
Abstract
Bone marrow transplantation (BMT) is an important therapeutic strategy in the management of selected malignant and nonmalignant hematological disorders. In 24% to 40% of cases, 1 , 2 BMT is associated with several systemic complications that require admission to an intensive care unit (ICU). The outcome for such patients is generally poor, especially those who require mechanical ventilation. Survival rates have been reported to be less than 10%. 1 , 2
Tracheotomies are often performed in critically ill patients who need prolonged respiratory care. Open tracheotomy (OT) was, and is still considered, the gold standard surgical procedure. Percutaneous tracheotomy (PT) has been gaining popularity in the last two decades, especially for patients in the ICU. Several recently published studies have compared open versus percutaneous tracheotomy. 3 , 4
Most of these studies have found that the complication rate was similar for both methods, with PT tending to have a lower rate. Since PT does not have to be performed in the operating room, it has the important advantage of eliminating movement of ICU patients, an act that can lead to mishaps. 5 Thrombocytopenia or coagulopathy is one contraindication to PT. Unfortunately, most BMT patients have severe thrombocytopenia and coagulopathy. Additionally, those patients frequently suffer from renal and hepatic failure, 6 conditions that pose a surgical challenge. The purpose of this study was to evaluate the safety and efficacy of PT in mechanically ventilated BMT patients with severe thrombocytopenia.
Materials and Methods
Between January 2000 and June 2003, 275 PTs were performed at Rambam Medical Center. Of these, 26 were performed in the ICU of the BMT department. Demographics, primary disease, the cause for mechanical ventilation, co-morbid conditions, immediate and delayed complications of PT, and decannulation were recorded. Laboratory analysis included complete blood count, renal function tests, and coagulation profile. Acute renal failure (ARF) was defined as a doubling of the baseline serum creatinine level. In our study, severe thrombocytopenia was defined as a platelet count less than 30,000 cells/mm 3 .
All patients received 6 units of platelets one hour prior to the procedure.
The procedure was performed under general anesthesia and the patients were intubated at the time of the procedure. An anesthesiologist was present to sedate and paralyze the patient and control the airway until the tracheotomy tube was secured in place. Capnography monitoring was used to insure the correct positioning of the canula. We used the Portex guide wire dilating forceps kit (Portex Ltd, Kent, UK). Neither intraoperative fiberoptic guidance nor bronchoscopy was used.
Major bleeding was defined as bleeding that required transfusion or surgical intervention. Minor bleeding was defined as bleeding that was managed by tight dressing without use of blood products.
Results
Twenty-six patients consisting of 16 males and 10 females underwent PT in the BMT department between January 2000 and June 2003. The mean average age of the patients was 46 ± 14.3 years. The indications for BMT were acute myeloid leukemia (AML) in 15 patients, lymphoma in 7, and multiple myeloma in 4 patients. All patients suffered from respiratory failure. The average intubation time prior to tracheotomy was 10.4 ± 2.2 days (range, 7-17 days). The predisposing conditions that led to intubation were acute respiratory distress syndrome (ARDS) in 14 patients, pneumonia (Aspergillus, aspiration, or CMV) in 7, and alveolar hemorrhage in 5 patients. Fifteen patients (57%) suffered from acute renal failure. Of these 14 underwent continuous venovenous hemodialysis (Prisma, Gambro AB, Stockholm, Sweden) and received anticoagulation therapy. The mean platelet count prior to PT was 14,300/mm 3 ± 5500 (range, 6000-30,000/mm 3 ) and mean hemoglobin concentration was 10.4 g/dL ± 1 (range, 8-12 g/dL). Post-transfusion platelet count was not reported.
The mean international normalized ratio (INR) was 1.1 ± 0.2 and mean partial thromboplastin time (PTT) was 45 ± 9 seconds (Table 1).
One patient developed moderate bleeding during the percutaneous procedure. After the procedure was ceased, the patient was transferred to the operating room. During open tracheotomy, a bleeding vessel from the thyroid gland was located and sutured. This patient had a normal INR and an elongated PTT of 55 seconds due to heparin therapy. All other 25 procedures were completed successfully in a mean time of 10.2 ± 3.3 minutes.
Complications included minor bleeding that developed within 24 hours after the procedure in 4 patients. Three of them had a prolonged PTT due to heparin therapy and the other one had a normal coagulation profile. These patients were treated conservatively by tight dressing with Hexaca pron (Teva Ltd, Netanya, Israel) around the canula. Since they were hemodynamically stable, they did not require any blood products. All bleeding stopped during the first 24 hours postoperatively. No other immediate or delayed complications were encountered.
