
Abstract
EBM rating: C-4
ESS involves dissection and removal of bone, inflamed nasal and sinus mucosal linings, and other soft tissue. Some bleeding is unavoidable in any EES procedure and, when excessive, may jeopardize the safe performance of surgery. Topical or injected vasoconstrictors, as well as other measures (such as hypotensive anesthesia), are usually used for minimizing the amount of intraoperative bleeding. However, because postoperative bleeding is common, many rhinologists have adopted nose packing or other hemostatic means as a routine measure for controlling this bleeding. Nasal packing causes pain, rhinorrhea, nasal obstruction, and inconvenience. Its removal is painful and may cause rebleeding. 4,5 Many of our own patients who had undergone ESS under local anesthesia complained that the removal of packing was more stressful than the surgery itself. Some patients stated that the inconvenience caused by the packing would prevent them from considering revision surgery if necessary.
Various absorbable materials have been proposed as substitutes for packing. These include fibrin glue (Quixil [Cros-seal], OMRIX biopharmaceuticals, Brussels, Belgium), 5 hyaluronic acid, 6 a specific gelatin-thrombin–based agent (FloSeal, Baxter International Inc, Deerfield, IL), 7 and tissue adhesives. However, although many of these materials have proved to be effective as hemostats, data regarding their effect on mucosal healing are equivocal. Both human and animal studies have raised concerns that these agents may be associated with increased scar tissue formation. 8 These materials are also quite expensive, and therefore cost-benefit analysis should be considered. The purpose of the current study was to assess the necessity of routine nose packing in ESS.
PATIENTS AND METHODS
The study was approved by the local internal review board and performed on 100 consecutive adult patients undergoing ESS by the senior author (RE) at Hadassah Medical Center. All patients signed an informed consent form and were scheduled to undergo the procedure under general or local anesthesia according to the standard preoperative assessment used in our department. Only patients with hemoglobin levels higher than 10 mg/dL, normal prothrombin, and normal partial thromboplastin times were eligible for surgery. Contrary to other studies, 4 no preoperative measures (ie, administration of systemic antibiotics or steroids) were used to reduce inflammation at the time of surgery. Immediate preoperative medication included 10 mg diazepam in cases of general anesthesia and 10 mg diazepam, 50 to 100 mg dolestine, and 25 mg promethazine in cases of local anesthesia. Intravenous midazolam was given after entering the operating room in local anesthesia cases. Patients undergoing ESS under general anesthesia were maintained according to the anesthesiologist's preference. A hypotensive technique was not used. In all cases, 2 mL 10% cocaine were applied topically by neurosurgical cotton pledgets for 10 minutes at the beginning of surgery. The lateral nasal wall was injected with 2% lidocaine with 1:100,000 epinephrine. A greater palatine foramen block was not used. Targeted surgery using cold instruments with/without a microdebrider was performed in accordance with the patient's pathology. Bipolar electrocautery was used only when a pulsatile bleeding artery was encountered or when partial inferior turbinectomy was performed. At the end of surgery the nose was rinsed with cold normal saline. Merocel packing or a hemostatic agent (microfibillar collagen or tranexamic acid) was used only when bleeding continued for more than 5 minutes after completion of surgery. Patients who did not require packing during the first 2 postoperative days were considered as “no-packing” cases, whereas patients who required immediate or delayed packing or the use of a hemostatic agent were considered “packing” cases. “Packing” versus “no packing” was analyzed with regard to demographic characteristics, medical history, previous surgeries, current surgical procedure, type of anesthesia, and amount of intraoperative bleeding. Statistical analysis was performed using a Fisher exact test. A P value of less than 0.05 was considered significant.
All patients remained hospitalized for 2 nights after surgery. They were instructed to sleep with their head elevated, to refrain from hot food and from blowing their nose, and to rinse their nose with normal saline and dexamethasone/neomycin drops. A single intramuscular injection of 1 mL betamethasone (2 mg short-acting + 5 mg long-acting drug per 1 mL) was administered postoperatively. Intravenous antibiotics were given for the duration of hospitalization. Manual clearing of blood clots and crusts was performed before discharge, at the first clinic visit (6 days after surgery), and subsequently as required.
