
Abstract
OBJECTIVES: To describe and evaluate the efficacy of frozen-section analysis of cortical bone margins in surgery of the craniofacial skeleton.
STUDY DESIGN: Retrospective analysis of a consecutive series of patients undergoing oncologic resection of various head and neck neoplasms with osseous involvement by the senior author (Y.D.) from 1998 to 2003.
RESULTS: Frozen-section analysis of cortical bone was performed in 38 patients. Adequate specimens for histological analysis were obtained in all patients. Frozen sections were positive in 21 of 22 patients with bone invasion on decalcified specimens. After validating our technique for frozen analysis of cortical bone in 13 patients, the method had a sensitivity of 89% and a specificity of 100% in 25 patients. Malignancies diagnosed on frozen cortical bone specimens included squamous cell carcinoma (15), mucoepidermoid carcinoma (3), and sarcoma (3). Frozen cortical margins altered the extent of bony resection in 8 patients.
CONCLUSION: A simple technique for analysis of cortical bone involvement by neoplasm is presented and reviewed. It allows for frozen-section analysis with standard equipment and appears to be a reliable method to evaluate bony margins intra-operatively.
EBM rating: C-4
A method of accurate frozen section analysis of cancellous mandibular bone was described by Forrest et al. 1 Curettage of mandibular bone marrow allowed assessment of adequacy of resection with standard frozen-section techniques. A method for intraoperative assessment of both cortical and cancellous bony margins was described by Weisberger et al. 2 Frozen-section analysis was performed after microwave decalcification of specimens. However, the technique is labor intensive, requires special equipment including a diamond band-saw, and takes several hours.
We present a simple technique that allows rapid intraoperative frozen-section analysis of cortical bone. This method allows standard processing and analysis of the tissue by the surgical pathologist.
METHODS
We performed a retrospective review of 38 patients evaluated with frozen-section analysis of cortical bone by the senior author (Y.D.) from 1998 to 2003. The study met the approval of the institutional review board. To validate the technique, the initial 13 patients with radiographic and clinical cortical mandibular involvement underwent frozen-section analysis of areas of suspected cortical bone invasion. The subsequent 25 patients underwent frozen-section analysis of cortical bony margins with the described technique. Charts were evaluated for adequacy of frozen specimens for histologic analysis, results of frozen analysis, and final pathologic result of decalcified specimens.
Surgical Technique
Following resection of the specimen, soft tissue and bony margins are obtained. A 4- to 5-mm sharpened, curved osteotome is used to obtain thin sections of the cortical bony margins. The osteotome can be used on both cortical and cancellous bone. The osteotome is directed parallel to the cut surface of the bone to produce thin bony sections (Fig 1). Cortical specimens should be thin enough to be translucent. The lower density of cancellous bone typically results in small, thin fragments of bone that are easily collected. The cortical bony margins are then processed by the surgical pathology department in the routine method used for soft-tissue frozen sections. A standard cryostat and microtome are used to prepare slides for staining. No decalcification or other special equipment is required. Standard hematoxylin and eosin staining is performed (Fig 2). Our pathologists have experienced no significant difficulties in reading these sections or in diagnosing neoplastic involvement (seen as neoplasm interspersed with small sections of bone) in this series of patients. No equipment failures such as cryotome damage occurred.
