Abstract
EBM RATING: C
Primary hyperparathyroidism results in metabolic imbalances with subsequent symptoms. The resolution of this is achieved via the excision of the hyperfunctioning parathyroid gland, which requires both the successful identification and removal of the offending gland. This is both an intraoperative surgical and pathologic assessment, mandating close cooperation between both surgeon and pathologist. Ideally, the pathologic technique used for tissue confirmation should provide accuracy and reliability and afford the greatest speed. 1 Conventionally, tissue confirmation has been achieved by using intraoperative frozen section (FS), which has been reported to have an overall accuracy rate of 99.2%. 2 However, is has been suggested that FS is time consuming, irretrievably utilizes tissue, 3 and is costly. It also has been stated previously that an experienced surgeon can identify parathyroid tissue in situ using gross confirmation alone and differentiate it from other tissue types, without the assistance of a pathologist. 1,4 These include lymph nodes, adipose tissue, thymus, and thyroid tissue. This claim has not been confirmed by rigorous analysis, nor has it been compared with the current gold standard for intraoperative tissue identification, FS diagnosis. Furthermore, with the advent of preoperative radionucleotide scanning using technetium-99m sestamibi scanning (MIBI) and intraoperative quick parathyroid hormone (QPTH) monitoring to identify abnormal hyperfunctioning parathyroid glands, the role of the FS in the intraoperative diagnosis of abnormal parathyroid glands once again has been called into question. 5
The aim of this study was to assess the need for routine FS in tissue identification during parathyroidectomy in a series of 50 consecutive cases.

Gross appearance of a parathyroid adenoma. Note the glistening, encapsulated, and lobated appearance.
MATERIAL AND METHODS
We analyzed our experience with 50 consecutive parathyroid procedures performed by a single surgeon (B.C.S.; 20 excisions and 30 biopsies leading to excision), undertaken for primary hyperparathyroidism (35 adenoma, 15 hyperplasia), at Penn State Milton S. Hershey Medical Center (HMC). These cases were accessioned to the Surgical Pathology Service in the Department of Pathology, HMC, between December 2002 and August 2003. All 50 cases had tissue submitted for intraoperative FS consultation. Both the surgeons' assessment and the pathologists' opinion on intraoperative consultation (gross examination [GE]) were recorded