RESULTS
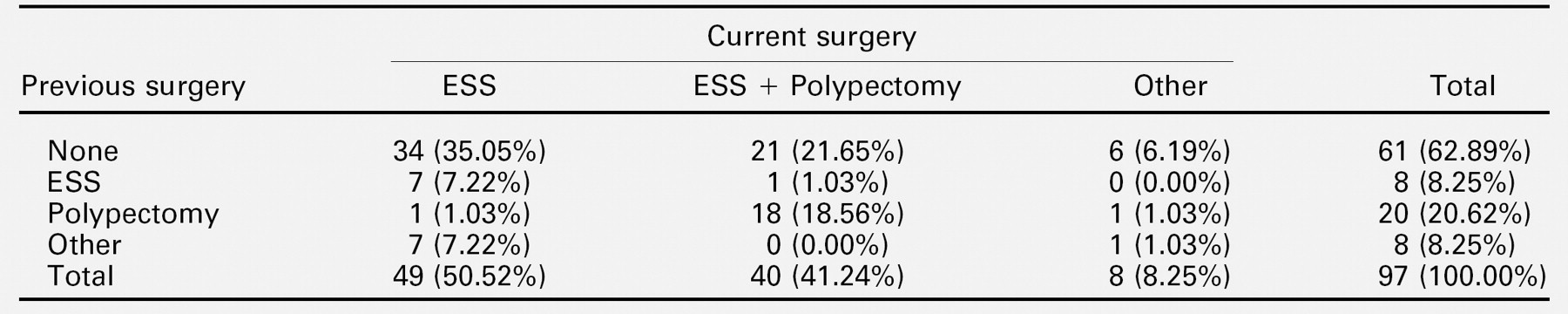
One hundred consecutive patients were analyzed. Three patients who required packing because of bolstering of mucosa (2 patients) and medialization of the middle turbinate (1 patient) were excluded from the study. The remaining 97 patients included 61 males and 36 females aged 16 to 86 years (mean 44 years). Seventeen patients (18%) were smokers, and 80 (82%) did not smoke on a regular basis. Medical history included hypertension in 10 patients, asthma and/or allergy in 26 patients, and other illnesses (such as carcinoma in other organs, rheumatoid arthritis, and so on) in 12 patients. Forty-nine patients (50%) did not report any other significant illnesses. Sixty-one patients (63%) denied any prior sinonasal surgery (Table 1). Thirty-six patients had undergone at least 1 other sinonasal procedure in the past: 8 underwent ESS, 20 nasal polypectomy, and 8 had other nasal surgery (such as septoplasty or turbinectomy). Only 6 of the 36 previously operated-on patients underwent the prior surgery at our institution. The current surgery was ESS for chronic sinusitis in 49 patients (50%), ESS associated with nasal polypectomy (unresponsive to medical treatment) in 40 patients (41%), and other endoscopic procedures (such as excision of a mucocele or a benign endonasal tumor) in 8 cases (9%). Fifty-four patients (56%) underwent the operation under general anesthesia (with or without the assistance of an image-guidance navigation system) and 43 (44%) under local anesthesia (with no image-guidance navigation system). No patient had to be converted from local to general anesthesia. There were no statistical significant differences between the general and the local anesthesia groups in relation to age, gender, past medical history, past or current operation, and smoking habits. Intraoperative blood loss was less than 30 mL in 82 patients (85%), 30 to 50 mL in 11 (11%), and more than 50 mL in 4 (4%). In 89 patients (92%), packing or a hemostatic agent was not used. In the other 8 patients, merocel packing was used in 6, microfibrillar collagen in 1, and tranexamic acid in 1 patient. No patient had postoperative bleeding complications, and no “no-packing” patient became a “packing” patient (ie, none of the “no-packing” patients required packing between the end of the surgical procedure and discharge from the hospital).
