
Abstract

CASE REPORT
A 69-year-old female without significant medical history presented to the Albany Medical Center Hospital Emergency Department with an acute episode of shortness of breath. On initial evaluation, the patient appeared in respiratory distress with significant stridor. As a result, an Otolaryngology–Head and Neck Surgery consultation was obtained to evaluate the patient for possible upper airway obstruction. Examination of the oral cavity demonstrated macroglossia and an edematous soft palate. Palpation of the neck did not reveal a goiter or other masses. Further examination showed findings consistent with hypothyroidism, such as pitting edema, periorbital and facial edema, and thinning of outer halves of eyebrows. Flexible fiberoptic laryngoscopy demonstrated supraglottic edema with upper airway obstruction (Fig 1). Laboratory data were unremarkable, with the exception of the results of the thyroid function tests that demonstrated an elevated TSH and low free T4 (0.4 ng/dL, with normal as 0.7 to 1.48). Further testing revealed no elevation of microsomal or thyroglobulin antibodies. Hypothalamic and pituitary hormone levels were also normal. The patient required fiberoptic nasotracheal intubation and subsequent tracheotomy. During tracheotomy, a thyroid biopsy was obtained and demonstrated findings consistent with atrophic thyroiditis, which include extensive fibrosis, lymphocytic infiltration, and loss of normal lobular architecture with a paucity of follicles (Fig 2). Due to the patient's overt hypothyroidism, she was started on thyroid hormone replacement therapy with intravenous levothyroxine. Subsequent thyroid function testing demonstrated normalization of TSH and free T4 levels. Follow-up laryngoscopy was performed 2 weeks after the initiation of therapy and revealed resolution of supraglottic myxedema with a widely patent airway. The patient did not receive antibiotics nor did she receive either steroid or antireflux medications during her hospitalization. The patient was decannulated without difficulty 3 weeks after tracheotomy.
DISCUSSION
Hypothyroidism occurs with increasing frequency throughout life, affecting women 4- to 6-fold more often than men. The commonest cause of goitrous hypothyroidism in adults in the United States is autoimmune thyroiditis (Hashimoto's disease). Nongoitrous hypothyroidism is most often caused by autoimmune diffuse thyroid atrophy (atrophic thyroiditis), management of Graves' disease with 131I, thionamides, or thyroidectomy. In the adult, early symptoms of hypothyroidism are nonspecific and of insidious onset. Initially, the symptoms may include fatigue, lethargy, constipation, cold intolerance, stiffness, cramping of muscles, and menorrhagia in the female. Subsequently, the patient may develop dry skin with coarse hair, hoarseness of voice, and hearing loss. Also, obstructive sleep apnea may occur. Ultimately, the clinical picture of florid myxedema appears with dull expressionless face, sparse hair, periorbital puffiness, large tongue, and pale cool skin that feels rough and doughy. In fact, the term myxedema connotes severe hypothyroidism in which there is accumulation of hydrophilic, mucopolysaccharides in the ground substance of the dermis and other tissues. If left untreated, the patient with severe, long-standing hypothyroidism may pass into a hypothermic stuporous state known as myxedema coma. Respiratory depression is an important component of this state. The patient typically presents with hypotension, hypothermia, and hypercapnia. Factors that predispose to myxedema coma include cold exposure, trauma, infection, and the administration of central nervous system depressants.