independently so as to avoid bias (Fig 1). Touch imprints, scrape smears, as well as FSs then were performed for definitive tissue identification (Figs. 2–4). Touch imprint evaluation was performed by lightly touching the fresh-cut surface of the specimen to a glass slide 3 times. The slide was fixed immediately in 95% alcohol for 30 seconds and then stained by using hematoxylin and eosin. Smear imprint evaluation was performed by scraping the cut surface with a scalpel or edge of a glass slide and smearing the material onto a glass slide, which was fixed immediately in 95% alcohol for 30 seconds and then stained with hematoxylin and eosin. The FS was performed by embedding the tissue in O.C.T. Compound (Tissue-Tek; Sakura Finetek USA, Torrance, CA), which then was rapidly frozen. Sections 6 μm in thickness were cut, fixed in 95% alcohol for 30 seconds, and subsequently stained with hematoxylin and eosin stains.
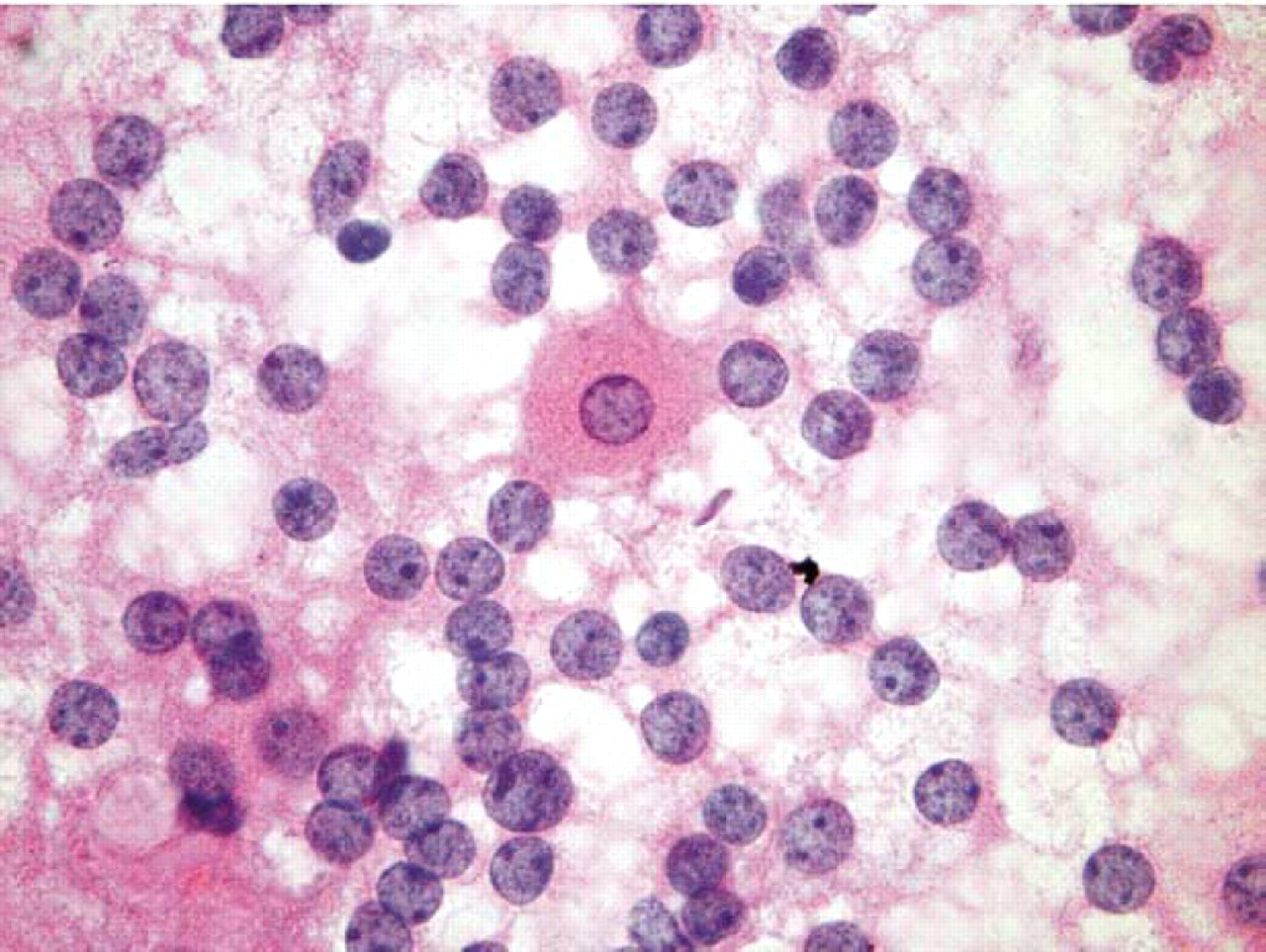
This touch preparation demonstrates naked nuclei with salt and pepper chromatin residing within a lacy pink background composed of parathyroid gland cell cytoplasm that has been stripped from the nucleus, a single intact parathyroid cell can be visualized in the center of the field (hematoxylin and eosin stain, X1000).
Cost-effectiveness of FS was evaluated by using a decision model (Fig 5). The model was parameterized by using data from the literature, and cost data are from our institution for the current fiscal year (2004). The cost of performing an intraoperative consult with FS was $294, and the additional cost of performing a touch prep and smear prep was $53. The cost of the parathyroidectomy procedure (inclusive of imaging and laboratory testing) was $4534 (unilateral neck exploration), ranging up to $7548 (bilateral neck exploration). The cost of a preoperative sestamibi was $754, and the QPTH was $28. The sensitivity, specificity, and frequency of removal on non-parathyroid tissue associated with GE were based on our data. However, because no specimens removed were suspected of being nonparathyroid in origin that were confirmed not to be parathyroid on FS, the specificity was 0. To examine the robustness of our model to this parameter, we performed a 1-way sensitivity analysis. The sensitivity and specificity of FS both were assumed to be 94% based on Shidham et al. 7
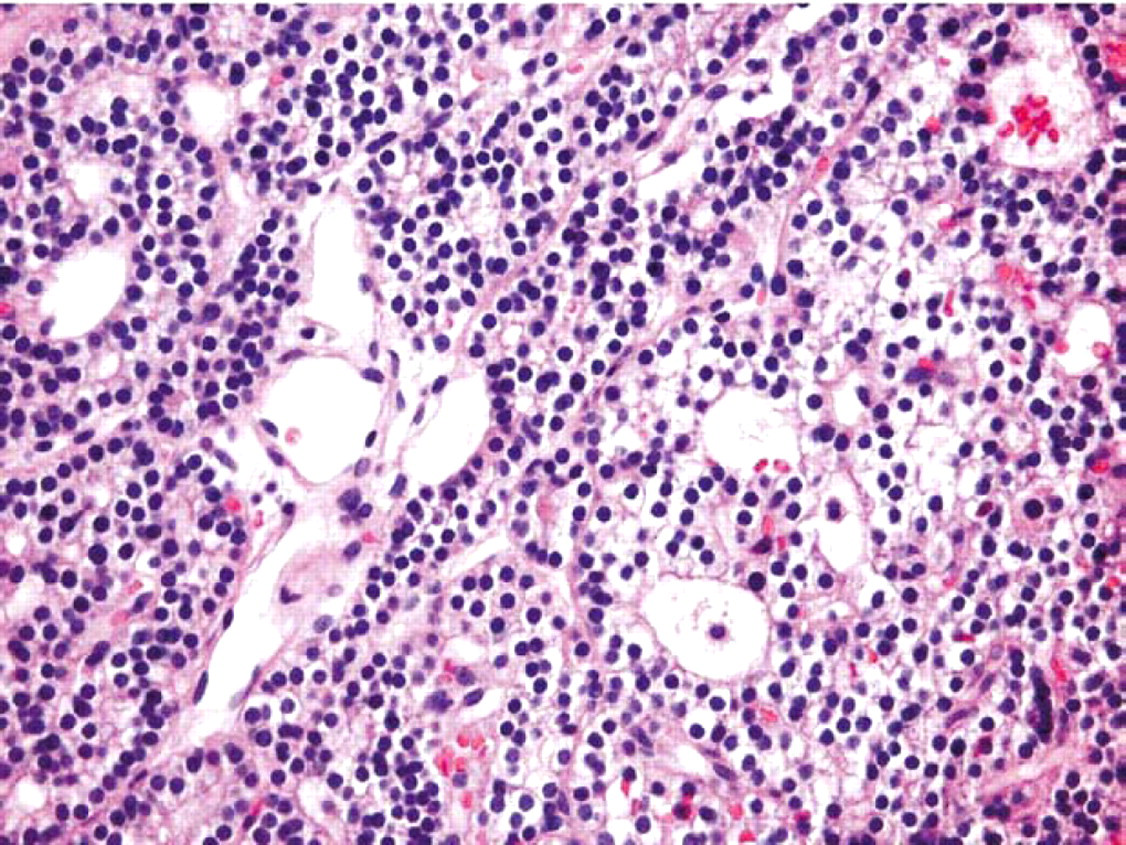
Frozen-section histology demonstrating sheets of cells with no parenchymal fat, within a parathyroid adenoma (hematoxylin and eosin stain, X 400).