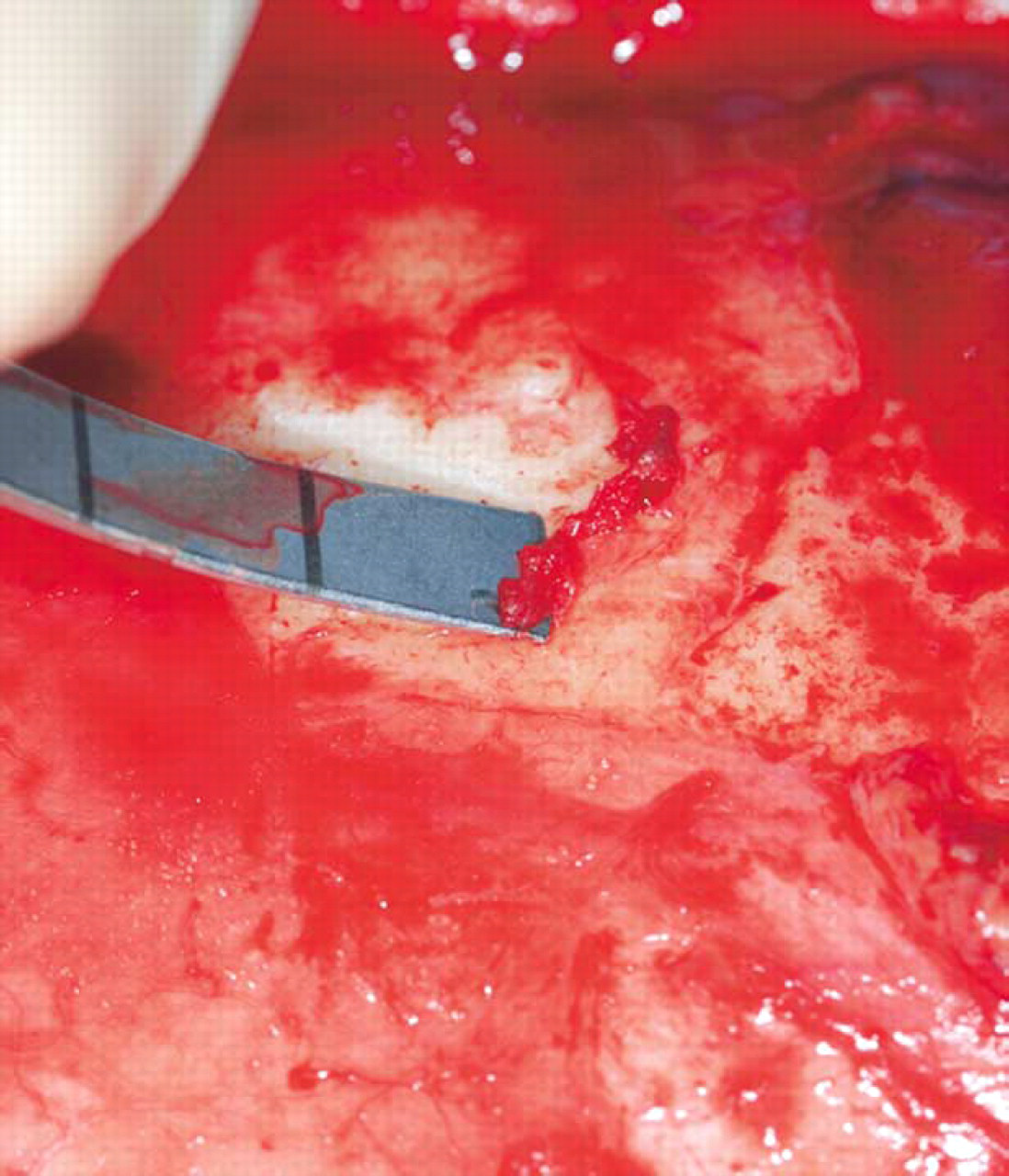
Intraoperative view demonstrating harvest technique. Note use of a sharp curved osteotome to facilitate osseous margin harvest.
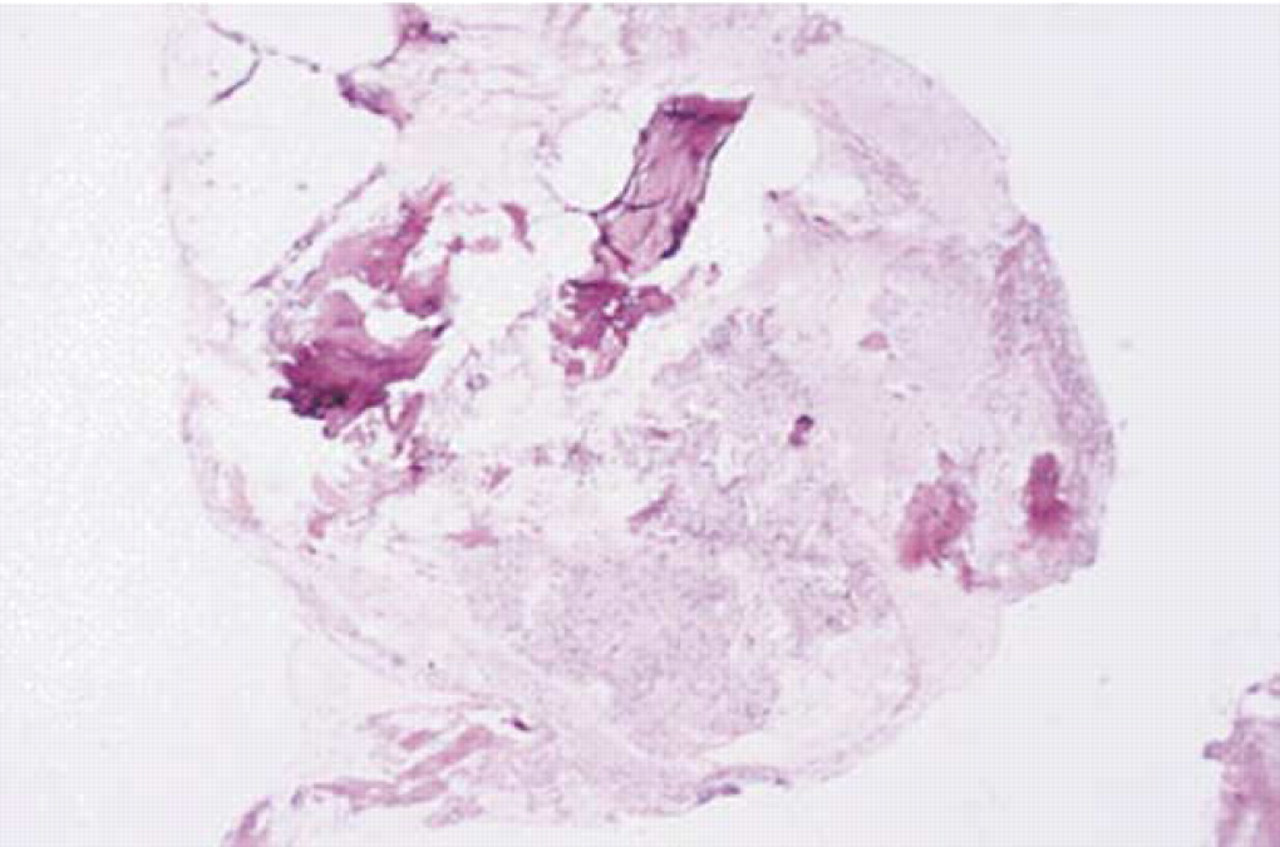
Frozen section (hematoxylin and eosin stain at 50×) demonstrating bony trabeculae with embedded tumor. The tumor cells form interlacing whorls in a distinct storiform fashion consistent with this patient's known sarcoma.
RESULTS
A total of 38 patients undergoing cortical bone frozen-section analysis was performed by the senior author (Y.D.) during extirpative surgery from 1998 to 2003. Cortical bone sites evaluated included 22 mandibular, 4 maxillary, and 12 calvarial margins. All 21 positive frozen sections were confirmed on subsequent final analysis to have cortical bone involvement by a variety of neoplasms (squamous cell carcinoma 15, sarcoma 3, mucoepidermoid carcinoma 3) and included all bony sites analyzed. The initial 13 positive sections in this series were done at the time of a planned resection of the clinically involved bone to validate our technique of evaluating cortical bone with frozen sections. All 13 initial specimens confirmed malignancy involving cortical bone. In the subsequent 25 patients, frozen-section analysis of cortical bone was positive in 8 patients, and the patients underwent more extensive resection. All patients were evaluated preoperatively with contrasted CT, and all patients with lesions adjacent to the mandible were evaluated with a panorex and/or mandible series. All 8 positive frozen specimens were confirmed with decalcified permanent specimens. One patient had negative cortical bone involvement on frozen-section analysis and positive involvement on final sections (squamous cell carcinoma). All 16 patients with no cortical bone involvement also had no evidence of such involvement at the time of frozen-section analysis. Excluding the initial 13 patients, sensitivity and specificity were thus 88.9% (8/9) and 100% (16/16), respectively.
DISCUSSION
Treatment of head and neck malignancies commonly requires resection of bony structures as part of the composite specimen. Obtaining margins negative for malignancy has a tremendous influence on local recurrence and survival. With the routine use of osseous free flaps for primary reconstruction of segmental mandibular defects, it is vital to prevent the situation of learning that bony margins are positive a week after a free flap has been inset. Physical examination and imaging studies are useful for evaluating the extent of tumor involvement.
