
Abstract
EBM rating: C-4
© 2006 American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc. All rights reserved.
The effective surgeon-patient relationship is founded on trust and maintained with the mutual flow of information. Communication of expected postoperative outcomes during both the short and long term, an explanation of potential risks and benefits of the proposed procedure, and the presentation of alternative therapies are key features of the informed consent process. 3,4
To date, the literature examining outcomes following ESS has focused exclusively on longer-term outcomes. 5,6 Validated instruments exploring general quality-of-life elements as well as disease-specific symptoms (Chronic Sinusitis Survey, Sinonasal Outcome Test, Rhinosinusitis Outcomes Measure, etc.) have proven reliable in delineating patient symptoms months or even years out from surgery. 7,8 There is a distinct paucity of data, however, on patient-centered outcomes during the recovery period following ESS. Knowledge of patient experiences during the early postoperative phase would augment the otolaryngologist's ability to effectively counsel patients preoperatively, enable the dispersion of unrealistic expectations, and generally enrich the informed consent process.
The objectives of this study were to determine patient expectations of the early postoperative phase following ESS, to compare these preoperative expectations to the actual symptoms experienced during the recovery period, and to identify variables that influence patient recovery.
MATERIALS AND METHODS
This was a prospective, longitudinal study. Consecutive patients about to undergo ESS for medically refractory chronic rhinosinusitis (CRS) between June 2004 and March 2005 at an academic medical center were invited to participate. Institutional Review Board (IRB) approval was obtained prior to initiation of the study.
We constructed an 11-item survey, using questions taken from validated surveys, including a recovery from anesthesia survey (Quality of Recovery Score) 9 and disease-specific rhinosinusitis outcomes instruments (such as the Rhinosinusitis Outcomes Measure, and the Sinonasal Outcomes Tool). 7,8 The survey created was designed to address elements important to the recovery from anesthesia, as well as sinonasal symptoms related to CRS and ESS. The variables examined were rated by patients on a Likert scale from 1 (symptom absent) to 5 (maximum severity), and included: frequency of epistaxis, nasal obstruction, nasal discharge, nausea and vomiting, fatigue, frustration, sadness, ability to fall and stay asleep, activity level, narcotic usage for facial pain, and level of overall health.
Before surgery, subjects completed 2 surveys: one establishing their baseline preoperative functioning and symptoms, and a second assessing what they expected to feel like on the evening of postoperative day (POD) #1. After surgery, patients then completed 3 additional surveys evaluating their recovery on POD #1, POD #7, and POD #14. A total of 5 survey datasets were thus obtained for all patients. Demographic data, work status, patient comorbidities, operative parameters, and preoperative CT stage were also recorded.
All patients underwent ESS under general anesthesia by the same attending surgeon (RS). Bilateral nasal packs (Merocel sinus packs, Medtronic ENT Surgical Products, Inc., Jacksonville, FL) were placed at the conclusion of each procedure, and patients were specifically instructed to remove the packing the next morning. Postoperatively, all patients were given standard prescriptions for a narcotic pain medication and a 7-day course of a cephalosporin (or macrolide if penicillin-allergic).
Patient characteristics were described using measures of central tendency (mean or median) and variability (standard deviation or range). Categorical level variables (ie, gender, septoplasty, previous ESS) were described using frequency (%). Statistically significant differences between groups were assessed using the independent samples t test or Pearson's χ 2 . The nonparametric equivalents Mann-Whitney U test and Wilcoxon Signed Ranks test were utilized when assumptions for parametric methods were not met. Determinations for statistically significant differences for the scores reported over the 4 time periods were assessed using the Friedman test. The survey tool was assessed for reliability and validity at each time interval using Cronbach's alpha. All analyses were considered statistically significant when P < 0.05. SPSS (version 11.5, Chicago IL) was utilized for all statistical analyses. Cronbach's alpha coefficients for the sinonasal domain ranged from 0.41 to 0.81 for the specified time points. Anesthesia-related domain coefficients ranged from 0.42 to 0.70.