Gupta et al 1 studied the otolaryngologic manifestations of hypothyroidism. The findings included rhinorrhea and globus sensation with pale, edematous nasal and pharyngeal mucosa. Bicknell 2 believed that hoarseness was less likely caused by stretching of the recurrent laryngeal nerve by the thyroid gland, but rather was due to myxedematous thickening of the vocal cords. In primary myxedema, which is the outcome of atrophic thyroiditis, the deposition of mucopolysaccharides into the tissues of the hypopharynx result in edema of the supraglottic structures. 3 Thus, supra-glottic myxedema may result in upper airway obstruction. Recently, immunohistochemical studies of human cadaveric larynges demonstrated the presence of thyroid hormone receptors in the human larynx. 4 Although tracheal compression may occur secondary to goiter, it is uncommon for hypothyroidism to result in upper airway obstruction at the level of the supraglottis or glottis. In fact, review of the literature demonstrates 1 case report of a patient with overt hypothyroidism who presented with upper airway obstruction which improved with levothyroxine therapy. 5
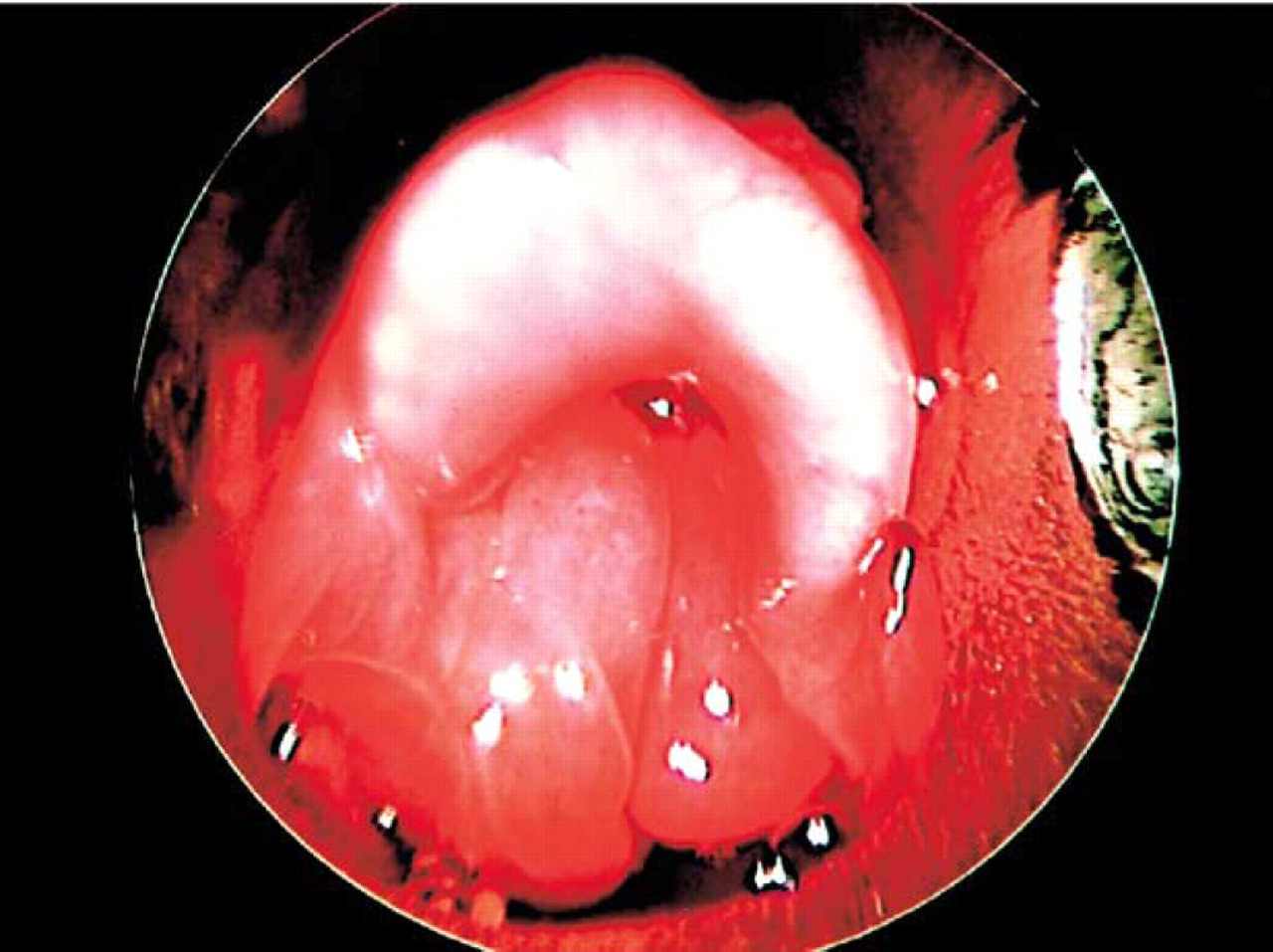
Intraoperative view of supraglottic structures during rigid laryngoscopy. The image depicts significant edema of bilateral arytenoids, resulting in upper airway obstruction. (Photograph obtained with 0 degree rigid endoscope [Richard Wolf, Vernon Hills, IL] via rigid laryngoscopy with Dedo laryngoscope [Pilling Surgical, Horsham, PA].)
