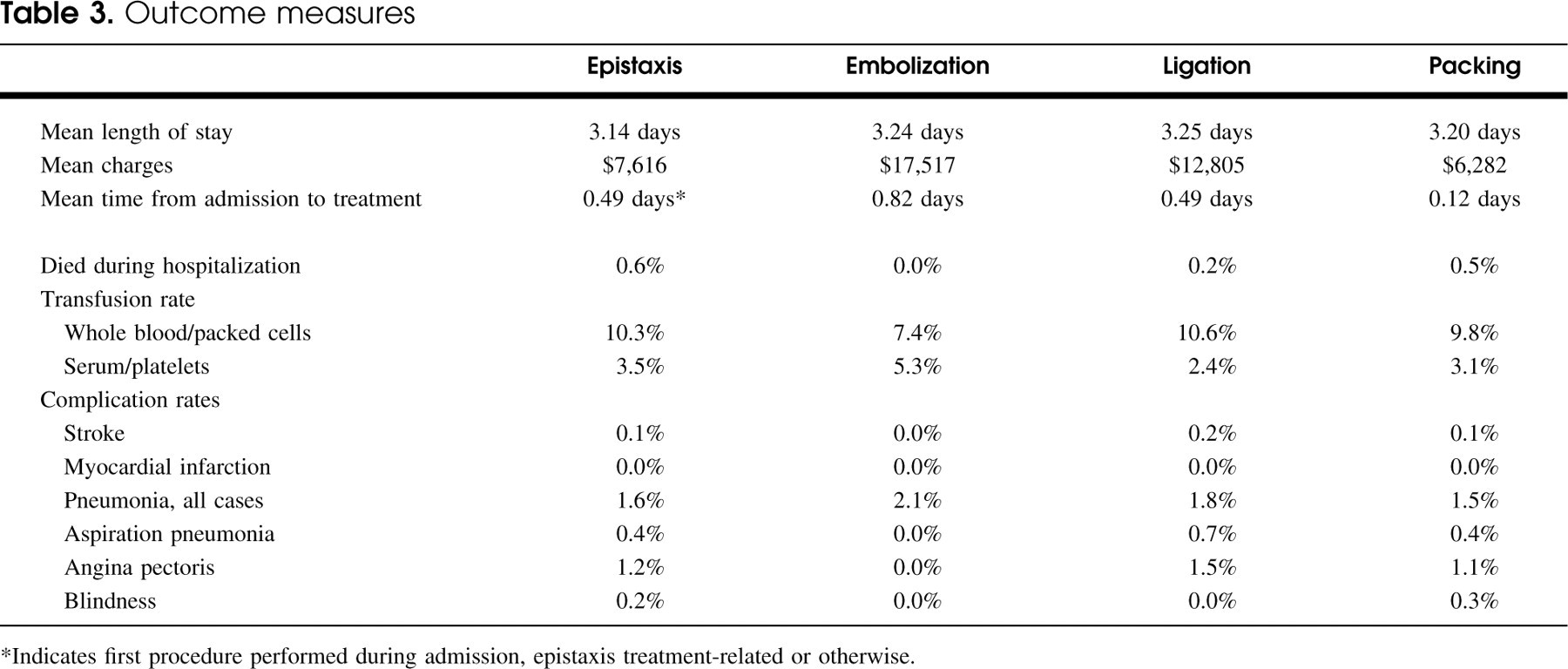
∗Indicates first procedure performed during admission, epistaxis treatment-related or otherwise.
As an indirect measure of the safety of the treatments studied, we determined the incidence of a number of potential complications and deaths during hospitalization for the 3 groups. As shown in Table 3, the rates of death and the complications listed were quite low, and there were no significant differences between the three treatment groups. Similarly, in the Monte et al1 study of treatments for posterior epistaxis, they noted none of the complications sought in our analysis, and had only 1 (2%) death, which was felt not to be directly attributable to epistaxis or nasal packing. They did, however, identify 2 (4%) cases of arrhythmias and several local complications due to nasal packing such as sinusitis, nasal alar necrosis, and facial swelling.
