
Abstract
OBJECTIVES: In September, 2004, an Air Force otolaryngology team was deployed to Iraq as a member of the multispecialty head and neck team, which had historically consisted of neurosurgery, ophthalmology, and oral surgery. We examined our operative and outpatient experience to determine if otolaryngology would be a critical component of this new head and neck team.
STUDY DESIGN AND SETTING: Between September 7, 2004, and January 22, 2005, we collected data on all otolaryngology operative procedures and outpatient visits at the Air Force Theater Hospital at Balad Air Base, Iraq.
RESULTS: One hundred fifty-nine patients underwent 257 operative procedures with the 3 most common procedures being complex facial laceration repair, tracheostomy, and neck exploration for penetrating neck trauma. In the otolaryngology clinic, we examined and treated 529 patients from throughout the Middle East.
CONCLUSIONS: The otolaryngology team proved to be a critical component of the Air Force multispecialty head and neck team.
EBM rating: C-4
The highest level of care available in Iraq is located at the Army combat support hospital and the Air Force Theater Hospital. Since the outset of the war, a multispecialty head and neck team consisting of neurosurgeons, ophthalmologists, and oral surgeons has been caring for casualties at the combat support hospital. Several otolaryngologists, primarily from the Army, have been deployed to Iraq, but, to the best of our knowledge, otolaryngology was never a member of the multispecialty head and neck team and, consequently, the full spectrum of otolaryngologic equipment and services had not been available in the Iraqi theater of operations.
In the summer of 2004, the Air Force Surgeon General and his staff decided to deploy a fully equipped otolaryngology team to serve with the multispecialty head and neck team at the newly established Air Force Theater Hospital in Balad, Iraq. The hospital is located in the middle of the restive Sunni Triangle, 50 km north of Baghdad along the Tigris River. Previously, general trauma surgeons and an oral surgeon evaluated and treated the head and neck trauma patients at Balad Air Base. The Air Force readiness personnel tasked this new otolaryngology team with collecting all treatment data in an effort to determine if this team should continue as part of the multispecialty head and neck team.
MATERIALS AND METHODS
On September 2, 2004, the otolaryngology component of the head and neck team, consisting of 1 otolaryngologist and 1 otolaryngology technician, departed for Iraq. The team was accompanied by a full array of otolaryngology equipment: 2 operating microscopes, 2 headlights, craniofacial and maxillofacial plating systems with external fixation, electric drills and saws, rigid and flexible endoscopy equipment (including sinus endoscopes, nasopharyngoscopes, esophagoscopes, and bronchoscopes), pediatric airway equipment, nerve integrity monitor, portable audiometer, and full otologic, head and neck, plastic, and maxillofacial equipment sets. We collected patient data between September 7, 2004, and January 22, 2005. The study, including all accompanying figures, has been reviewed and approved through appropriate Air Force and hospital channels.
Patient data were collected over this 4.5-month period and separated into inpatient (surgical) and outpatient data. Inpatient data included patient name, age, military category (Army, Marine, Navy, Air Force, Iraqi National Guard/Police/Border Patrol, enemy prisoner of war, Iraqi civilian, coalition military, and coalition civilian), operative procedure(s), date of operation, intraoperative findings, and surgeons. Also, the postoperative condition and status of these patients were documented. Complex facial laceration repair was defined as a 2-layer closure of a facial laceration typically performed in the operating room. Finally, special attention was paid to the multiple mass casualties, including the Fallujah offensive, seen at the Air Force Theatre Hospital during this period.
The outpatient demographic data consisted of patient name, age, military category, presenting complaint, examination findings including audiometric results, diagnosis and treatment, and disposition (admit, return to duty, aerovacuation to Germany).
RESULTS
Between September 7, 2004, and January 22, 2005, 159 patients underwent 257 operative procedures by the otolaryngology team at the Air Force Theater Hospital at Balad Air Base, Iraq. The otolaryngology team scrubbed in on all 257 cases, often with the assistance of general trauma surgeons, neurosurgeons, oral surgeons, and ophthalmologists. The demographic data is shown in Table 1. Each patient had an average of 1.6 procedures performed in the operating room. During the first 2 months of deployment (October-November 2004), all patients operated on by the multispecialty head and neck team were tracked. Over this 2-month period, 170 patients had life/sight-saving surgery. The otolaryngologist was the busiest member of the head and neck team and was primary surgeon on 37% of these patients (63/170), followed by ophthalmology with 26% (44/170), neurosurgery with 22% (37/170), and oral surgery with 15% (26/170).