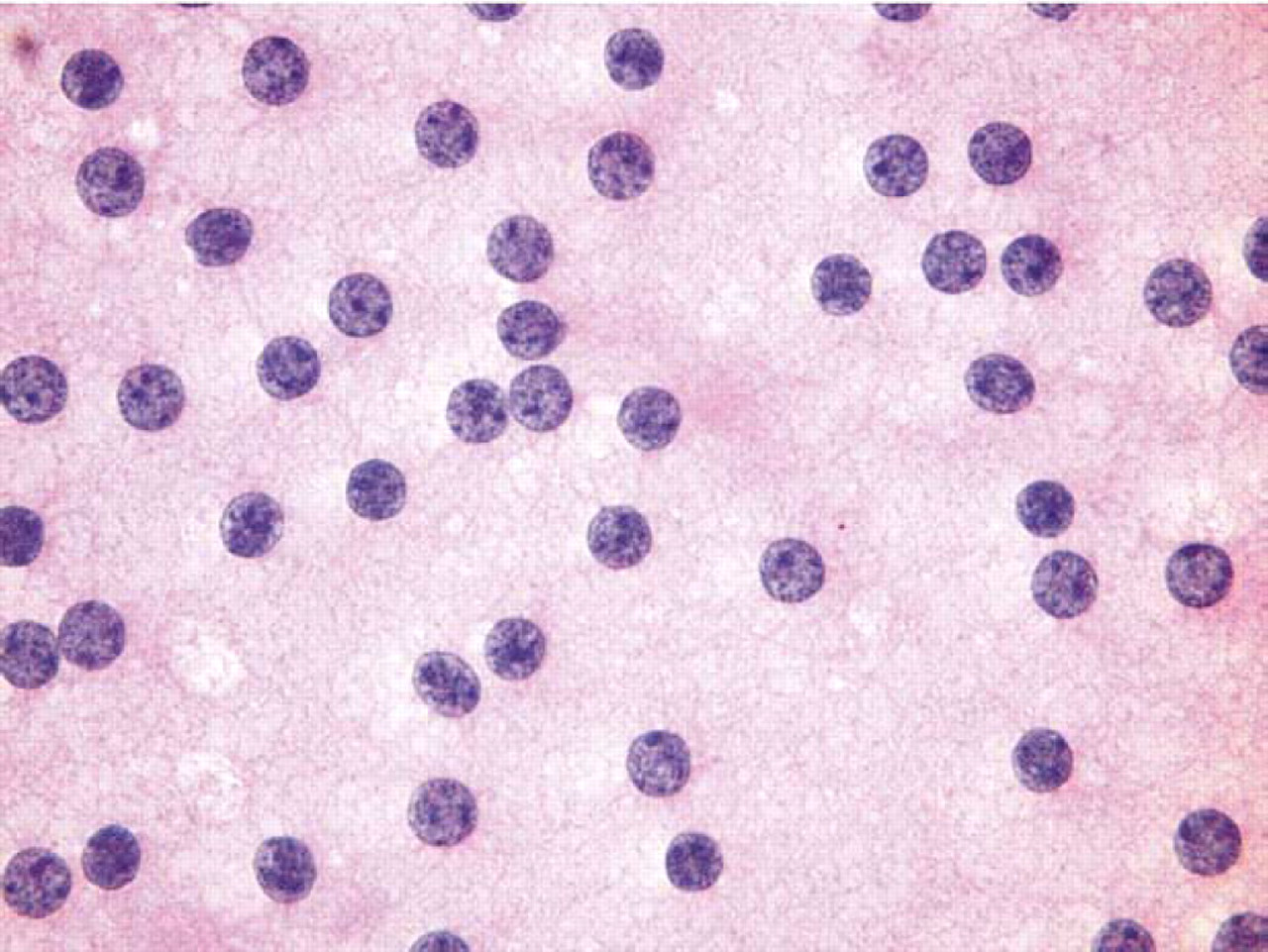
This smear preparation also demonstrates naked nuclei with salt and pepper chromatin residing within a lacy pink background composed of parathyroid gland cell cytoplasm that has been stripped from the nucleus (hematoxylin and eosin stain, X 1000).