Assessment of the secondary diagnoses listed for each admission showed a higher prevalence of hypertension in the epistaxis group (45.4%) compared with both the NIS population (26.1%) and the general population of the United States (approximately 28% to 33%).9,10 Although a causative role of hypertension in severe epistaxis seems obvious, conflicting reports exist in the literature.3,7,11 Atherosclerosis and atrial fibrillation were also more prevalent in this population than in the NIS population. It is unclear whether a direct causative effect exists between atrial fibrillation or atherosclerosis and epistaxis, or more likely, if this observed association might be due to anticoagulant or antiplatelet therapy often used in the management of these disorders.12 In the epistaxis group, 13% of cases had anticoagulant use listed as a secondary diagnosis, compared with only 0.9% in the NIS population. As use of aspirin or other antiplatelet agents was not available from the secondary diagnosis codes listed, we would expect that the percentage of patients in the epistaxis group on some form of antithrombotic therapy to be significantly higher than 13%. The higher proportion of cases on anticoagulant therapy in the epistaxis group supports the rather intuitive contribution of such therapy in causing epistaxis. However, another plausible contributing factor for this disparity in the inpatient group studied here might be that patients with epistaxis and cardiac disease who require antithrombotic therapy, (such as atrial fibrillation and atherosclerosis), might be more likely to require hospitalization for cardiovascular monitoring than those patients with epistaxis but without cardiac disease, who are more likely to be managed safely on an outpatient basis.
There are a number of limitations to this study that limit its ability to guide treatment decisions. The NIS database represents a 20% sampling of nationwide hospitals and contains admissions from hospitals in only 28 states. Regional preferences in medical practice or patient demographics within these states may introduce selection bias inherent in any sampling. The validity of the NIS data rests on proper coding of all entries. Misinterpretation of patient documentation by nonphysician coders, miscoding, and code omissions or duplications might all introduce error, although we would expect similar rates of such errors in all groups studied. Lastly, “hospital charges” are not an ideal measure of the true “cost” of the treatments examined. Hospital charges may have little bearing on reimbursement, and thus may be a poor reflection of true cost. In addition, total hospital charges likely exclude charges for the services of non–hospital–employed physicians involved in treatment of epistaxis. As total physician charges are likely to be greater in patients treated by arterial ligation (surgeon and anesthesiologist fees) or embolization (interventional radiologist and anesthesiologist fees) than in those treated with packing, the differences in mean total hospital charges between the treatment groups may be an understatement of the differences in mean aggregate charges for the treatment groups.
The treatment groups have significant demographic differences, which might suggest a bias impacting physician treatment choices or alternately might have accounted for a portion of the observed differences in hospital charges. Although the treatment groups were well matched for gender and race, there were significant differences in mean age between the packing (66.5 years) and the other 2 treatment groups (60.1 and 61.5 years). This might reflect physician bias toward initiating less invasive management (ie, nasal packing) in older and potentially less healthy individuals. In addition, our data showed a statistically significant difference between the mean number of secondary diagnoses in the packing group (3.86) and the ligation or embolization groups (each 3.15). The presence of a greater number of secondary diagnoses, suggesting a greater number of comorbid diseases, rather than patient age itself, may have played a greater role in the choice of treatment. The choice of treatment used might also have been affected by the status of the primary expected payer for each admission. Although the higher proportion of Medicare patients seen in the packing group is likely just a reflection of the higher mean age of this group, the identification of patients with Medicare as the primary payer may have influenced physician choice with respect to treatment. Similarly, costly embolization may have been more likely to be proposed for patients with private insurance, leading to the higher proportion of private insurance in the embolization group. The type of admission (ie, emergency, urgent, etc) may have also influenced the treatment used or vice versa. The embolization group had a higher proportion of elective admissions than the other treatment groups, which suggests that embolization may have been reserved for less severe cases of epistaxis that did not merit urgent action or for cases that were electively admitted after failure of outpatient-based therapy. Other factors unavailable in the NIS, such as level of physician training or preference, availability of subspecialists (ie, interventional radiologists), or the size and type of hospital (ie, private vs teaching) may also have affected the choice of treatment, and thus the results of our treatment group analysis.