Demographics of patient visits
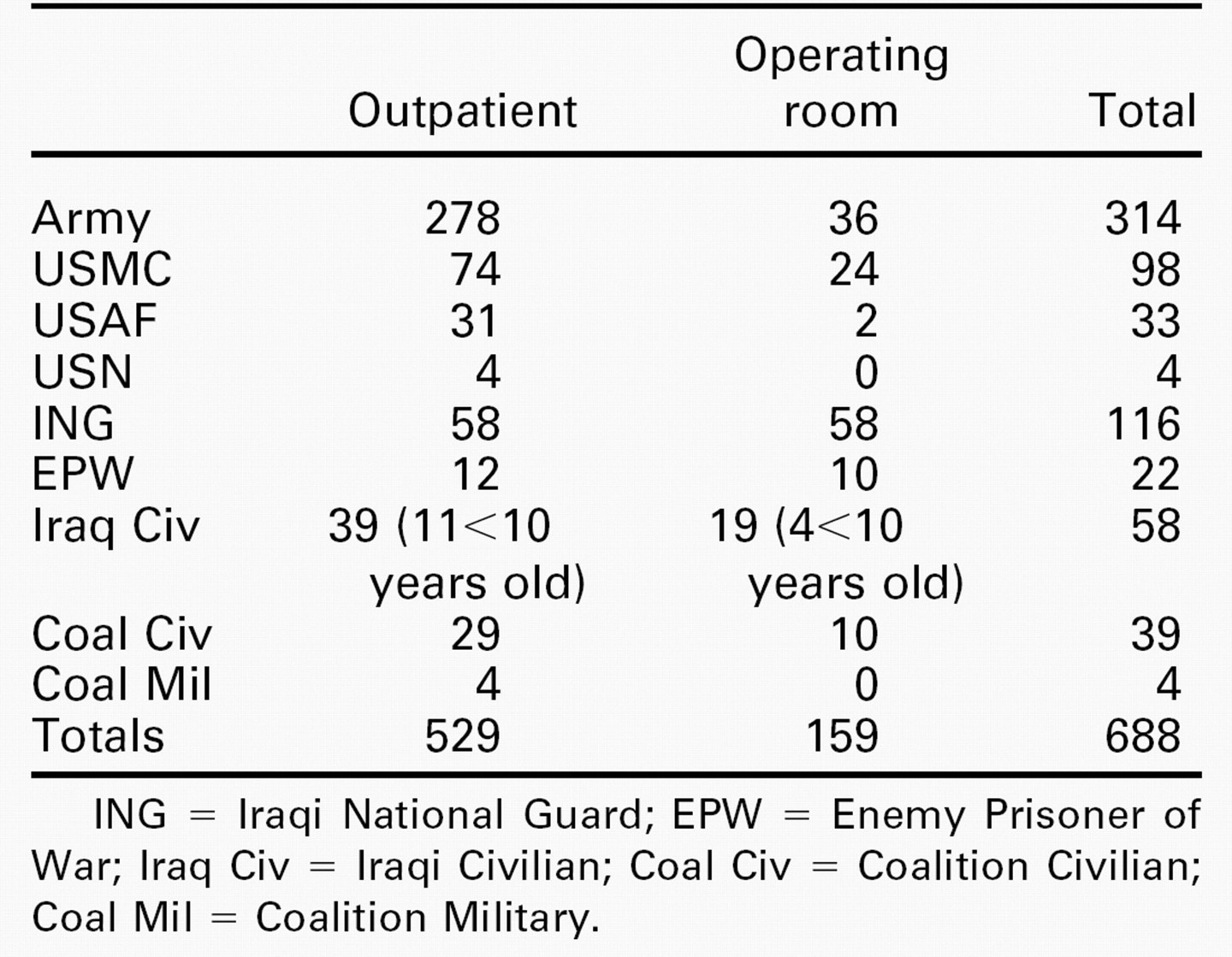
ING = Iraqi National Guard; EPW = Enemy Prisoner of War; Iraq Civ = Iraqi Civilian; Coal Civ = Coalition Civilian; Coal Mil = Coalition Military.
The most common otolaryngology procedures were complex facial laceration repair (70 patients), tracheotomy (53), neck exploration for penetrating neck trauma (27), direct rigid laryngoscopy (22), arch bars/intermaxillary fixation (15), control of facial bleeding (13), flexible bronchoscopy (10), flexible esophagoscopy (9), excision of head and neck mass (5), orbital enucleation (4), open reduction/internal fixation tripod fracture (4), open reduction/internal fixation mandible fracture (3), lateral canthotomy (3), and orbital exenteration (3). The 3 most commonly performed procedures were examined in more detail.