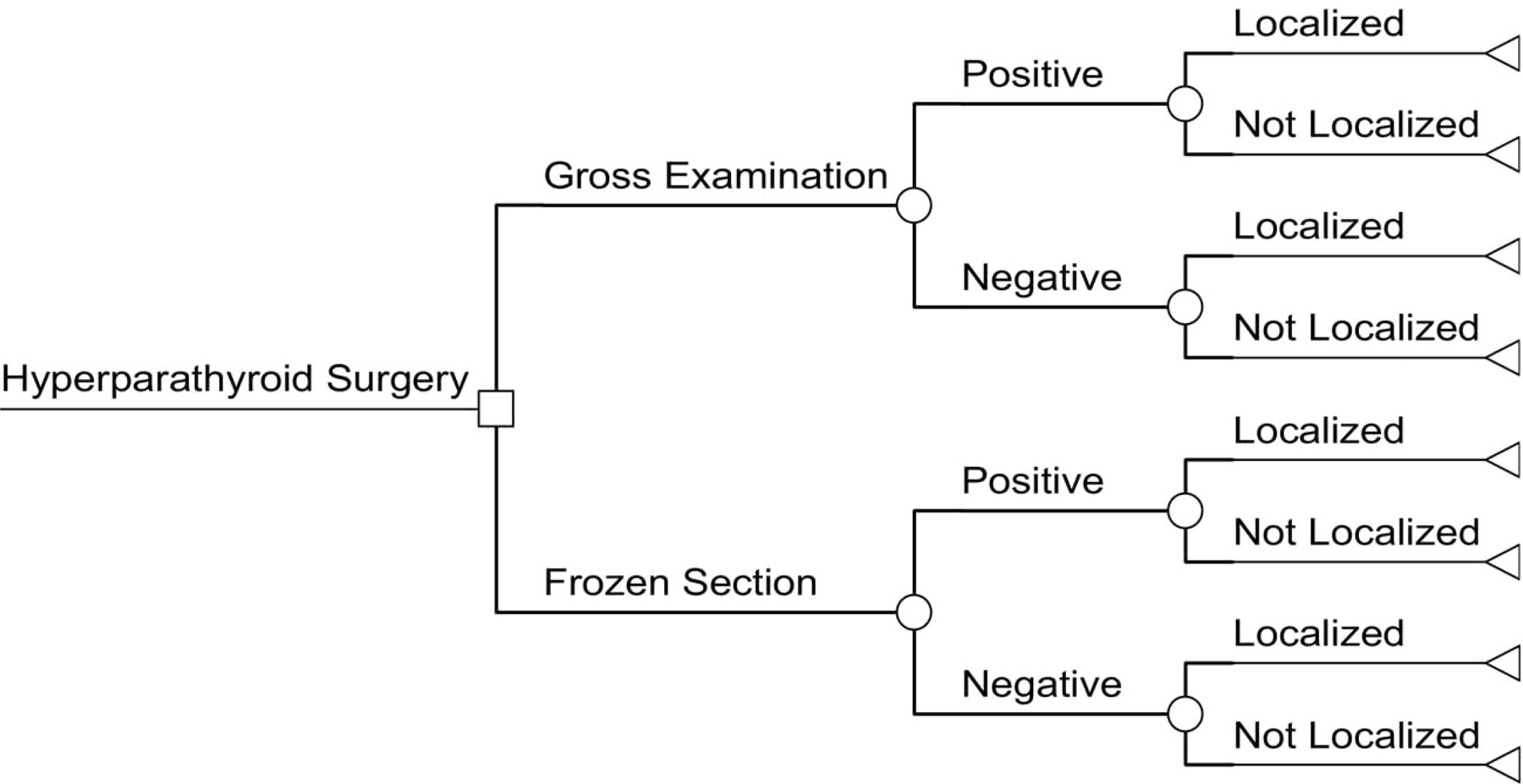
Decision tree for cost-effectiveness of frozen section (FS) versus gross examination (GE).
RESULTS
The cases submitted for intraoperative GE varied from small biopsy fragments weighing only 100 mg to fully encapsulated parathyroid glands weighing up to 16.1 g. The specimens examined ranged in color from mahogany red-brown to a yellow-tan color, with the majority being homogenous on cut section; however, 1 case demonstrated an area of cystic degeneration, and several specimens demonstrated a rim of yellow tissue.