Current and previous surgery of the patients under study
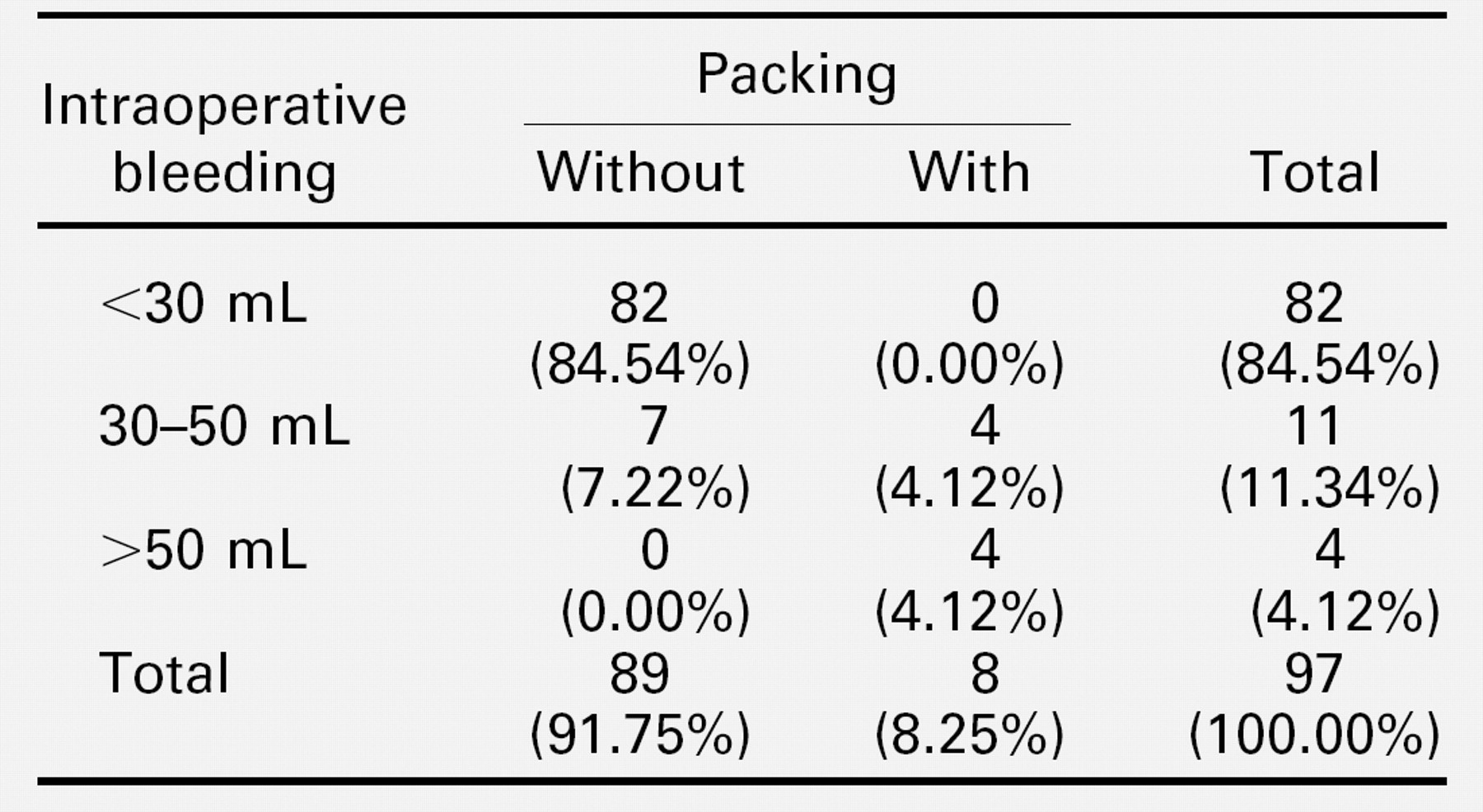
When comparing patients who required packing with those who did not, no statistical difference was found in relation to age (P = 0.7462), gender (P = 0.7061), comorbid conditions (P = 0.8456), previous sinonasal surgery (P = 0.4750), type of current surgery (P = 0.7357), and smoking habits (P = 0.1430). The prevalence of packing among patients who underwent ESS under general anesthesia (8/54) was significantly higher than the prevalence of packing in patients who underwent ESS under local anesthesia (0/43, P = 0.0082). In addition, the prevalence of packing among patients who bled more than 30 mL intra-operatively (8/15) was significantly higher than the prevalence of packing in patients who bled less than 30 mL (0/82, P < 0.001) (Table 2).