Complex facial lacerations were typically caused by improvised explosive devices (IED) consisting of artillery shells or other explosives buried in the ground or carried in a motor vehicle (vehicle-borne IED). These complex facial lacerations usually occurred with multiple other extremity and torso injuries and were often associated with extensive blood loss (Fig 1). Surgical treatment consisted of airway management, stopping the active bleeding, and then restoring the tissue/boney integrity of the injury (Fig 2).

Close-range high-velocity gunshot wound.
The second most common procedure performed was tracheostomy, a procedure that was subdivided into emergency and elective airway surgeries. Four emergency/urgent airway surgeries were performed (Fig 3). Forty-nine elective tracheostomies were performed, typically for United States troops with major head and neck trauma, pending aerovacuation, and for Iraqis who were ventilator dependent. Lastly, the otolaryngology team intubated 3 patients after failed attempts by other services.

Wound in Figure 2 after closure/intermaxillary fixation.
The third most common procedure was neck exploration for penetrating neck trauma. Twenty-seven patients underwent neck exploration with a mortality of 4% (1/27). The location of the penetrating neck trauma was zone I in 6 cases, zone II in 20 cases, and zone III in 1 case. The incidence of major intraoperative pathology found on exploration in the operating room was 78% (21/27). The neck explorations were performed by an otolaryngologist and a trauma surgeon who would perform vascular grafts if indicated. The otolaryngology team participated in all neck explorations with the exception of 1 additional neck exploration that occurred while the otolaryngologist was escorting a critically ill patient to Germany. All patients with penetrating neck trauma were treated with perioperative antibiotics, typically intravenous clindamycin.
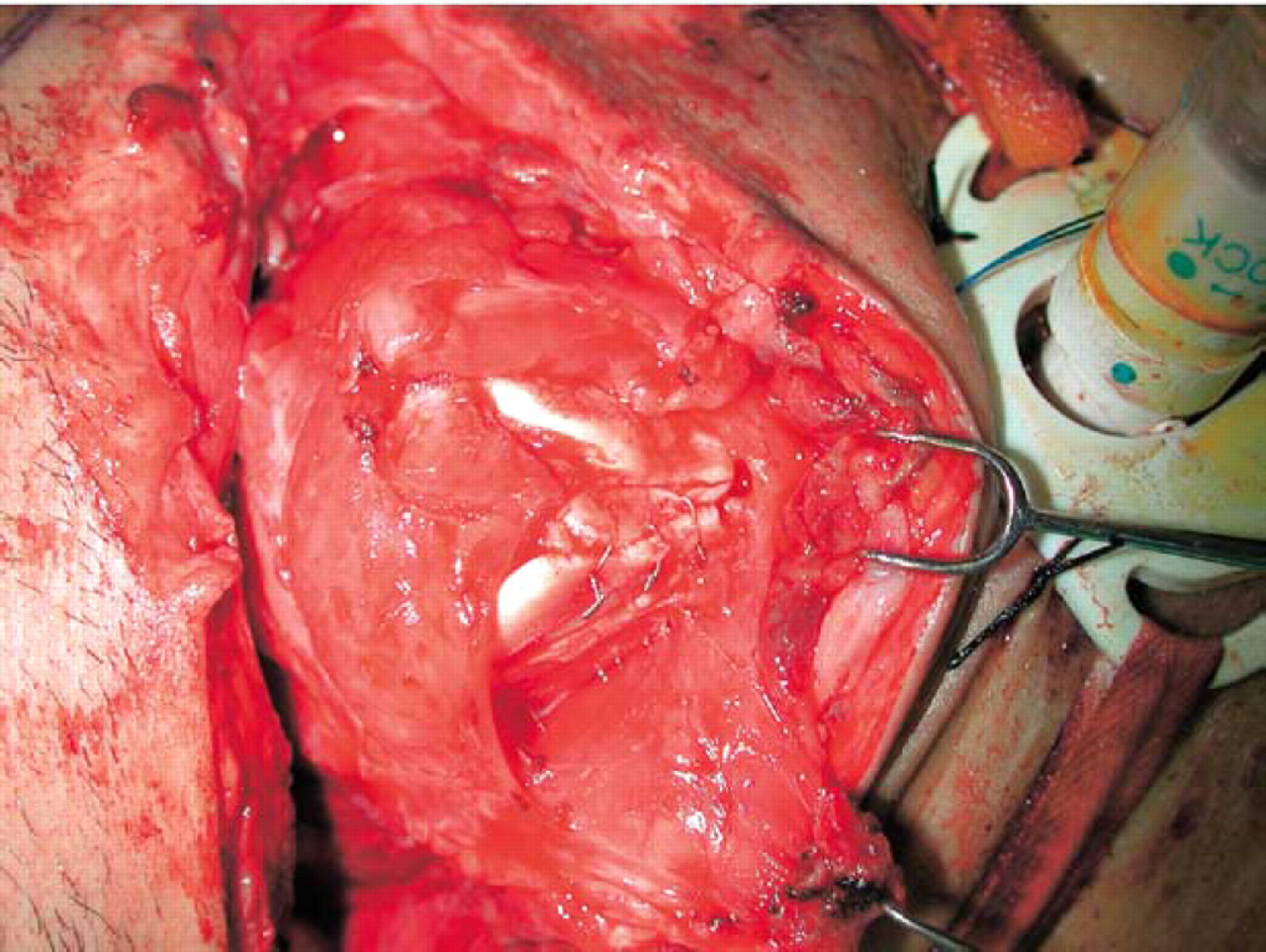
We explored six patients with zone I trauma, and the incidence of major intraoperative pathology was 100% (Table 2). There was no operative mortality (0/6). One patient had primary repair of a subclavian vein injury. We explored 20 patients with zone II trauma with an incidence of major intraoperative pathology of 70% (Table 2). One patient had an autologous sapheneous vein interposition graft for a common carotid artery (CCA) laceration (Fig 4), whereas a second patient had primary repair of a small opening in the CCA where a cordis had been placed. Patients with zone II injuries had a mortality of 5% (1/20). The patient who died had