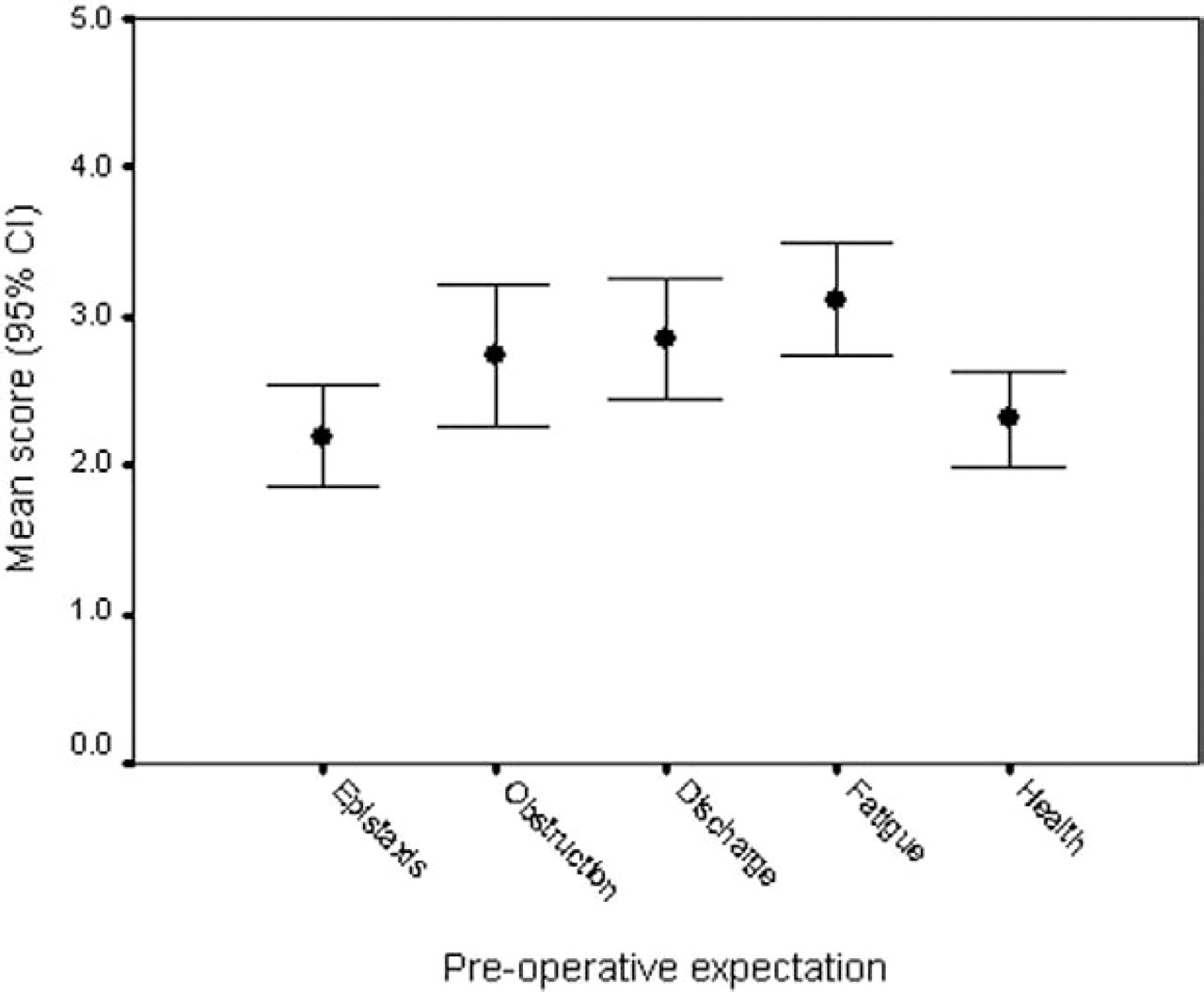
Patient (preoperative) expectations of sinonasal symptoms for the day after ESS, rated on a scale from 1 (symptom absent) to 5 (maximum severity).