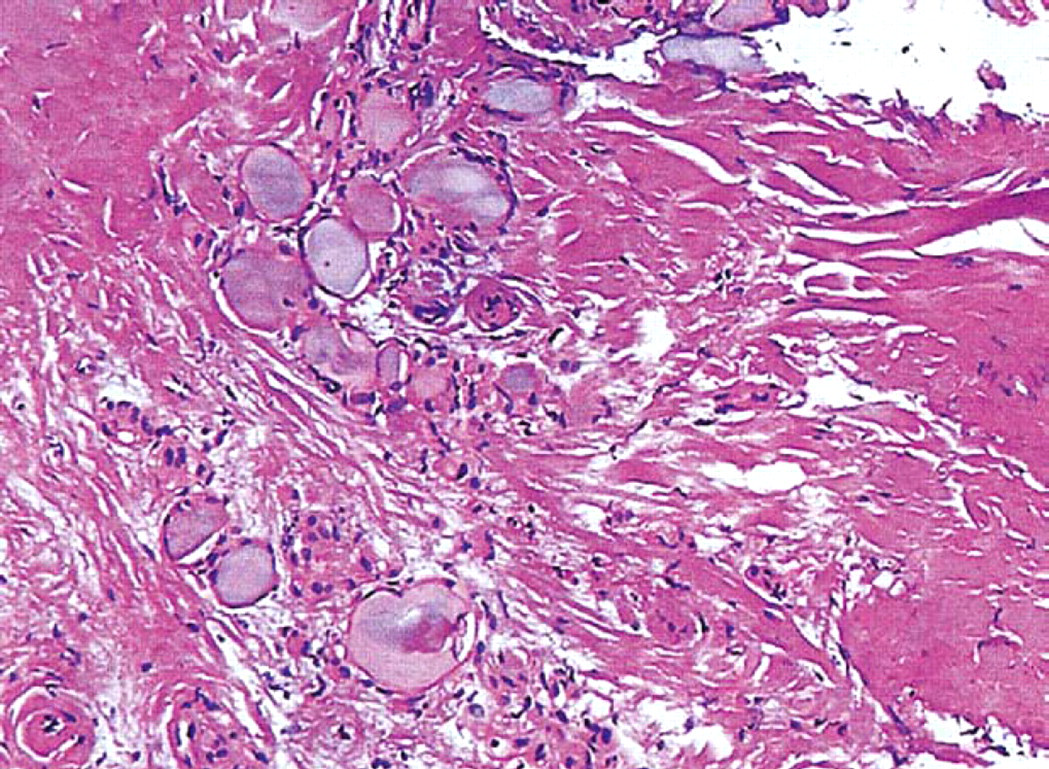
Biopsy findings are consistent with atrophic thyroiditis that include extensive fibrosis, lymphocytic infiltration, and a loss of normal lobular architecture with a paucity of follicles. (Hematoxylin and eosin stain; original magnification (
In this case report, the patient presented in respiratory distress with stridor, signifying upper airway obstruction. Flexible laryngoscopic evaluation demonstrated supra-glottic edema. Further evaluation demonstrated overt hypothyroidism that was confirmed with a high TSH and low free T4. Although the patient did demonstrate findings consistent with primary myxedema, she did not present with myxedema coma. Initial therapy included establishment of a secure airway. The diagnosis of atrophic thyroiditis was made based on overt hypothyroidism, the absence of goiter, negative microsomal and thyroglobulin antibodies, and the findings on biopsy that included fibrosis, lymphocytic infiltration, and a loss of normal lobular architecture with a paucity of follicles. The patient received levothyroxine intravenously with subsequent resolution of supraglottic edema 3 weeks after tracheotomy.
We would like to thank Donna M. Vincenti, MD, for preparation and analysis of photomicrographic material.