emergent ligation of the common carotid artery, internal jugular vein, and vertebral artery at a forward location. We reexplored the patient who arrived at our hospital with active bleeding. He died of a cerebellar stroke 2 days postoperatively. Finally, we explored 1 patient with zone III penetrating trauma and emergently ligated the internal carotid artery (ICA) and the external carotid artery (ECA) at the skull base. He survived postoperatively. Two additional patients with zone III penetrating neck trauma were completely asymptomatic and were noted to have partial and complete occlusion of the internal carotid artery on computed tomography angiography. These patients were observed without neck exploration and had no complications. Also, 2 patients had exploration of posterior neck penetrating trauma to control muscle bleeding.
We recorded 529 outpatient visits at the otolaryngology clinic. The demographic data is shown in Table 1. The 10 most common outpatient diagnoses were hearing loss after acoustic trauma (59), superficial shrapnel wounds with simple 1-layer repair or observation (53), tympanic membrane perforation (47), chronic (nontraumatic) otitis media (46), otitis externa (30), blunt head and neck trauma (26), parotid/neck masses (25), sinusitis (15), facial abscess (14), and chronic (nontraumatic) hearing loss (13). It should be noted that these numbers represent outpatient visits and not patients. Consequently, the outpatient visits would exceed the patient number because the typical patient with hearing loss or tympanic membrane perforation would have more than 1 outpatient visit for serial audiometry and examination of the eardrum.
Several mass casualties occurred during our deployment to Iraq. The busiest mass casualty occurred during the Fallujah offensive between November 8 and November 18, 2004. During this 10-day period, 381 combat injured personnel were admitted to our hospital, including 52 patients admitted on November 9, 2004. The otolaryngology service performed 34 head and neck procedures on 26 patients during this mass casualty. The otolaryngology service also participated in many orthopedic and general surgical cases during this timeframe.
DISCUSSION
The key question that needed to be answered during this deployment was whether the otolaryngology team would enhance the capabilities of the multispecialty head and neck team that had been operating in Iraq for the previous 18 months. The multispecialty head and neck teams working in both American and British hospitals did not have an otolaryngologist as a member of these teams. 2

Emergent surgical airway.