RESULTS
Demographics
The study population consisted of 46 patients who completed all 5 of the necessary surveys. There were 24 women and 22 men with a mean age of 45 years (range, 17-74 years). Sixty-seven percent of patients were Caucasian, 23% were African American, and 10% did not provide ethnic background information. For the majority of patients (over 60%), this was their first sinus operation, while 17 patients (39%) had undergone a previous ESS. The mean CT stage (Harvard CT Staging System) 10 was 3.1, representative of bilateral disease with frontal and/or sphenoid sinus involvement. The mean operative time was 84.3 minutes and the average blood loss was 110 mL. There were no complications.
Preoperative Expectations of Recovery
Patients' preoperative expectations of their status on POD #1 are displayed in Figure 1 (sinonasal) and Figure 2 (anesthesia-related). Before undergoing surgery, the majority of patients expected their sinonasal symptoms on the day after surgery to include mild epistaxis, mild to moderate obstruction, and moderate discharge. The vast majority of patients (84%) expected to use narcotic pain medication once or twice per day on POD #1. Patients generally expected that their functional symptoms such as activity and fatigue would be moderately affected by the surgery. Psychosocial variables such as sadness, frustration, and sleep disturbance were expected to be minimally altered or unchanged after surgery. Patients anticipated their overall sense of health would be only mildly affected postoperatively.
