
Abstract

A total of 78 suspected fish bone patients were treated at the outpatient clinic in our hospital from July 1, 2000 to December 31, 2001. All patients were examined with a tongue depressor used to inspect the hard and soft palate, anterior and posterior pillar, tonsils, and tongue. In cases where no fish bone was identified, indirect laryngoscopy (IDL) with a laryngeal mirror was performed. IDL is done by having the patient sit upright and extend his/her neck enough for the physician to see the entire oropharyngeal area. The patient's tongue is gently pulled out using the physician's nondominant hand. The patient is asked to breathe through his/her mouth while the laryngeal mirror in the dominant hand is used to examine the hypopharynx. The soft palate and uvula can be pushed backward with the mirror if necessary, to avoid touching the posterior pharyngeal wall so the gag reflex is not stimulated, and the fish bone can be removed when visible. Cases that failed to identify the fish bone with IDL were re-examined using a 4-mm or 5.8-mm 70 degree telescope (Karl Storz, Tutlingen, Germany) under either direct visualization through the scope or from a monitor (Sony Trinitron) connected to the video camera unit system. Patients with a negative finding from the telescope were recommended for endoscopy under general anesthesia.
For the technique with the telescope, the patient was asked to sit forward, with their back away from the seatback, and extend his/her neck. The telescope was held in the dominant hand and the patient's tongue gently pulled out with the other hand. Attention was first paid to the patient's most painful side. The telescope was passed into the patients' oral cavity and then oropharynx. The scope was stabilized so that the tip of the scope would not move by resting the scope on the patient's tongue. The scope was rotated to the left and right side with the tongue used as a fulcrum for detailed inspection of each side of the anterior and posterior pillars, tonsils, and lateral tongue base. Normally a 4-mm telescope was used to inspect these particular sites because of the wider angle of the smaller diameter rod lens, so the overall view was more clear. The tip of the telescope was positioned approximately 1.0 to 1.5 cm away from the area to be examined, careful not to touch the telescope to the posterior pharyngeal wall of the patient so the gag reflex was not stimulated.
