
Abstract
BACKGROUND: Sinonasal carcinomas, including nonkeratinizing (NK) squamous cell carcinoma (SCC) and sinonasal undifferentiated carcinoma (SNUC), are uncommon malignant neoplasms arising from the Schneiderian respiratory epithelium of the nasal cavity and paranasal sinuses. Due to their low frequency, the cytogenetic data on these tumors is limited.
METHODS: Seventeen patients who were operated on in our institution for extirpation of paranasal carcinomas were enrolled in this study. Fourteen pathologically confirmed samples of sinonasal carcinomas were cytogenetically analyzed using G-banding techniques after short-term culture. Three samples did not grow on culture.
RESULTS: Five of the 14 sinonasal carcinomas had an abnormal karyotype (36%). Of the 9 NK SCCs, 3 had abnormal karyotypes with numerical and structural chromosomal anomalies. Of the 5 patients with SNUC, 2 had an abnormal karyotype. One case of SNUC had a diploid complex karyotype. Another case of SNUC had a near triploid composite karyotype with 60–69 chromosomes. The chromosome arms that involved frequent breakpoint and rearrangements were: 1p, 6p, 7p, and 12q. We found that 3 of the 3 patients who died of disease displayed an abnormal karyotype, whereas 2 of the 11 patients who are alive displayed an abnormal karyotype (P = 0.027).
CONCLUSIONS: The study revealed that more than a third of the paranasal carcinomas carry an abnormal karyotype. No specific common aberrations were found in these tumors. To our knowledge this is the first attempt to investigate sinonasal squamous and undifferentiated carcinomas on a genetic level using G-banding technique. Additional studies are required in order to determine whether cytogenetic data may serve as an adjunct to conventional pathology for the diagnosis and prognosis assessment of these rare and highly aggressive tumors.
Squamous cell carcinoma (SCC) of the nasal cavity and paranasal sinuses is a rare malignant neoplasm with an incidence of less than 1:200,000 per year. The most common malignant lesion in the sinonasal tract, it accounts for approximately 3% of all carcinomas of the head and neck. Most sinonasal SCCs are well to moderately differentiated, with a positive stain to cytokeratine. 1 Less frequently, poorly differentiated nonkeratinizing (NK) SCC, adenocarcinoma, or sinonasal undifferentiated carcinoma (SNUC), which lack the typical features of conventional SCC, can arise from the sinonasal epithelium. Nonkeratinizing SCC (also known as transitional cell carcinoma, intermediate cell carcinoma, or Schneiderian carcinoma) is considered a variant of SCC, whereas sinonasal undifferentiated carcinoma is a pathologically distinctive neoplasm which also lacks squamous differentiation. This tumor is composed of medium-size undifferentiated cells, with occasional mixed neuroendocrine features. Both SNUC and NK SCC are locally aggressive, and usually present as a large paranasal mass spreading into the anterior skull base, orbit, and dura. Complete surgical resection followed by irradiation is the mainstay of treatment in these cases, and the prognosis of patients varies between 20% and 70% 5-year survival. 2,3
The classification and pathological diagnosis of sinonasal carcinomas may be difficult. Due to their low frequency, the cytogenetic data on these tumors is limited, and the only previous study, which included 3 cases of SCC, reported various complex chromosomal abnormalities, with no specific karyotypic patterns. 4
In the current study, we cytogenetically characterized the short-term cultures of NK SCC and SNUC originating in the nasal cavity and paranasal sinuses. We describe the specific chromosomal abnormalities found in these tumors and correlate between the karyotype and the clinical outcome of the patients.
MATERIALS AND METHODS
This study involves 17 patients who were operated on in our institution between 2001 and 2004 for extirpation of sinonasal carcinomas. Of the 17 tumors, 14 pathologically confirmed samples were analyzed using classical cytogenetic methods. The demographic features of the patients are summarized in Table 1. The pathological diagnosis was performed according to the World Health Organization's Histological Classifications of Tumors. 1 Nine tumors originated in the maxillary sinus and 5 in the ethmoidal sinuses. All patients had received postoperative radiation therapy except patient 4, who had tumor recurrence and received 7700 cGy 2 years prior to her current operation. The oncological outcome of the patients is based on 16 to 48 months of clinical and radiological follow-up. Tumor staging was performed using the American Joint Committee on Cancer-Union Internationale Contre le Cancer (AJCC-UICC) 2002.