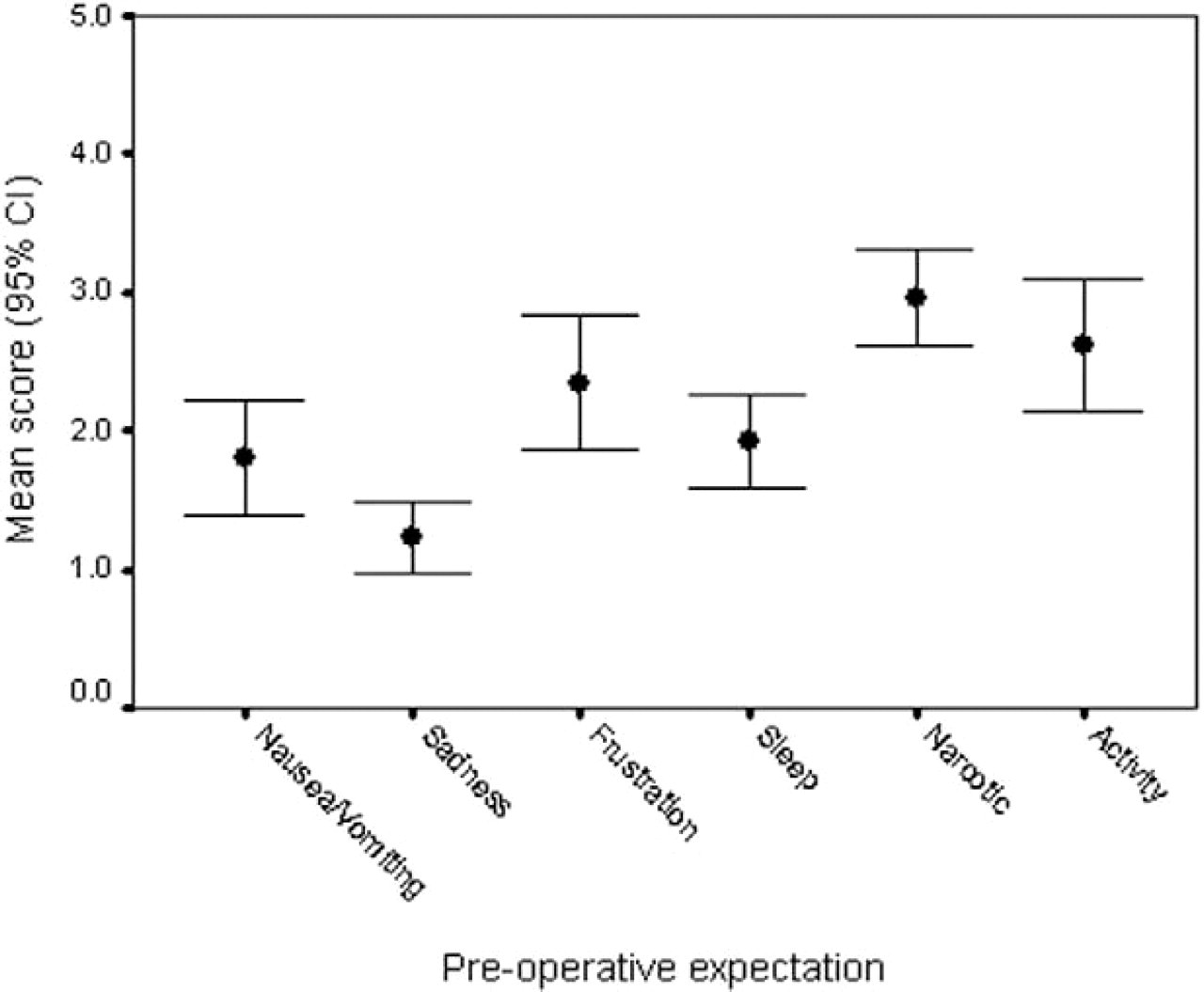
Patient expectations of POD #1 symptoms related to recovery from anesthesia.
We discovered that men and women differed slightly in their preoperative expectations. Specifically, men generally anticipated worse epistaxis postoperatively (P = 0.028) but better overall health (P = 0.023) for POD #1 when compared to women.
The expectations of patients with and without a history of previous ESS were very similar. When compared to the first-time surgery group (n = 29), patients who had undergone a previous ESS (n = 17) expected a greater level of activity (P = 0.023) and overall sense of health (P = 0.021) with less frustration (P = 0.025) postoperatively. There was no statistically significant difference in actual symptoms on POD #1 between the revision surgery cohort and the previously non-operated-upon group (P > 0.05).
Expectations vs Actual POD #1 Outcomes
To evaluate the concordance between preoperative expectations of the recovery period and the actual outcomes following surgery, patient responses were collapsed into 2 groups: those with no or minimal symptoms (rated 1 or 2 on a Likert scale from 1 to 5) and those with moderate to severe symptoms (rated 3, 4, or 5 out of 5). Only the responses from patients who had not undergone previous ESS (n = 29) were utilized for this portion of the analysis.