Penetrating neck trauma
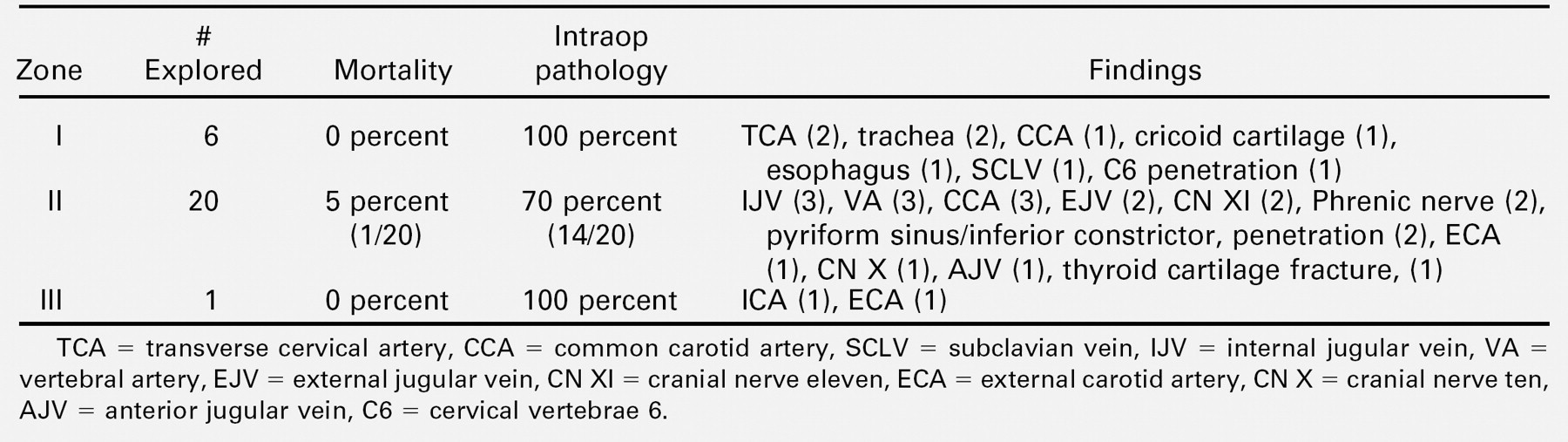
TCA = transverse cervical artery, CCA = common carotid artery, SCLV = subclavian vein, IJV = internal jugular vein, VA = vertebral artery, EJV = external jugular vein, CN XI = cranial nerve eleven, ECA = external carotid artery, CN X = cranial nerve ten, AJV = anterior jugular vein, C6 = cervical vertebrae 6.
Twenty-five percent of patients who were aerovacuated to Walter Reed Army Medical Center between March 1, 2003, and July 1, 2003, had combat injuries to the head and neck. 3 This high percentage of head and neck injuries exceeds that seen in previous wars. 4 Many factors account for the high percentage of head and neck trauma seen in OIF, primarily body armor. Body armor consists of a vest with ceramic plates that will stop high-velocity rifle bullets (AK-47) and shrapnel (Fig 5). The ceramic plates protect the torso and abdomen, whereas the remaining part of the body armor consists of a softer material that will stop low-velocity projectiles. 3 This softer material protects part of zone I of the neck, but the upper two thirds of the neck and face are unprotected. 3 The effectiveness of body armor in protecting the torso was shown when 10% of Marines wearing body armor presented with torso injuries, whereas 24% of Iraqis without body armor presented with torso injuries over the same period. 2,5 However, body armor has negligible impact on the incidence of head and neck injuries. Data from the forward surgical team showed that troops wearing body armor had a 19% incidence of head and neck injuries, whereas those without body armor had an incidence of 17%. 6 In previous conflicts, soldiers with head and neck trauma would commonly present with significant and often fatal injuries to the chest and abdomen. Thus, better protection of the torso has led to a higher incidence of operative head and neck trauma.