Chromosomal Analysis
A classical cytogenetic analysis was performed on in situ metaphases from primary short-term cultures. The tissue samples for cytogenetic and pathological analysis were taken directly from the fresh surgical specimens. A biopsy from the core of the tumor was mechanically disintegrated and digested for 2 hours with 400 U/mL type II-S collagenase (Sigma, St. Louis, MO). Cell suspension was cultured in RPMI 1640 medium supplemented with 17% fetal calf serum and 2% antibiotics at 37°C in 5% CO2 for 6 to 10 days. Cytogenetic analysis was made according to a standard technique as described previously. 5 Chromosome aberrations were determined according to the International System for Human Cytogenetic Nomenclature, Guidelines for Cancer Cytogenetics. 6
Statistical analysis was performed using Mantel-Haenszel and Fisher Exact tests (Statcalc). Five to 25 metaphase cells from primary cultures were studied in each specimen using G-banding technique (220 metaphase overall). The study protocol was approved by the local Institutional and National Review Board (IRB Approval No. 03-061).
RESULTS
The histopathological data and karyotypes of the tumors are summarized in Tables 1 andTable 2 respectively. Five of the 14 sinonasal carcinomas had an abnormal karyotype (36%).
Demographic and clinical data of patients
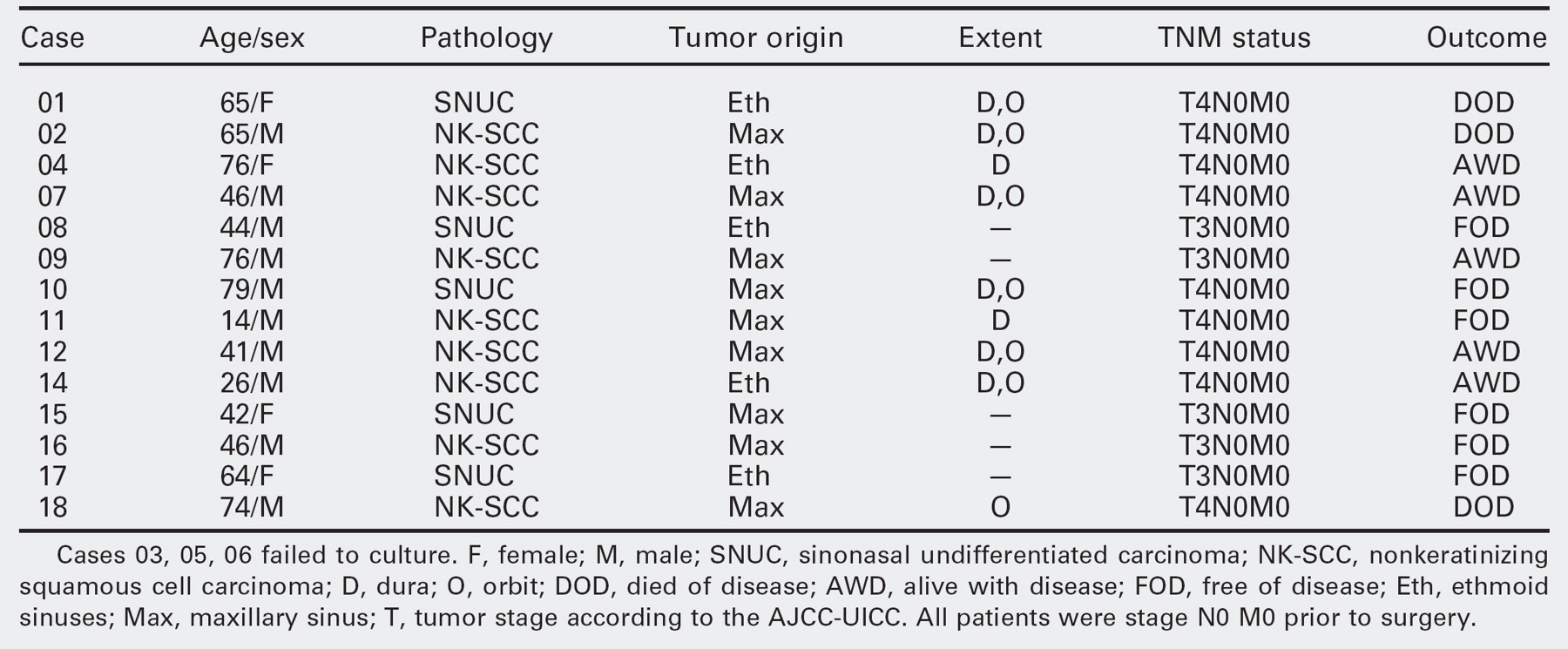
Cases 03, 05, 06 failed to culture. F, female; M, male; SNUC, sinonasal undifferentiated carcinoma; NK-SCC, nonkeratinizing squamous cell carcinoma; D, dura; O, orbit; DOD, died of disease; AWD, alive with disease; FOD, free of disease; Eth, ethmoid sinuses; Max, maxillary sinus; T, tumor stage according to the AJCC-UICC. All patients were stage N0 M0 prior to surgery.