Individual patients were poor predictors of symptoms experienced on postoperative day #1, with the exception of sleep and overall health. On POD #1, patients who expected difficulty sleeping were more likely to experience this (P = 0.017.), and similarly, those who anticipated poorer overall health actually rated their overall sense of health as moderately to severely diminished (P = 0.028).
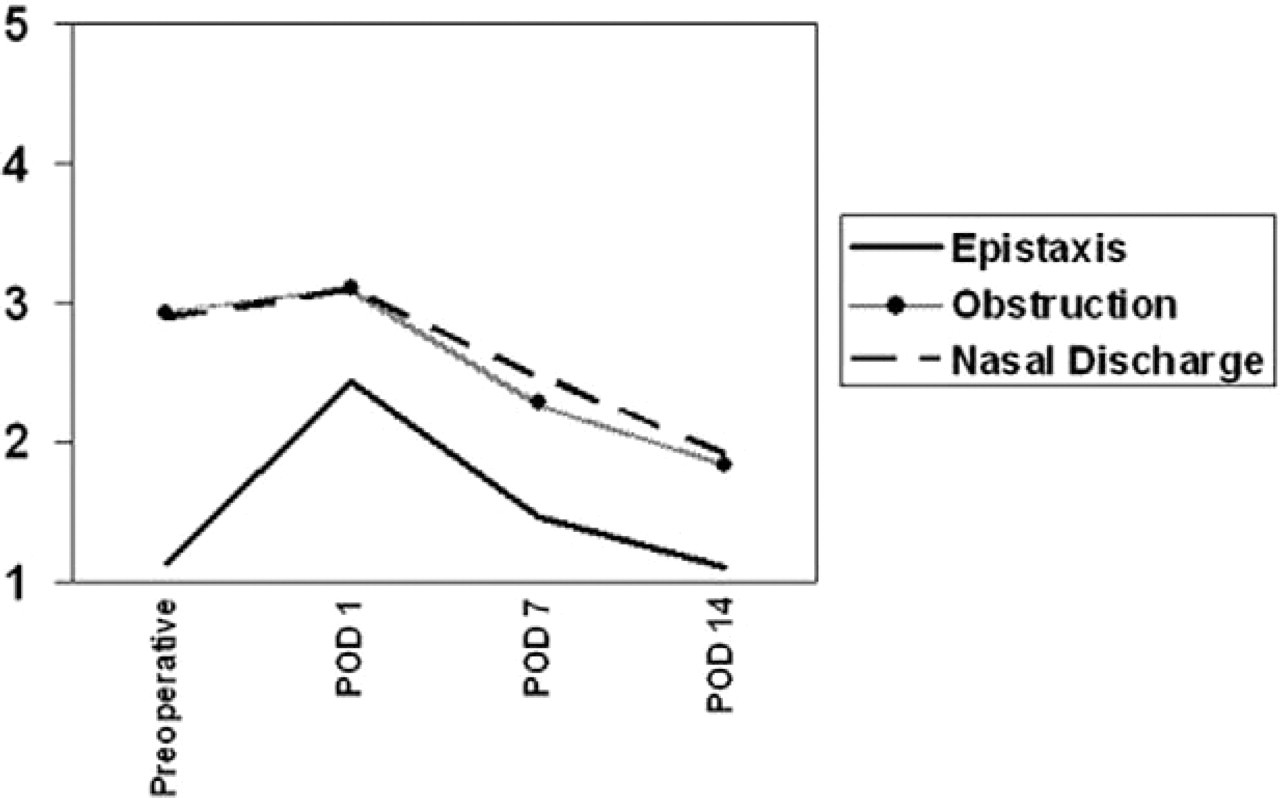
Time course for recovery of sinonasal symptoms rated on a scale from 1 (symptom absent) to 5 (maximum severity). Improvement in these symptoms over the recovery period was statistically significant (P < 0.05).
As a group, the only variable found to be significantly under- or overestimated preoperatively was epistaxis. Sixty-seven percent of patients expected to have no more than minimal nosebleeds postoperatively, but the majority (54%) actually reported experiencing a moderate amount of epistaxis on POD #1 (P = 0.04). For the remainder of the variables, there was no statistical difference between the aggregate expectations and the actual reported symptoms (P > 0.05).
Actual Postoperative Recovery
Over the 2-week postoperative period, patients demonstrated a statistically significant improvement in nearly all variables studied (P < 0.05), with the exception of sadness and difficulty sleeping, which remained unchanged throughout the recovery phase. Figures 3, 4, and 5 illustrate the time course for recovery of those variables found to be statistically significant over POD #1, POD #7, and POD #14.