There are several other important factors to consider when assessing outcomes and costs for epistaxis treatments that could not be analyzed from the NIS data. These include the nature and extent of treatment administered before the index admission, the severity of bleeding, the location (anterior or posterior) of bleeding, recurrence rates, and patient quality of life. There is no specific code available in the NIS data to systematically identify those patients who may have had treatment before admission. As many practitioners use nasal packing as their initial treatment for epistaxis, there is a possibility that the packing group mostly contains patients admitted for their first intervention, whereas the ligation and embolization groups contain patients whose epistaxis was refractory to nasal packing placed in the outpatient setting or during a previous admission. By this logic, there exists a possibility that the packing group contains fewer cases of severe or refractory epistaxis, thus contributing to the observed lower total charges. Although the similarity of the transfusion rates for the 3 treatment groups argues that no major differences in the “average” severity of bleeding existed, this may not have been the case. More dramatic bleeding may prompt a treating physician to immediately move toward more aggressive and invasive treatment, such as embolization or surgical ligation. Differing proportions of anterior and posterior bleeds between the groups might have had significant effects on results, as posterior bleeds have been shown to command higher charges for their treatment.4 Indeed, from our own analysis, those in the packing group treated with anterior nasal packing had lower mean total charges and LOS than those treated with posterior packing. However, other than in the packing group as discussed, there was no way to determine the relative proportions of anterior or posterior bleeds from the NIS data. Recurrence or readmission rates are obviously important outcome measures when comparing treatments for epistaxis. Unfortunately, such information was also not available in the NIS. Lastly, in comparing treatments, it is important to assess their impact on patient quality of life. Although most prospective studies have not addressed this issue in epistaxis treatment, previous studies have reported major discomfort due to nasal packing.5,6,8 Surgical ligation, however, either by open or endoscopic approaches, may avoid some of the discomfort associated with nasal packing, but it is associated with risks of anesthesia and postoperative healing issues.3,5–8 Thus, if we assume similar rates of bleeding control and complications, the difference in treatment costs would need to be carefully weighed against increased patient discomfort and presumably lower quality of life.
Although many of the limitations noted in this analysis might be overcome by a well-designed prospective randomized trial that compares treatments, implementation of such a study would be difficult at best. A more feasible approach might be a large multi-institutional retrospective series, in which chart review would permit assessment of issues, such as preadmission treatment, location and severity of bleeding, recurrence or readmission rates, complications, and treatment-related patient complaints, might provide further clarification of the findings provided by our analysis of the NIS.
Despite the limitations of the data, our analysis suggests a cost benefit to nasal packing compared with embolization or surgical ligation for the treatment of epistaxis. Despite the lack of significance to the difference in charges between the ligation and embolization groups, there was a trend toward lower cost in the ligation group, which has been reported in previous studies.1,5 This suggests that ligation may be a more cost-effective management for epistaxis refractory to packing than embolization. Although our suspicion was that embolization might pose additional risks in terms of thromboembolic events, this was not borne out by the data. Other reports have similarly shown low rates of such complications from intra-arterial embolization in the management of epistaxis.13 Other than cost, in all likelihood the primary factor limiting more widespread use of selective intra-arterial embolization in the management of epistaxis is the limited availability in some localities of a skilled interventional radiologist capable of performing the procedure with minimal risk.
Conclusions
Epistaxis continues to be a common problem facing otolaryngologist–head and neck surgeons. We feel our data shows acceptably low rates of major complications, similar rates of transfusion, and similar length of hospital stay with nasal packing, arterial ligation, or intra-arterial embolization for the treatment of epistaxis. From a purely economic standpoint, nasal packing is associated with the lowest hospital charges of the treatments studied, and as such more invasive and costly treatments such as arterial ligation and embolization should be reserved for epistaxis refractory to packing. However, to assess the true cost-effectiveness of these treatments, data on pre-admission treatments, recurrence rates, and patient quality of life, which were not available for this analysis, are needed. Further studies on the efficacy of these treatments, as well as quality of life outcomes, are thus needed to further refine algorithms for the management of patients with epistaxis.
We would like to thank Misook Park, MS, from the Department of Biostatistics at Virginia Commonwealth University, for assistance with the statistical analysis.