Patient characteristics
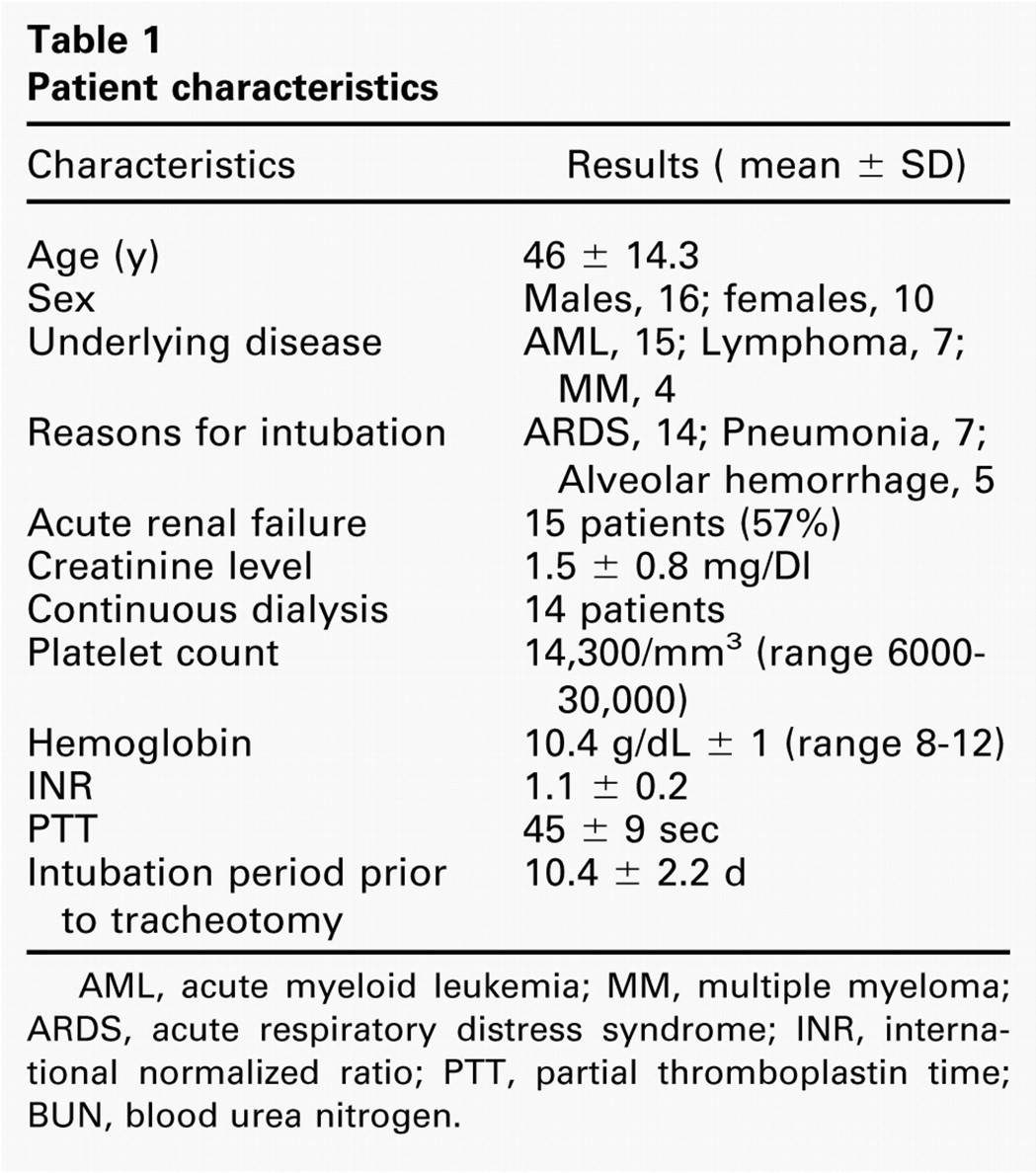
AML, acute myeloid leukemia; MM, multiple myeloma; ARDS, acute respiratory distress syndrome; INR, international normalized ratio; PTT, partial thromboplastin time; BUN, blood urea nitrogen.
Twenty-one patients died of their underlying diseases, usually due to multiorgan failure or sepsis unrelated to the tracheotomy. The mean time between PT and death was 12.4 days. Five patients survived, and they were decannulated after a mean time of 21 days. None of the survivors had acute renal failure
Discussion
Tracheotomy is one of the most frequently performed surgical procedures in critically ill patients. 7 Although PT has been performed for the past two decades, a considerable resistance to its acceptance among otolaryngologists persists. This resistance probably arose because the procedure is performed in a relatively blind fashion.