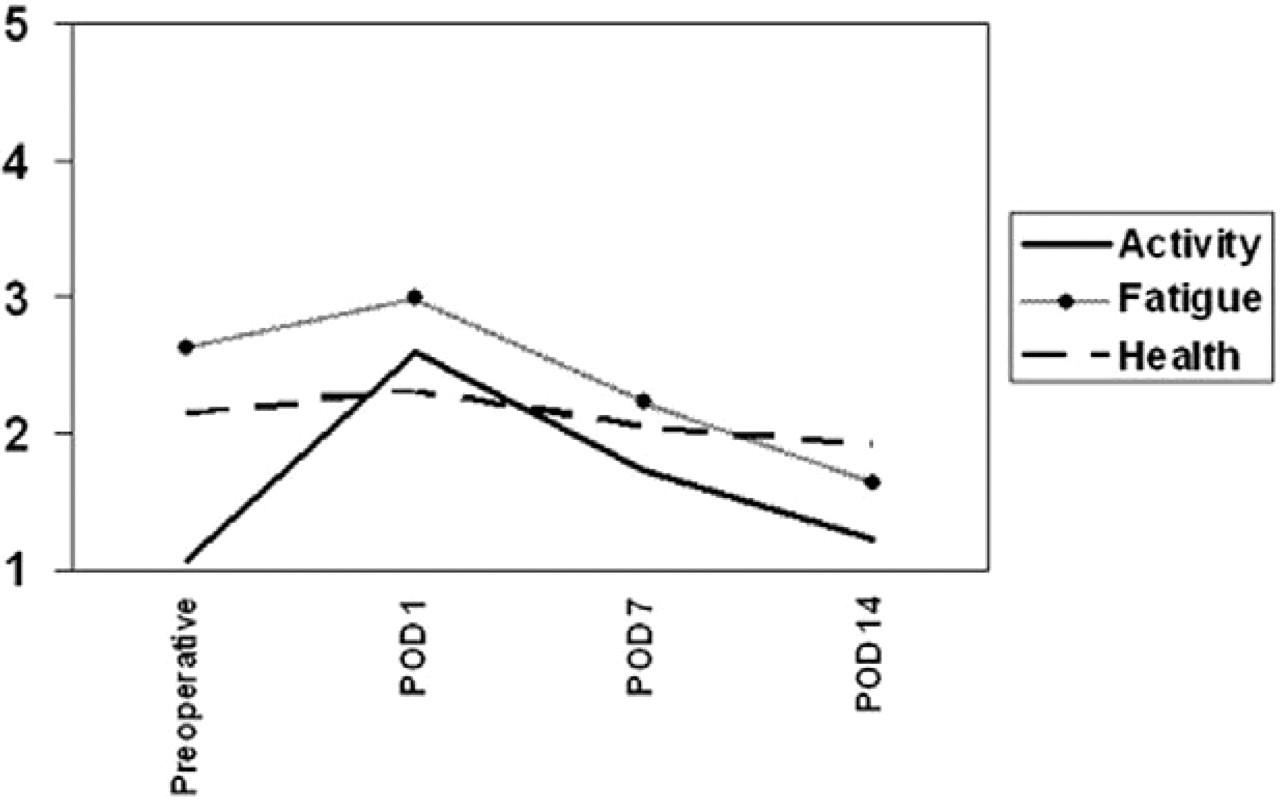
Time course for recovery of functional symptoms, including activity, fatigue, and overall health, was significant (P < 0.05) over the study period.
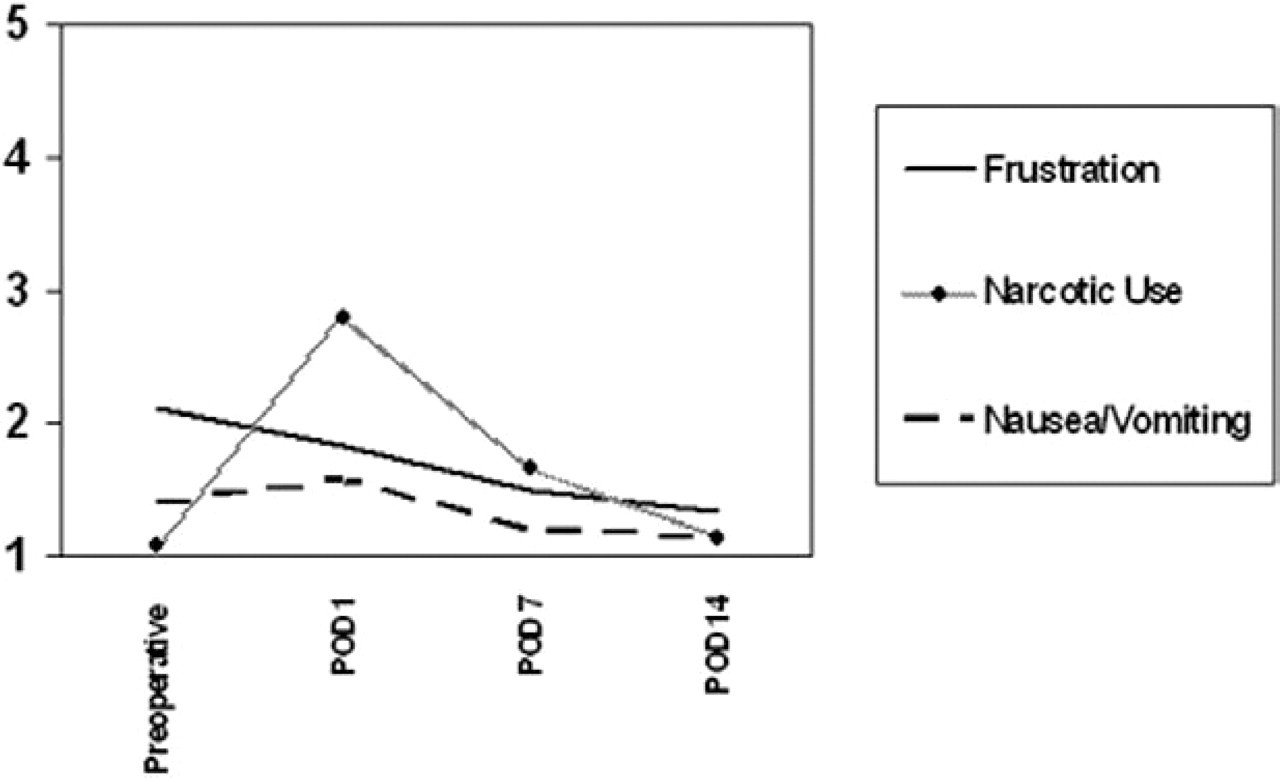
Recovery from the use of narcotic pain medications, frustration, and nausea/vomiting (P < 0.05).
Of particular importance was that as early as 2 weeks after ESS, patients reported a significant improvement over preoperative levels in several symptoms including nasal obstruction (P < 0.001), discharge (P < 0.001), fatigue (P < 0.001), and overall health (P < 0.05).
Analysis of pain medication use revealed that 7% of study patients admitted to using a narcotic pain medication regularly before surgery. The majority of patients (91%) did take the prescribed narcotic for pain control at least once on POD #1. However, by POD #7, 63% of patients had discontinued narcotic use entirely and 14% were using these medications just once daily. No patients reported using narcotics more than 4 times per day by POD #7. By POD #14, the vast majority (over 93%) were no longer using any narcotic pain medication (P < 0.001).
Of the 80% of study patients who were working (or attending school) full-time preoperatively, 75% returned to work without any restriction of duties by POD #7, and 100% were back to work by POD #14.
Factors Influencing Recovery
Several variables including demographic data, length of anesthesia, estimated blood loss, preoperative CT stage, and the specific surgery performed were examined to identify factors that influenced patient recovery following ESS. Male patients reportedly experienced greater frustration than female patients on the first day after surgery (P = 0.016). Age was also found to be a significant factor in recovery symptoms in that nasal obstruction on POD #1 was rated to be significantly worse by younger patients than those older than 50 years of age (P = 0.045). There were no other significant age- or gender-related differences in postoperative outcomes.
Patients who had a septoplasty performed at the same setting as their ESS appeared to have a more difficult postoperative course when compared to the cohort of patients who had ESS without septoplasty. On POD #1, the ESS with septoplasty group (n = 18) required significantly more narcotics for pain control when compared to those patients who had not had a septoplasty performed (P = 0.011). By POD #7, narcotic use was no different between the 2 groups. Septoplasty patients also experienced a greater decline in activity level on POD #1 (P = 0.029) and POD #7 (P = 0.016), and complained of increased POD #1 nausea and vomiting (P = 0.024). Epistaxis was also reported as being worse on POD #1 (P = 0.009) by the septoplasty group. The discrepancies in recovery symptoms between these 2 groups disappeared by POD #14.