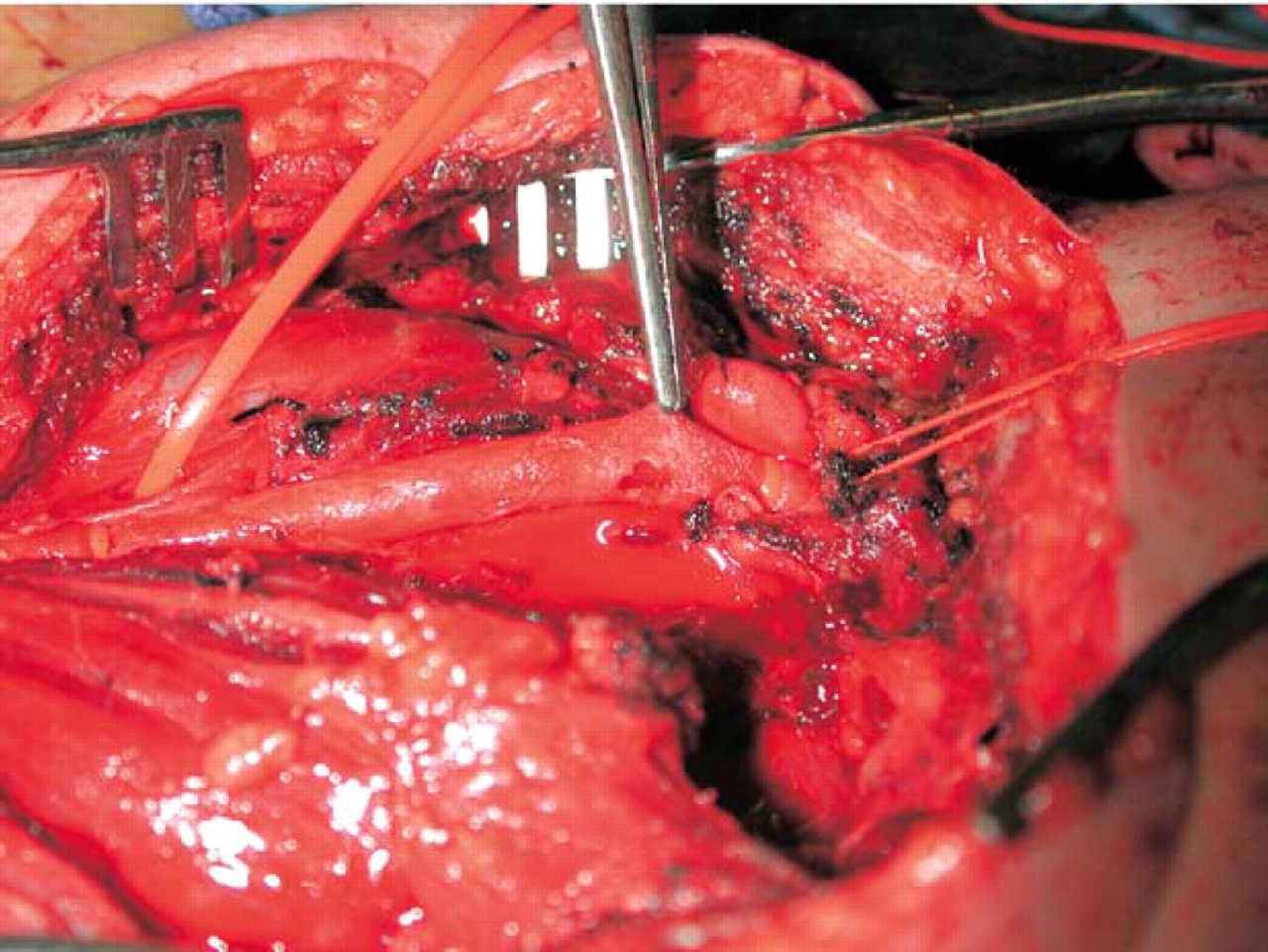
Common carotid artery perforation from IED.
The percentage of soldiers wounded in action in OIF who die from their wounds is exceedingly low. In World War II, 30% of those wounded in action died of their wounds. 1 In Vietnam, 24% of those wounded in action died of their wounds. 1 However, in OIF, only 10% of those wounded died of their wounds. 1 Despite the increasing lethality of weapons used in OIF, including massive IEDs, which often combine blunt, penetrating, and burn injuries, our soldiers have a significantly higher survival rate compared with previous conflicts. 1 Clearly, the presence of surgical subspecialists, including otolaryngologists, at theater hospitals enables the performance of definitive life-saving surgery, often within 1 hour of injury. The critical skills of acute airway management, upper airway endoscopy, and neck exploration enable the otolaryngologist to bring unique capabilities that maximize the care of the combat injured.
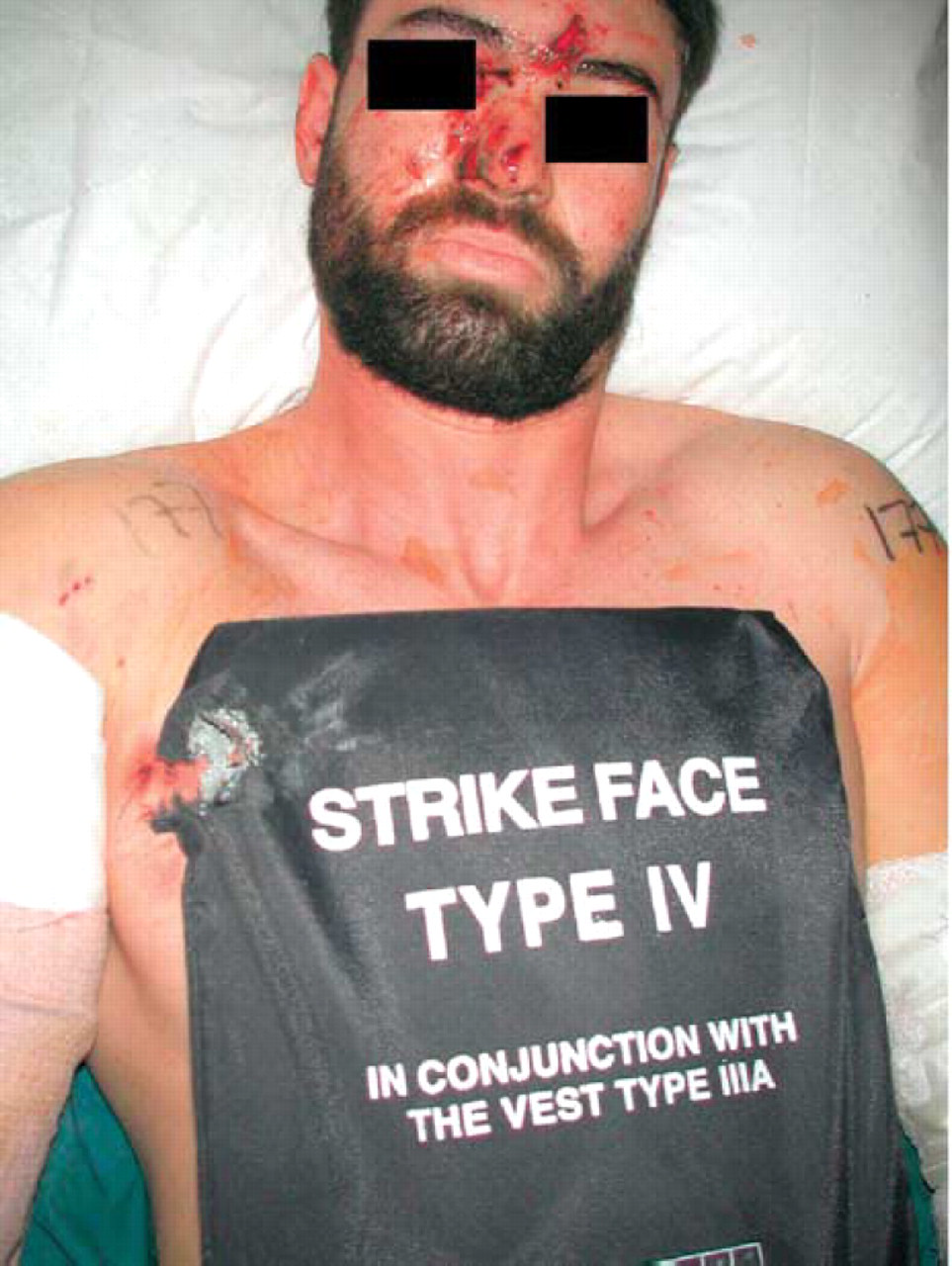
Body armor stopping high-velocity projectile over chest.
The unique skills of the otolaryngologist at a theater combat hospital are illustrated by several cases. The first case, a 32-year-old Army sergeant, walked into the emergency room from a helicopter during the Fallujah offensive with bright red blood pouring from his mouth and small puncture holes in zone II of his neck (Fig 6). He was taken to the operating room, a surgical airway obtained, and his neck was explored, showing no bleeding. Rigid direct laryngoscopy showed brisk bright red blood running from the pyriform sinus. The inferior constrictor was opened over this area, a 3-mm artery torn by a 1 mm × 2 mm metal shard