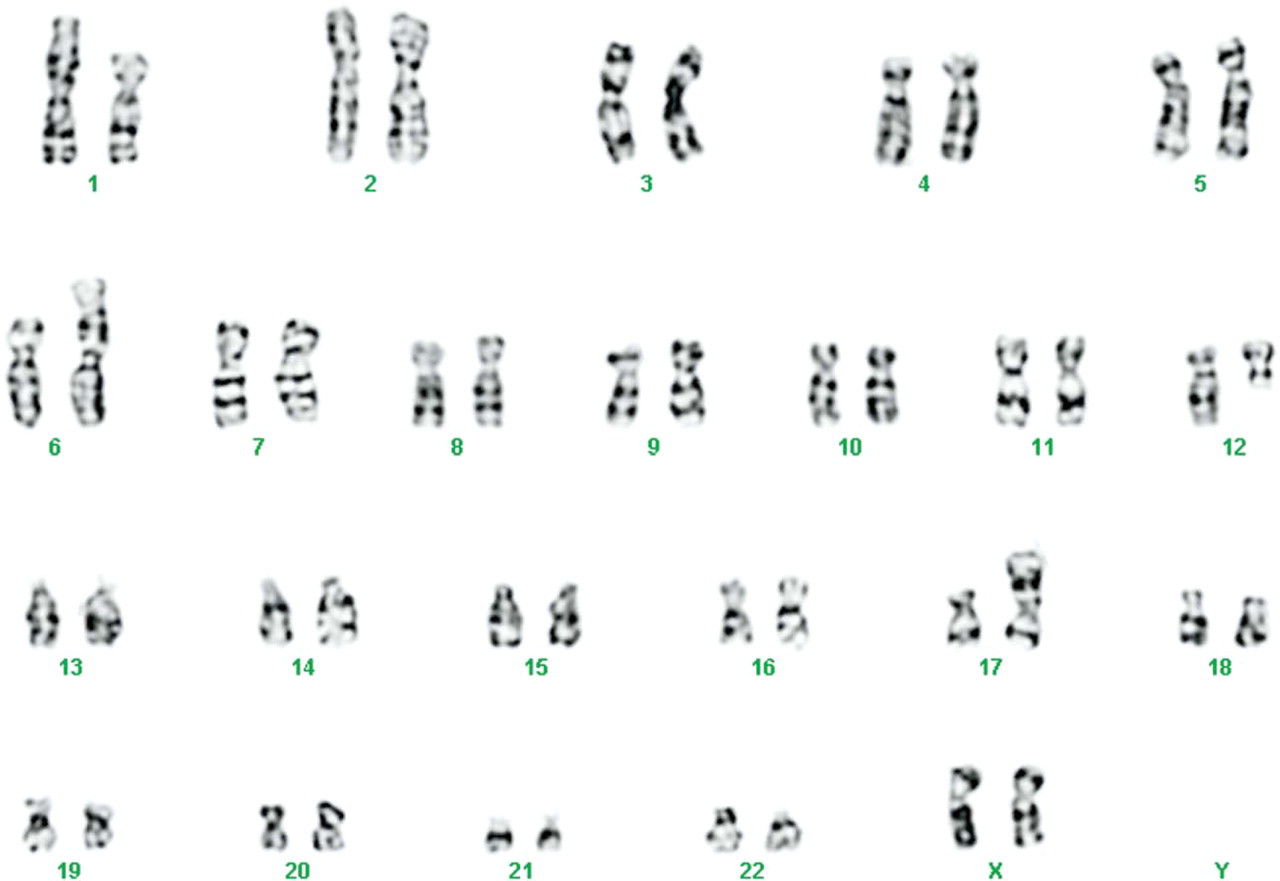
Two of the 9 NK SCCs (cases 4 and 18) had significant chromosomal abnormalities and 2 cases (case 2 and 9) had chromosomal changes that are not related to the tumor. The principal chromosomal abnormality found in all cells of case 2 was inv(2)(p11q13), which is frequently found in the Jewish population in Israel (see also A.O-U. and R.S. personal communication). 7 This tumor also demonstrated abnormal clone with a trisomy of chromosome 8 (Table 2). Case 4 had a near diploid composite karyotype containing clonal abnormalities involving chromosomes 1, 6, 7, 8, 10, and 12 (Fig 1). Case 9 showed 2 clones of cells with a normal karyotype and a loss of Y-chromosome. Case 18, which had suffered from NK-SCC originating in the maxillary sinus, also had a composite karyotype involving chromosome arms 1p, 2p, 3q, 4p, 5p, 6q, 7p, 7q, 10p, and 15q (Fig 2).