Surprisingly, preoperative CT stage or surgical parameters such as operative length, volume of blood loss, number of sinuses opened at surgery, and history of previous ESS did not significantly impact patient recovery during the early postoperative period.
DISCUSSION
This is the first study to examine patient expectations of recovery from ESS and to document outcomes during the early postoperative period. The day after ESS, patients typically expected to experience a moderate degree of sinonasal issues (nasal obstruction, discharge, and bleeding) with only a minimal amount of psychosocial symptoms. This was generally consistent with what was actually experienced on POD #1, with the exception of the severity of epistaxis, which was underestimated by the majority of patients. We discovered that patient expectations of the recovery period vary widely, which highlights the importance of preoperative counseling and the bi-directional flow of information necessary during the informed consent process.
Key elements of an individual's recovery from surgery are pain control and the time frame of returning to work. 11 Our results showed that narcotic pain medications were discontinued or used just once daily by the large majority of patients by 1 week after surgery. This information is useful, as patients requiring significant amounts of narcotics after POD #7 (and certainly after POD #14) may warrant further evaluation. These findings may also be useful in gauging how much narcotic one should prescribe postoperatively for a routine ESS patient. With respect to functional recovery, the majority of patients had resumed their baseline activity level and had returned to work or school by POD #7. It is our practice to recommend no heavy lifting or straining for 7 days post-ESS, and it would appear that the majority of patients are physically and emotionally able to return to work by this time.
Our findings suggest that patients who have a septoplasty performed at the same setting as ESS can be expected to have a more difficult postoperative course. Other studies have suggested that much of the morbidity of septoplasty is related to the use of nasal splints or packing left in place for several days following this procedure. 12,13,14 All of our study patients, however, removed their packing the morning after surgery, and the septoplasty group still experienced significantly more pain, epistaxis, nausea and vomiting, and decreased activity than the nonseptoplasty cohort. Septoplasty, in and of itself, appears to increase the morbidity of sinonasal procedures.
We hypothesized that general anesthesia was the source of much of the morbidity associated with the early recovery period following ESS, and that perhaps more extensive procedures requiring longer periods of anesthesia would portend a poorer short-term outcome. This was not at all supported by our results. In fact, none of the surgical parameters investigated (including operative length, extent of surgery, blood loss, etc.) were significant factors in postoperative recovery. This was true even for the patient outcomes evaluated on POD #1—less than 24 hours after surgery. Previously published reports, however, have demonstrated that patients with more severe preoperative sinus disease tend to do worse over the long term. 15,16
In this study, we have documented a significant improvement in sinonasal symptoms and quality of life as early as 2 weeks after surgery. Prior outcomes research for CRS has established improvements over preoperative symptoms for a variety of time points postoperatively, ranging from months to years. 17,18,19 Considering that medical therapy of CRS is generally expected to impact patient symptoms over the time course of a few weeks, the rapid improvement demonstrated post-ESS is formidable. In addition to being efficacious, sinus surgery is generally well tolerated by the vast majority of patients.
The limitations of this study include its relatively small sample size and the possibility of a learning effect. The small sample size and limited number of questions in our survey could be a contributing factor to the variability noted in the Cronbach's alpha coefficients. In addition, one must consider the learning effect associated with subjects completing the same survey multiple times in a short time course, which might explain the increase in the coefficients noted over the postoperative time course.
CONCLUSIONS
Patient expectations of endoscopic sinus surgery vary widely, although this surgery is generally well tolerated with a brief recovery period. Postoperatively, the majority of patients experience a moderate amount of sinonasal symptoms, and only minimal psychosocial changes can be expected. Most patients can expect to return to work by 1 week after surgery. Concomitant septoplasty appears to increase the morbidity of ESS. Understanding patient expectations and the usual postoperative course based upon patient-centered data will improve communication and enhance our ability to prepare patients for surgery.
The authors would like to sincerely thank Dana Oliver, MS, biostatistician with the Department of Operations, St. Louis University Cancer Center, for her assistance in the statistical analysis of the data presented.