DISCUSSION
Packing after routine endonasal surgery is commonly practiced all over. This has led to the development of various packing materials, some of which not only apply pressure but also allow breathing or attempt to decrease postoperative adhesions. However, packing remains very uncomfortable and usually requires antibiotics to avoid the rare possibility of toxic shock syndrome. 4 In addition, removal of packing is often more stressful than the surgery itself and can cause rebleeding. On the other hand, hemostatic agents dissolve spontaneously and do not require antibiotic therapy or removal. However, studies have raised concerns about their biocompatability. 8 In addition, hemostatic agents are expensive, and their efficacy must be weighed against their cost.
Association between packing and amount of intraoperative bleeding
This study was initiated to assess the necessity to pack the nasal cavity after routine ESS. Patients were elected for surgery using the standard criteria used in our department in accordance with the conventional guidelines published in the literature. The operation was performed by means of our usual techniques with no special pre- and/or postoperative measures taken to minimize bleeding. We therefore assume that the results of our study are also valid for other institutions performing standard ESS.
It is the policy of our department to perform a preoperative evaluation of every surgical candidate (in rhinology as well as in other surgical fields) by measuring the complete blood count and by assessing the clotting mechanism. A patient with an abnormal blood test result is referred to a hematologist before surgery. We believe that, although costly, this approach prevents potential bleeding complications in certain cases. Indeed, clotting mechanism abnormalities were discovered in some of the surgical candidates in our department (Eliasher et al., 2005), although no bleeding tendency was apparent in their medical history. Thus, excessive bleeding was prevented by taking appropriate measures during surgery (eg, infusion of fresh frozen plasma).
In our department, we use cocaine and epinephrine on a routine basis in endonasal surgery. Contrary to a previous report, 9 we did not observe any adverse side effects that could jeopardize our patients. Mild tachycardia and slight blood pressure elevation were usually observed, but they resolved spontaneously in all cases. We believe that the strict local anesthesia technique used in both local and general anesthesia cases enables performance of relatively bloodless surgery and facilitates preventing postoperative bleeding, thus negating the need for packing.
Targeted surgery is routinely performed. We approach the diseased regions without touching healthy tissue. Minimizing tissue damage lessens the amount of intra- and postoperative bleeding. It also contributes to early healing with minimal postoperative adhesions.
Minimal tissue damage and creation of controlled synechiae between the middle turbinate and the nasal septum prevent the need to pack the nose to bolster the mucosa or to medialize the middle turbinate. Only 3 patients required packing because of these reasons, and all 3 were performed during the early stages of the study.
When comparing patients who required packing with those who did not, no statistical difference was found in relation to age, gender, comorbid conditions, previous sinonasal surgery, type of current surgery, and smoking habits. Statistically, more patients required packing when the operation was performed under general anesthesia (P = 0.0082) and when the intraoperative blood loss was greater than 30 mL (P < 0.001). In fact, these 2 parameters seem to be related because 11 out of the 15 patients who lost more than 30 mL of blood (including 3 out of the 4 patients who bled more than 50 mL) were operated on under general anesthesia. The fact that patients under local anesthesia bleed less than under general anesthesia has been previously described. 10 Other advantages of local anesthesia include less operating room time, less operating room staff, more safety when working in close proximity to the orbital wall or to the base of the skull, and avoidance of complications associated with general anesthesia. We believe that local anesthesia should be performed whenever possible. However, many patients require general anesthesia because of various reasons, and, in these cases, application of local vasoconstrictors along with a targeted meticulous operative technique can minimize bleeding.
In conclusion, the results of our study support the results of a previous publication 4 stating that most ESS procedures can be managed without packing and with no other hemostatic measures. Local anesthesia, application of local vasoconstrictors, and careful operative techniques minimize the need for nose packing, thus reducing patient discomfort, postoperative complications, and cost of surgery.