Examination of the hypopharynx was performed by raising the eyepiece-side of the scope while the distal part and the tip of the scope were still at the same position. The scope could be advanced a few centimeters for improved inspection. Areas of examination were the entire base of the tongue, epiglottis, valleculae, pyriform sinuses, posterior pharyngeal wall, glottic opening, and postcricoid area. For difficult-to-see areas of the valleculae and pyriform sinuses, the patient was asked to say “e”, to make these areas more visible. At these sites, especially for a thin, small fish bone, a 5.8-mm, 70 degree telescope is more beneficial because of better magnification and illumination. Sensitive gag-reflex patients could be anesthesized locally with 10% lignocaine spray.
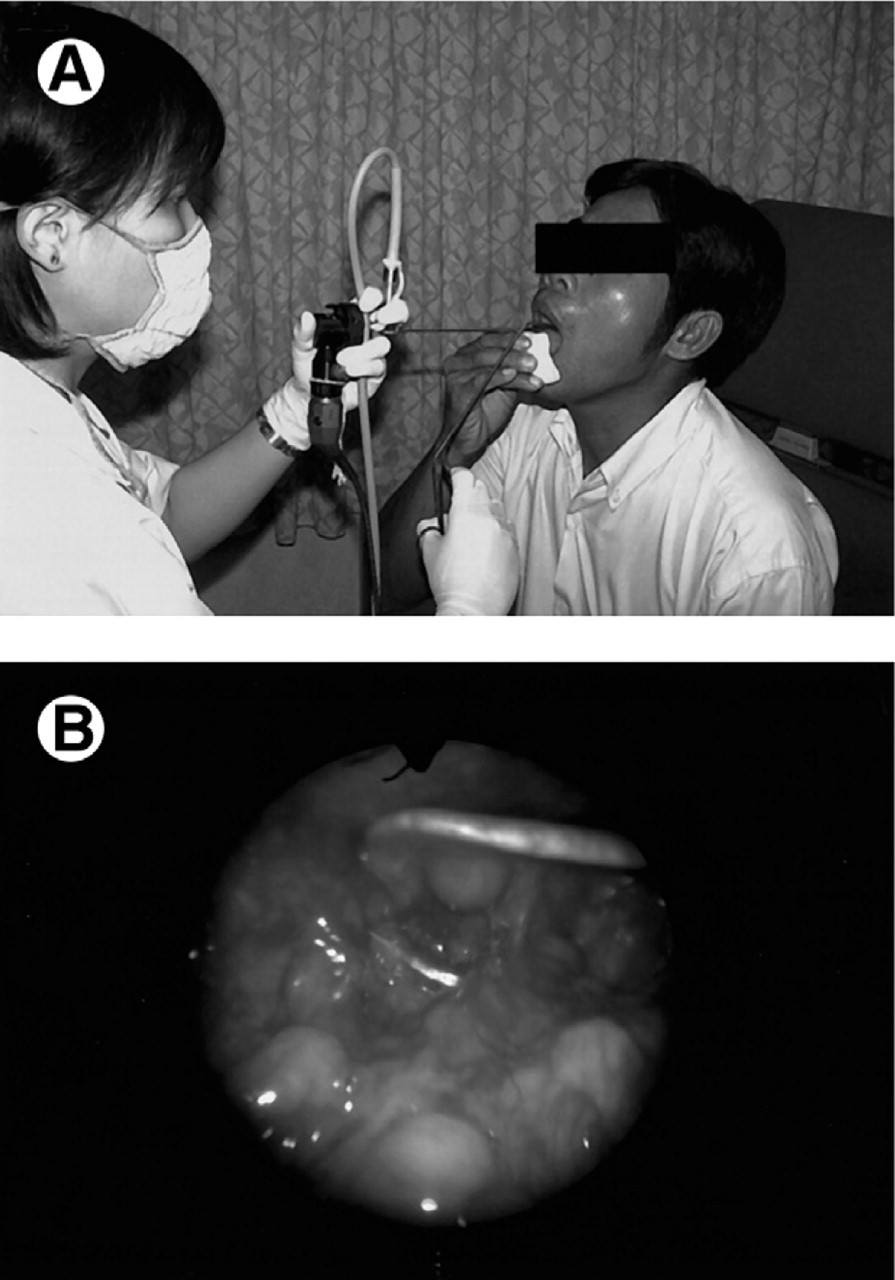
When a fish bone was identified, the telescope was changed to the opposite hand and the patient pulled out his/her own tongue. The fish bone was removed by using the removal forceps in the dominant hand (Fig 1 A). Two types of forceps were used depending on the site of the fish bone. An alligator forceps was used for removing higher-located fish bones, while a curved laryngeal forceps was used for removal of fish bones at a lower site. The technique to use the removal forceps was similar to use of the scope. The forceps was rested on the patient's tongue, making sure that the tip of the forceps was visible all the time of forceps manipulation. Orientation of the forceps tip was made compatible for grasping the fish bone, then the fish bone was removed. The patients could go home after the procedure without further observation in the hospital.
(
Diagnosis was successful by IDL examination in 52 (66.7%) of 78 cases. The remaining 26 cases were re-examined with a 70 degree telescope and a fish bone was detected in 22 cases (84.6%), mainly located at the inferior pole tonsil and valleculae (Fig 1 B). Four cases in which telescopy failed to identify the fish bone were referred for endoscopy with the patient under general anesthesia; fish bones were found embedded in the inferior pole tonsil (1 of 4), at the postcricoid area (2 of 4), and at the posterior pharyngeal wall (1 of 4). There were no significant complications in this series.
A 70 degree telescope is very beneficial in the diagnosis and removal of impacted fish bones, especially at the base of the tongue, inferior pole tonsil, valleculae, and supraglottic area. It is very useful in reducing the risk and cost of general anesthesia and is recommended as an alternative procedure when fish bone retention of the upper aerodigestive tract is suspected.