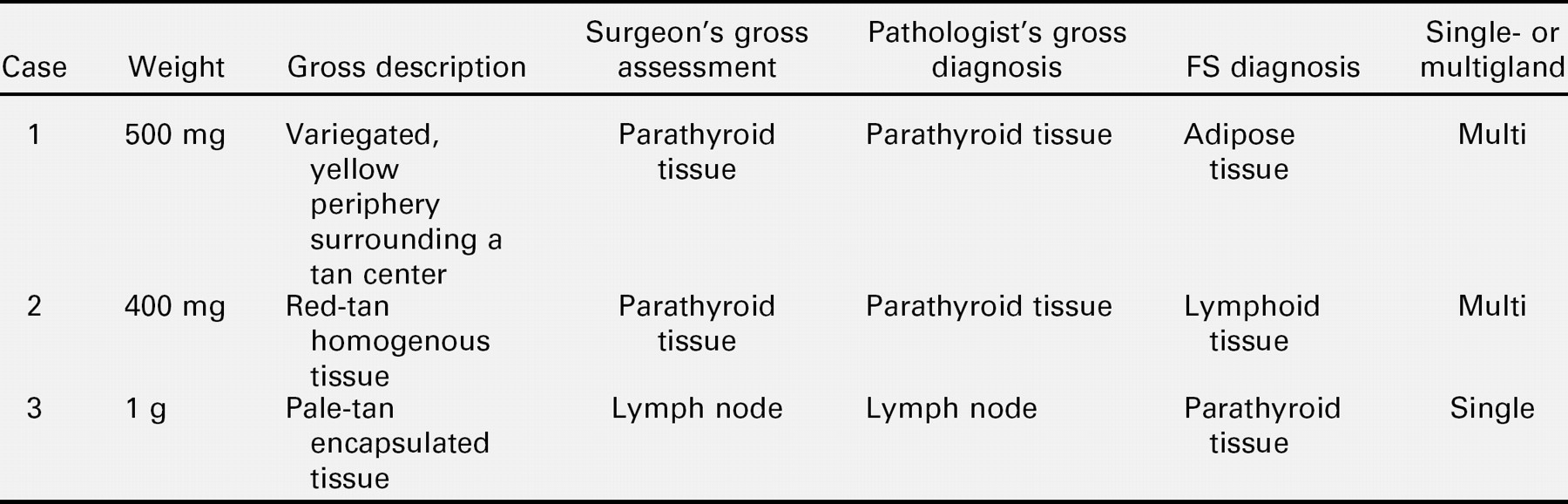
Of the 50 parathyroidectomy procedures performed, both the surgeon's and pathologist's gross opinions were concordant in all cases. However, incorrect gross identification of parathyroid tissue occurred by both the surgeon and pathologist in the same 3 cases (6%; table 1). Tissue mistaken for parathyroid tissue on GE included fat (1 case, 2%) and lymph node (1 case, 2%), and in 1 other case (2%), tissue submitted as probable lymph node on GE resulted in the FS tissue diagnosis of parathyroid tissue. In all 3 cases, the cytologic findings corroborated the FS findings. FS and cytologic examination confirmed the gross diagnosis of parathyroid tissue in the remaining 47 cases (94%). There was a 100% concordance between cytology and FS in our series.
The case of fat misidentified as parathyroid tissue was a biopsy specimen and consisted of a dark red-brown piece of tissue with a yellow rim. The 2nd misidentification case was that of lymphoid tissue incorrectly called parathyroid tissue, the specimen was an encapsulated pale tan nodule, which was shown to be a lymph node via FS. The 3rd misidentification case was in fact a biopsy fragment of dark red-brown tissue, which was grossly called lymph node and was shown to be parathyroid tissue via cytology and FS.
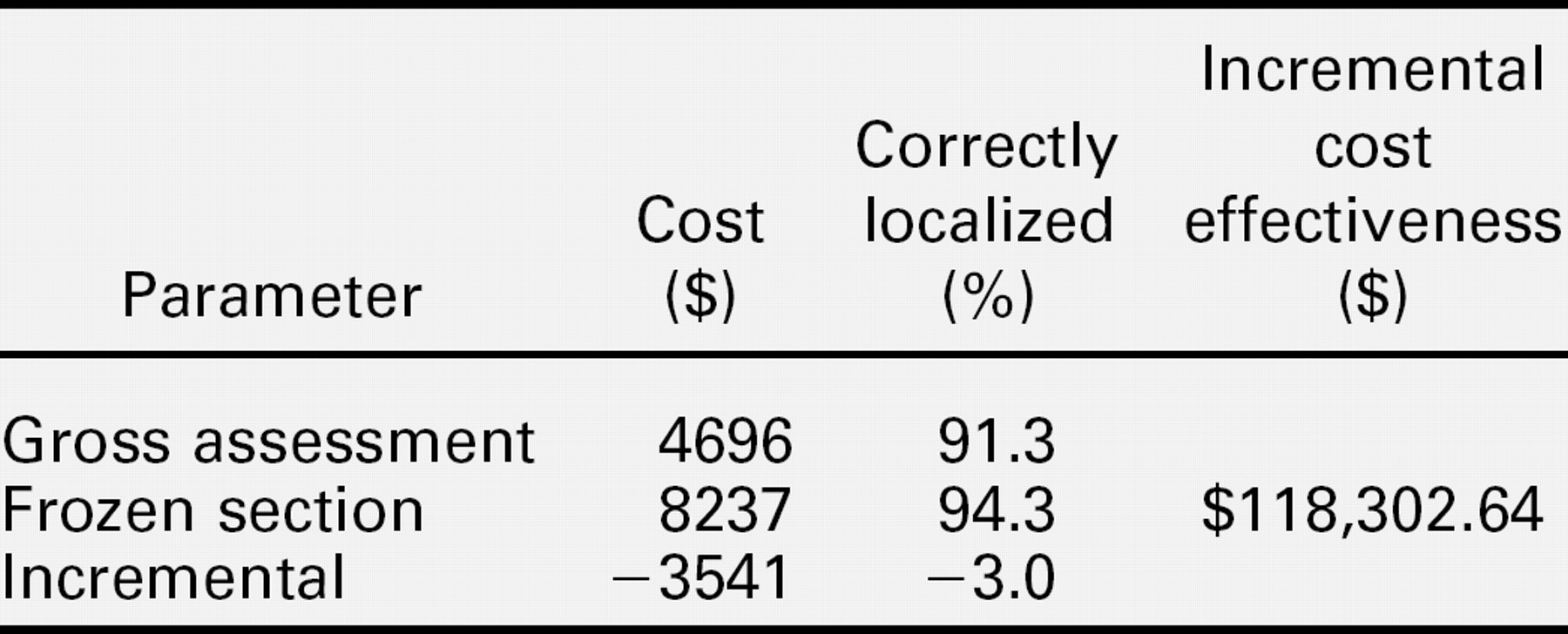
In the baseline cost-effectiveness analysis, in which specificity was assumed to be 0 for GE, the GE approach was less costly than the FS approach, but it also was less effective (table 2). Thus, it may be considered cost effective if the decision maker is willing to accept $118,303 in savings per case incorrectly localized. In 1-way sensitivity analysis in which specificity of GE was varied from 0 to 1, the GE approach became dominant (ie, less costly and more effective) for values of specificity of ≥60% (Fig 3).