However, microscopic disease is often not evident clinically or radiographically. 5,6 Approximately one-third of oral cavity squamous cell carcinomas with histological bone invasion will demonstrate no physical signs of invasion. 5,7 Prediction of the extent of bony involvement is more difficult in patients previously treated with radiation therapy. While non-irradiated mandibles typically have a single focus of cortical invasion that may subsequently spread, 50% of irradiated mandibles were found to have multifocal invasion of carcinoma by McGregor and MacDonald. 4
Preoperative radiographic studies are useful for evaluating for bone invasion. However, several studies have demonstrated a significant incidence of falsely negative imaging studies with bone invasion. Tsue et al reported that 50% of patients with floor of mouth carcinoma and no bone abnormalities on CT were found to have bone invasion on final pathology. 5 Plain radiographs were reported to have a 14% false negative rate with oral cavity squamous cell carcinoma. 8 Single positron emission computed tomography (SPECT) is a promising modality for accurately evaluating bone invasion by malignancy. In a prospective study of 38 patients with oromandibular cancer, Imola demonstrated an accuracy of 87% with SPECT scanning, compared to 71% with clinical examination, Panorex x-rays, and CT. 9
Intraoperative analysis of bony margins allows assessment for residual tumor. Techniques described for evaluating bony margins include curettage of cancellous mandible and microwave decalcification. Weisberger et al 2 described a method of intraoperative evaluation of bony margins after rapid microwave decalcification. The specimens are cut with a diamond-bladed band-saw and then require multiple episodes of microwaving in a mixture of formalin and hydrochloric acid for decalcification. Once decalcified, specimens are embedded in paraffin, cut, and stained. This technique obtained a 100% correlation with permanent specimens in 10 patients. Advantages include the ability to evaluate complete cross-sectional sections of bone. However, the method is labor intensive, requires experienced laboratory technicians and specialized equipment that is not found in most in hospital pathology suites, and takes 2.5 to 3 hours to complete analysis of the specimen. Forrest et al 1 reported a method of using a curette to obtain cancellous bone from the remaining mandibular stump. Specimens were processed in the standard fashion for frozen sections. In 16 patients with mandibular invasion by carcinoma, frozen-section analysis correctly predicted adequacy of resection in 32 (97%) of 33 margins. Permanent section results of the decalcified cancellous specimens completely correlated with the frozen-section analysis. 1
Frozen-section analysis of cortical and cancellous bone was reported to be highly accurate by Stevens and Palmer. 3 They performed frozen-section techniques using a standard cryostat and microtome on over 550 bone biopsies obtained by trocars or needles. Frozen-section analysis was reported as accurate for diagnosing a wide variety of pathologies including hyperparathyroidism, Paget's disease, osteoporosis, osteomalacia, and malignancies.
Our technique also supports the ability to perform frozen-section analysis of cortical bone with standard equipment. While Stevens and Palmer's technique is useful for transcutaneous evaluation of bone with needles or trocars, a sharpened osteotome provides a method of directly obtaining cortical bone specimens thin enough to be processed with a standard cryostat and microtome. Our technique provides a method to intraoperatively evaluate cortical and cancellous bony margins from a variety of head and neck sites. Forrest's technique was also found to be accurate; however, curettage only allows assessment of cancellous mandibular bony margins. 1
As we gained trust in this technique, we evaluated for cortical osseous margin control intraoperatively in the remaining 25 patients. After resection of clinically apparent tumor, 8 of 25 patients (32%) underwent wider excisions than planned preoperatively, because of positive frozen-section analysis. The single patient with negative frozen sections but positive final sections for carcinoma was noted to have a small focus of cortical bone involvement. No other intraoperative clinical findings or preoperative radiographic analysis (panorex and CT scanning) suggested this finding. This likely represented a sampling error as may be seen with all frozen sections. We found our technique of frozen analysis of cortical bone to be highly sensitive (89%, 8/9 patients) and specific (100%, 16/16 patients) with respect to decalcified permanent sections.
CONCLUSIONS
Obtaining negative surgical margins is a critical goal of oncologic surgery. Our technique provides a simple method for intraoperative evaluation of bony margins. By creating thin cortical bone specimens with an osteotome, standard frozen-section processing techniques may be utilized to assess cortical bone invasion by malignancy.