was ligated, and all bleeding stopped. The second case was a 22-year-old Marine hit by an IED in zone III of the neck. While waiting in the intensive care unit, bright red blood began gushing from his neck wound. Manual pressure was applied, a tracheotomy performed, and the ICA and ECA ligated at the skull base after the mandible was subluxed and all cranial nerves preserved. The third case was a 21-year-old Iraqi National Guard soldier hit by an IED, who presented with a gaping wound in zone I of the neck. A 6-cm section of his trachea was macerated below ring 2, and his esophagus had a large perforation. The esophageal perforation was repaired, a median sternotomy performed, the inominate vein ligated, the clavicular heads and upper sternum resected, a formal stoma created in the upper chest, and the proximal trachea oversewn subglottically (Fig 7).
In addition to surgical subspecialists, several other factors account for the increase survival in OIF. The forward surgical teams who accompany the troops give immediate life-saving care. 1,5,6 The helicopter crews brave direct fire to rescue the wounded and bring them to medical care literally within minutes. 1,5 The critical care air-transport teams are flying intensive care units that rapidly bring critically ill patients to advanced medical facilities in Germany and the United States. During Vietnam, the mean travel time for wounded soldiers from the battlefield to the United States was 45 days, while the same trip during OIF takes only 4 days. 1 During our rotation at Balad, an airman was critically injured by a mortar attack and was on the operating table at Walter Reed Army Medical Center 36 hours after his injury occurred. 1

Zone II penetrating neck trauma with puncture lacerations.

Zone I penetrating neck trauma with formal stoma.