DISCUSSION
Parathyroid exploration surgery has undergone many changes over time, and we now have access to an unprecedented number of techniques to minimize operative failure. The abundance of choices must be tempered not only by accurate diagnosis but also by financial prudence. Currently, the FS is considered the gold standard for intraoperative parathyroid tissue confirmation, with a reported accuracy rate of 99.2%. 2 However, even with this high accuracy rate, operative failures still are being cited secondary to FS misinterpretation. 7,8 Parathyroid histopathologic interpretation of an adenoma versus hyperplasia is considered by many pathologists to be a persistent challenge.
Three cases with discordant findings on gross examination and FS diagnosis
The advent of preoperative localization techniques, such as MIBI, and the development of the intraoperative QPTH has impacted upon the operative success rate of both initial parathyroidectomy and repeat parathyroidectomy. Boggs et al 6 reported that with the combined use of these techniques, in addition to the use of FS examination, their operative failures dropped from 10% to 1.5%. Thus, given the advent of preoperative localization using MIBI and intraoperative physiological monitoring using the QPTH assay, the role of the routine FS has understandably been called into question. As such, previous statements to the effect that experienced parathyroid surgeons usually can make the distinction between parathyroid tissue and other tissues warrant reevaluation. 1,4
Our study has shown that using preoperative MIBI and gross observation by both the experienced parathyroid surgeon and pathologist resulted in a true-positive parathyroid identification rate of 94%, which was confirmed by intraoperative cytology and FS. However this result is tempered by the potential for a 6% operative failure rate. The 6% error rate in gross tissue identification was caused by the mis-identification of fat in 1 case and lymphoid tissue mistaken for parathyroid or vice versa in 2 other cases. The differential diagnosis of specimens brought out of the operating room for tissue identification in parathyroid explorations includes parathyroid gland, thyroid gland, lymph nodes, adipose tissue, thymus, and skeletal muscle. This differential is always at the forefront of both the surgeon and pathologist's mind when assessing a specimen submitted for intraoperative assessment during a parathyroid exploration. In all cases, both correct and incorrect, the pathologist's and surgeon's gross opinion on intraoperative GE were concordant.
In the majority of cases evaluated, the gross identification of parathyroid tissue was fairly straightforward, as these conformed to the classical gross description of a red-brown tissue (because of the decreased stromal fat) and homogenous consistency. This classically is seen in single adenoma disease. The appearance of parathyroids in multigland disease is highly variable. Several of our cases strayed from this typical gross description and demonstrated evidence of hemorrhage, cystic degeneration, and variation in both size and shape. This may be due to our mix of single and multigland specimens analyzed. This made gross identification in these cases much more challenging. Furthermore, the gross appearance of tissues considered within the differential, such as thyroid, lymph node, fat, thymus, and muscle, also were noted to be similar to the gross appearance of parathyroid tissue, especially on smaller biopsy specimens. This made correct gross-tissue identification of parathyroid tissue potentially difficult and resulted in the 6% identification error rate in our study. The adjunct of intraoperative radioguided surgery was used in cases of solitary adenoma. QPTH was used only for cases of nonsestamibi-positive adenoma or multiple gland disease. These new technologies may lessen the surgeon's dependence on immediate pathologic analysis.
Summary of cost-effectiveness results of parathyroid tissue evaluation.
The concurrent use of intraoperative cytology for tissue identification in parathyroid exploratory surgery has been discussed by several investigators who previously have documented both the advantages and limitations of intraoperative cytological examination. 6 We were able to demonstrate that simultaneous cytological examination performed corroborated the histological tissue diagnosis in all cases. The cytological examination was always performed before the FS examination because of the faster processing time for the touch and smear preparations.
Given our findings, we concur with prior investigators that the concurrent use of cytological examination in tissue identification is a useful adjunct to the FS examination. 3,6 It should be noted, however, that the artifactual stripping of cytoplasm from the nucleus during smear or imprint preparation may result in the misinterpretation of parathyroid cells as lymphoid tissue cells. Also, a hypocellular cytology specimen is often nondiagnostic or even misleading. Therefore, although intraoperative cytology is recommended as an ancillary or adjunct method, we cannot advocate that it replace FS diagnosis as the gold standard in the intraoperative diagnosis of parathyroid tissue. An experienced pathologist is essential for the interpretation of cytology and FS.
The advent of the QPTH assay has irrefutably changed the face of the parathyroid exploratory surgery. QPTH is used by many surgeons at large centers as a means to determine the completeness of pathologic parathyroid gland removal and likelihood of achieving a surgical cure. The impact of the assay has been a reported decrease in operative failure and a subsequent decrease in FS requests. 5,9–12 Irvin 12 and Perrier et al 13 previously have stated that the QPTH assay had a 10-minute and 15-minute turnaround time, respectively. At the HMC, the turnaround time was at least 35 minutes. Consequently we were able to perform all our intraoperative cytological examinations, and FS examinations before the QPTH result was reported in those cases in which it was used. As such, the gross identifications of parathyroid tissue in our study were unbiased by the QPTH result and in most cases relied solely on MIBI or on the gross morphological features of the tissue submitted.