Nevertheless, the technique has numerous advantages. It can easily be applied at bedside by an appropriately trained surgeon. 8 During the procedure less dissection and tissue trauma occurs, thereby lessening possible hemorrhage. 9 , 10 Another reason for less bleeding is probably due to the tight fit of the tracheotomy canula to the surgical tract, leading to a tamponade of the small cervical vessels. 4 Additionally, PT is cheaper and less time-consuming than open tracheotomy. 10 , 11 The procedure can be performed at bedside, thus precluding the need to transport critically ill patients who require intensive monitoring. Smith et al 5 prospectively analyzed 125 patient transports from the ICU and found that one-third were associated with at least one mishap, ranging in severity from telemetry lead failure to vasoactive drug infusion disconnection.
The main disadvantage of PT is the blind manner of the procedure that can lead to paratracheal insertion. A large meta-analysis done by Dulguerov et al 4 found that perioperative complications are higher in the PT when compared to OT. Most of the complications resulted from paratracheal insertion or false passage of the canula. Van Heurn et al 12 performed histopathologic examination on the tracheas of 12 patients who underwent autopsies after PT and found that the puncture site of the trachea varied from the cricoid cartilage to below the third tracheal ring. Massick et al 13 reported a significantly increased postoperative complication incidence with the PT technique as compared to the open technique. The increase was attributed mainly to the inability to replace a displaced tracheotomy tube. They postulated that the increased risk of delayed airway loss could be directly attributed to the narrow dilated tract and the lack of a formal stoma. Others have suggested that the safety of the procedure could be enhanced by using fiberoptic tracheoscopy during the procedure. 14 Tracheoscopy will confirm the puncture site and the site the guide wire was inserted. However, there is no evidence to support a reduction in complications with the use of a bronchoscope. 15 Moreover, tracheoscopy, which is time consuming, can result in occult hypercarbia, respiratory acidosis, and hypoventilation. It should therefore be avoided in patients with raised intracranial pressure. 16 Capnography monitoring or ultrasonic guidance could be suitable alternatives to tracheoscopy. 17 , 18 Mallick et al compared capnography and tracheoscopy for percutaneous tracheotomy and found no difference in the complication rate or procedure success. 17
Although some disagreement about the contraindications for PT exist, the absolute ones are emergency tracheotomy, age younger than 12 years, positive end-expiratory pressure greater than 20 cm H2O, occluding thyroid mass over the tracheotomy site, and a palpable blood vessel over the tracheotomy site. 11 Relative contraindications are obesity, severe thrombocytopenia (platelet count <40,000/mm3), inability to identify the proper landmarks, and limited ability of the patient to extend the cervical spine.
The number of studies that have evaluated patients with thrombocytopenia who require tracheotomy is sparse. Blot et al 19 reported on 26 patients with thrombocytopenia and neutropenia who underwent open tracheotomy. They had a mean platelet count of 43,000/ mm 3 . No significant bleeding complications were reported. Beiderlinden et al 15 reported that of 133 patients who underwent PT, 18 had thrombocytopenia (<50,000/ mm3). None of the reports commented on the safety and complication rate of PT in patients with thrombocytopenia.
Recently, Kluge et al 20 reported on 42 patients with a mean platelet count of 26,000/mm 3 who underwent PT. All patients received from 6 to 12 units of platelets before the procedure. All procedures were completed without complication. Thus, the authors concluded that PT is safe in patients with thrombocytopenia as long as they receive a platelet transfusion prior to the procedure.
In our series, the patients had severe thrombocytopenia (mean, 14,300/mm 3 ) and mild coagulopathy. Only 1/26 patients (3.8%) suffered from major bleeding during the procedure. The patient underwent open tracheotomy in the operating room to control the bleeding. This patient had received heparin due to continuous hemodialysis, a factor that probably contributed to the bleeding episode. All other 25 PTs were completed successfully. During the perioperative period, 4 patients developed minor bleeding that required conservative management with tight dressing around the canula and no additional blood products. All received platelets one hour before the PT to maximize their platelet count, which reduced bleeding.
The low incidence of bleeding episodes can probably be attributed to a smaller skin incision, less tissue dissection, and the tight fit of the canula which tamponades the blood vessels.
We consider it important, however, that we gained extensive experience with PT in patients with normal coagulation studies before attempting it in thrombocytopenic patients.
Only 20% of the patients survived. These results are comparable with the published data. 2 All 5 patients that survived were decannulated without any problems or longterm complications.
Conclusions
The data show that PT can be performed safely in patients with severe thrombocytopenia, provided the surgeon and anesthesiologist are experienced in the procedure, and platelets are given before surgery.