Several clinical pearls were evident from our operative experience. First, IEDs would often pepper our patients with multiple small and seemingly insignificant holes. However, it rapidly became apparent that small holes or nicks caused by high-velocity 1- to 3-mm projectiles were potentially lethal. We therefore coined the phrase “small hole equals big pathology.” Second, our high incidence of intraoperative pathology found that high-velocity penetrating neck trauma (PNT) mandates consideration of neck exploration in all patients, even if asymptomatic. These same data have been shown in previous conflicts with high-velocity PNT. 7 However, our dilemma was identifying which asymptomatic patients presenting with puncture neck wounds needed exploration. Hundreds of patients hit by IEDs were peppered with these seemingly innocuous wounds. Obviously, all symptomatic patients with abnormal physical examinations presenting with PNT would be taken immediately to the operating room for neck exploration. Asymptomatic patients with small puncture wounds would be examined with plain anteroposterior and lateral neck films to determine the depth of penetration of these minute metal fragments. If the fragments traveled deeply into the neck below the sternocleidomastoid muscle, computed tomography angiography was ordered to examine the carotid sheath. Computed tomography angiography was most useful in examining the carotid sheath at the skull base for asymptomatic zone III PNT because this is the least accessible zone of the neck hidden beneath the mandible. Also, upper aerodigestive endoscopy was critical in the examination and treatment of PNT. For example, the bleeding artery ligated deep within the inferior constrictor muscle in case number 1 (Fig 6) was localized using a rigid suction tube placed via direct laryngoscopy at the pyriform sinus bleeding site and palpated externally through the neck. Rigid direct laryngoscopy was critically important in the assessment and treatment of a traumatic laryngeal fracture (Fig 8). Esophagoscopy, both rigid and flexible, was critical for identifying occult esophageal injuries in PNT. Furthermore, as we are well aware, it all begins with the airway. Otolaryngology was instrumental in evaluating airways during the many mass casualties and assisting in acute airway management. Multiple patients presented with acute airway obstruction and needed emergency airway surgery or intubation after failed attempts by other services. Additionally, otolaryngology was instrumental in controlling exsanguinating hemorrhage from the head and neck. Several patients presented with potentially lethal hemorrhage from the scalp, face, nasopharynx, and oropharynx requiring up to 22 units of blood during resuscitation (Fig 3). The otolaryngologists controlled the massive hemorrhage with a combination of electrocautery, suture ligation, and direct packing. Lastly, all patients with high-velocity penetrating neck trauma were treated with perioperative clindamycin, and all wounds were drained with passive Penrose drains. The only neck infections treated at our hospital were PNT patients explored at forward facilities who had placement of closed-suction (Jackson-Pratt) drains and subsequently developed deep space neck infections.
Laryngeal fracture repair with 30-G wire.
The most common outpatient diagnosis was hearing loss secondary to acute acoustic trauma. Typically, these patients would be seen days to weeks to sometimes months after their injuries. All patients had audiometry performed. Those patients presenting with significant hearing loss would be placed in jobs without noise exposure or aerovacuated to Germany and followed with serial audiograms. Consideration was given to medical management such as oral steroids, but most outpatients presented weeks to months after injury and our use of medical management was infrequent. Also, extensive efforts were made to distribute the effective new Army hearing protective plugs, and thousands were distributed to units in the field.
Our observation was that the outpatient care of our soldiers in the field was exceedingly important. First, by treating the many common head and neck diseases seen, we were able to maximize the quality of life for these patients and maximize their effectiveness in the field. Second, we were able to safely and effectively treat many patients in theater who otherwise would have been aerovacuated to Germany for an otolaryngology consult. All 4 subspecialties comprising the head and neck team established outpatient clinics. This helped maintain unit strength and morale because these soldiers were extremely reluctant to leave their comrades. Third, we were able to identify early several potential head and neck tumors that needed advanced care in Germany and the United States. Lastly, we were able to have a positive impact on the Iraqi military patients, civilians, and enemy prisoners of war. By offering care that was difficult to find in the local medical system, we greatly improved the quality of life for these Iraqis. All wounded patients of every nationality and military affiliation were treated the same within our hospital.
The experience of mass casualty treatment is unique. The major role of otolaryngology in the acute mass casualty was clearly airway control and hemorrhage control. The otolaryngology team would move from patient to patient checking and managing airways with the surgeons, emergency room doctors, and anesthesiologists. Even though it is well known that the survival of critically ill trauma patients arriving with active cardiopulmonary resuscitation is less than 1%, our dedicated doctors attempted to save all patients. 8
CONCLUSION
The otolaryngology team proved to be a valuable and indispensable member of the multispecialty head and neck team deployed during OIF. Otolaryngologists possess the key airway skills, endoscopy skills, and neck exploration skills needed to maximize the quality of care of our wounded patients. Otolaryngologists also provide outpatient treatment, which further maximizes the quality of care for our patients and allows otolaryngologic consultation in theater, thus preventing many needless aerovacuations to Germany.