Because the cost of performing the required QPTH assays at our institution was $28 and the cost of performing an intraoperative consult with both FS and cytologic examination was $347, it can be suggested from our study that the elimination of the FS diagnosis in parathyroid explorations could be cost effective. However, the potential cost of a repeat MIBI study and repeat parathyroidectomy is many times greater than the cost of an intraoperative FS consultation and must be borne in mind when evaluating the necessity for routine FS diagnosis in this setting. Not all cases of misdiagnosis of tissue on gross inspection would have resulted in surgical failure in cases in which QPTH was utilized. This would reduce the likelihood and costs of revision surgery when FS is not used to less than our reported 6% error rate on gross inspection alone. In 1-way sensitivity analysis in which specificity of GE was varied from 0 to 1, the GE approach became dominant (ie, less costly and more effective) for values of specificity of ≥60% (Fig 6).
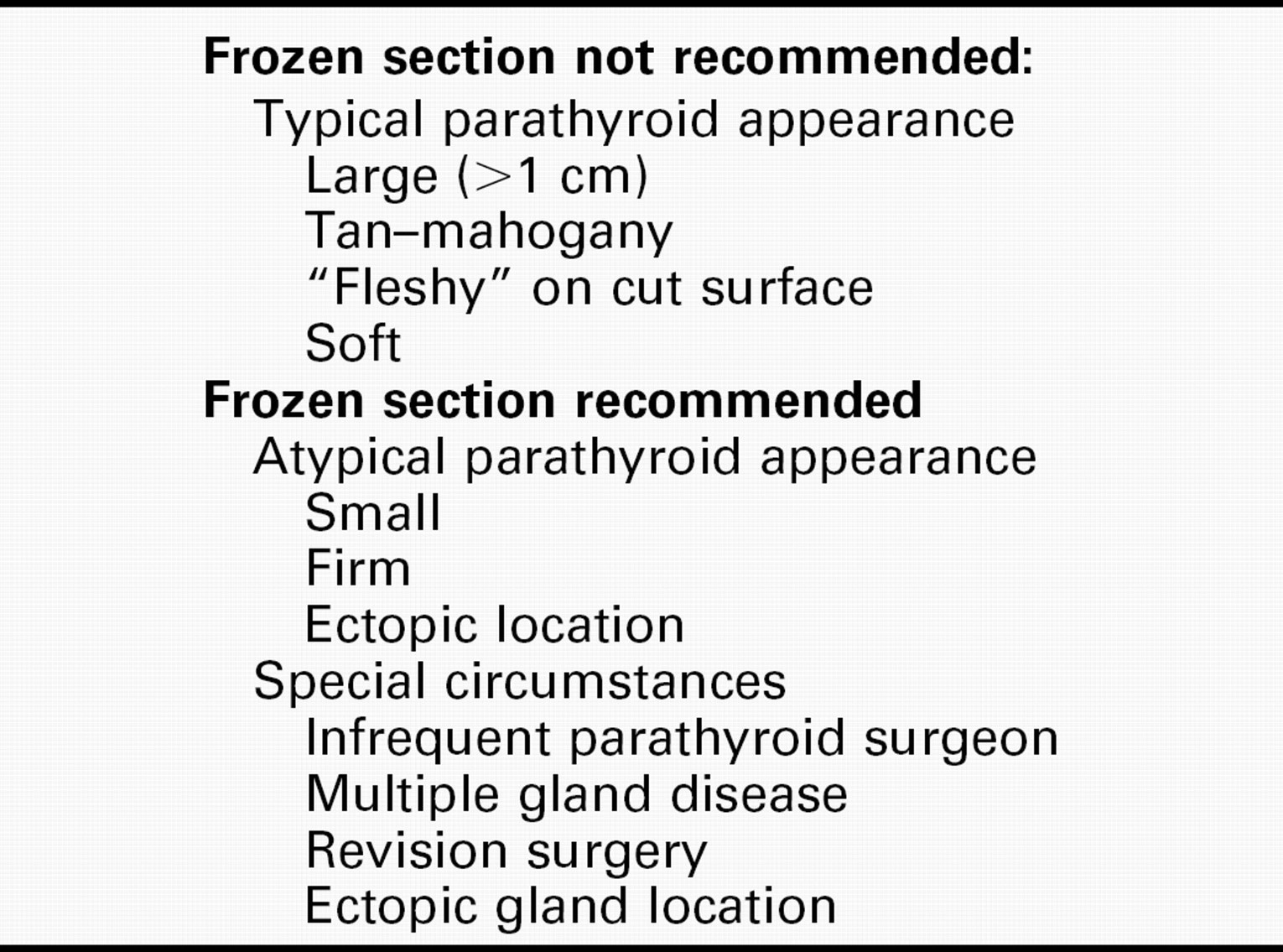
The following are our recommendations for FS use. The premise of this paper was a prospective analysis of a single experienced parathyroid surgeon's ability to correctly identify parathyroid tissue on GE. These observations were compared with standards such as a pathologist's gross inspection, cytology, and FS. These findings should not be extrapolated to mean that FS is neither useful or necessary in parathyroid surgery. Situations that warrant the judicious use of FS would include the following: the infrequent parathyroid surgeon, cases of multiple gland disease (primary, secondary, or tertiary hyperparathyroidism), ectopic glands, reoperant necks, and otherwise technically difficult primary surgeries (table 3). Small specimens (biopsies as opposed to complete excisions) were more challenging to diagnose by GE.
CONCLUSION
Given the concordance rate between the surgeon's and pathologist's opinion on GE of tissue removed at parathyroid exploration, our study supports the proposition that an experienced parathyroid surgeon need not routinely request FS examination for tissue confirmation, especially with the use of MIBI and concomitant QPTH assays. Cost analysis of our data confirms this assertion. However, when compared with FS confirmation, there was a 6% error rate on GE alone, which could lead to repeat and often difficult parathyroidectomy procedures if FS were not performed in these cases. Our findings also emphasize the importance of cytology imprints and smears as useful adjuncts in the FS diagnosis of parathyroid tissue. The experienced parathyroid surgeon's decision to omit intraoperative FS examination for tissue confirmation in parathyroid explorations, especially when guided by MIBI and intraoperative parathyroid hormone monitoring, must be balanced against the potential cost implications for a repeat parathyroidectomy procedure. However, we encourage the use of FS for casual parathyroid surgeons. We also advocate the liberal use of FS in cases of multiple gland disease, ectopic glands, reoperation, and difficult primary surgeries. Future investigations with a larger sample and separation of single versus multiple gland specimens may shed further light on our findings. 10
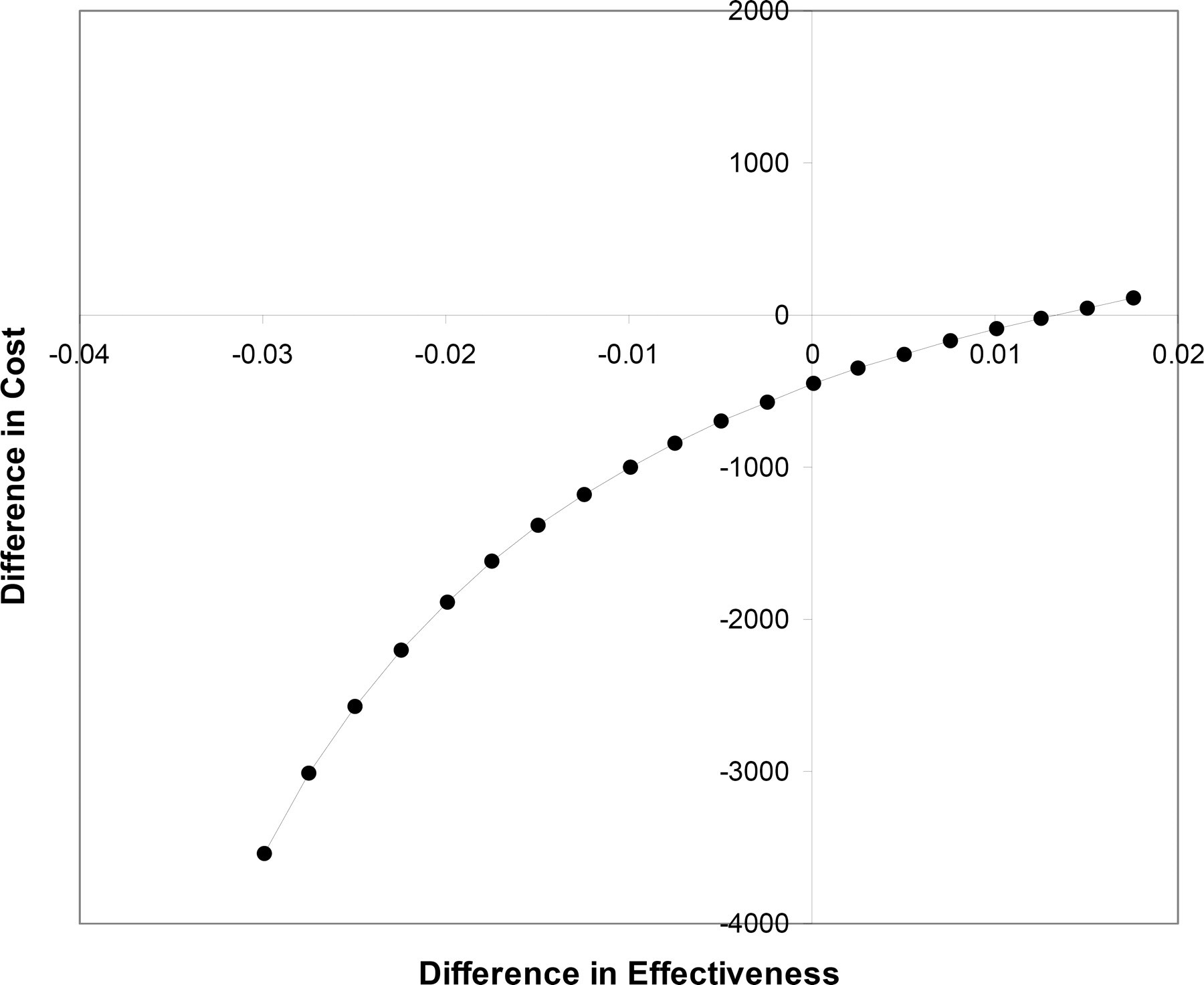
One-way sensitivity analysis of the specificity of FS.
Recommendations for frozen-section use in parathyroid surgery