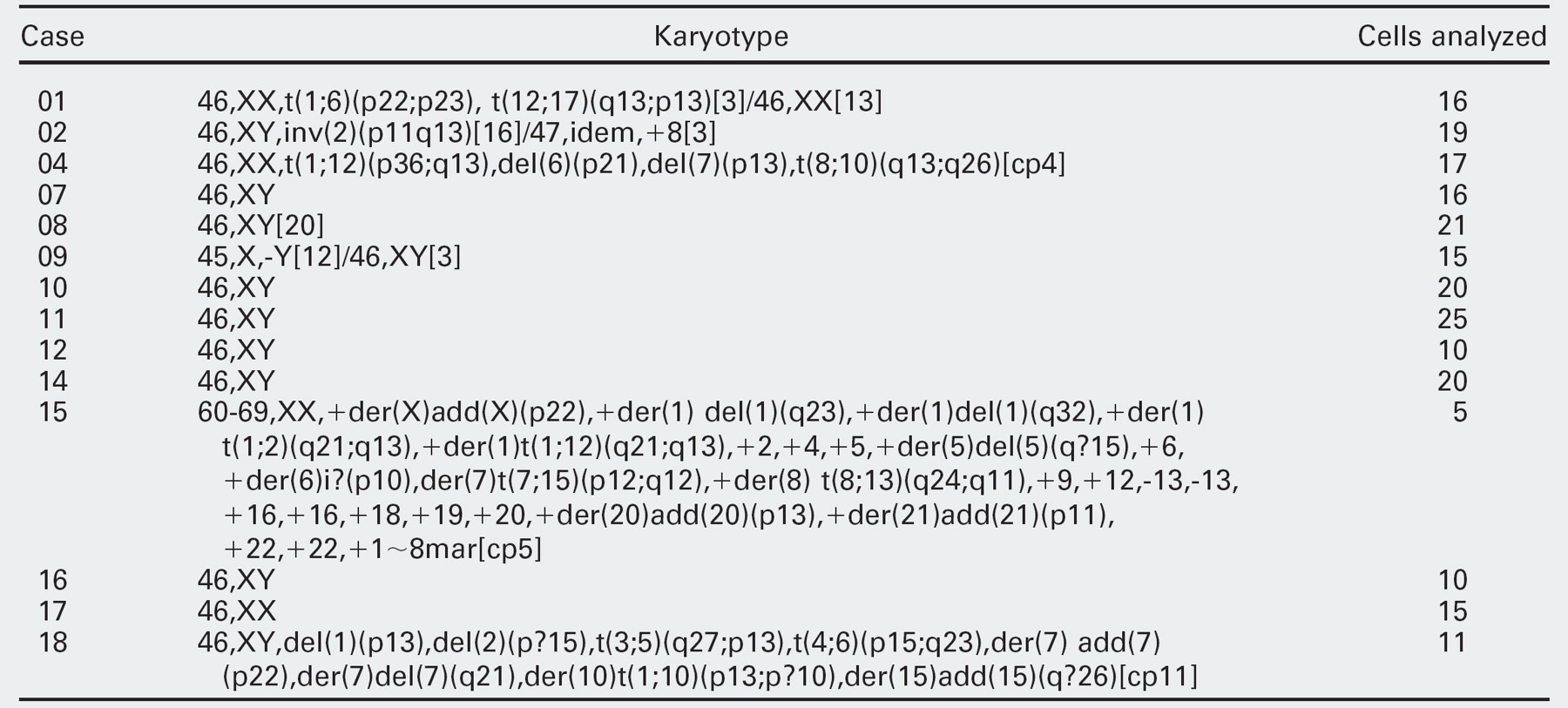
Specific karyotype of patients
Of the 5 patients with SNUC, 2 had an abnormal karyotype (cases 1 and 15). One of the 5 SNUC (Case 1) had a complex karyotype, with 2 translocations involving chromosomes 1, 6, 12, and 17 (Fig 3) in 3 cells (see Table 2). Case 15, which had also suffered from SNUC originating in the maxillary sinus, had a composite karyotype with 60-69 chromosomes (Fig 4).
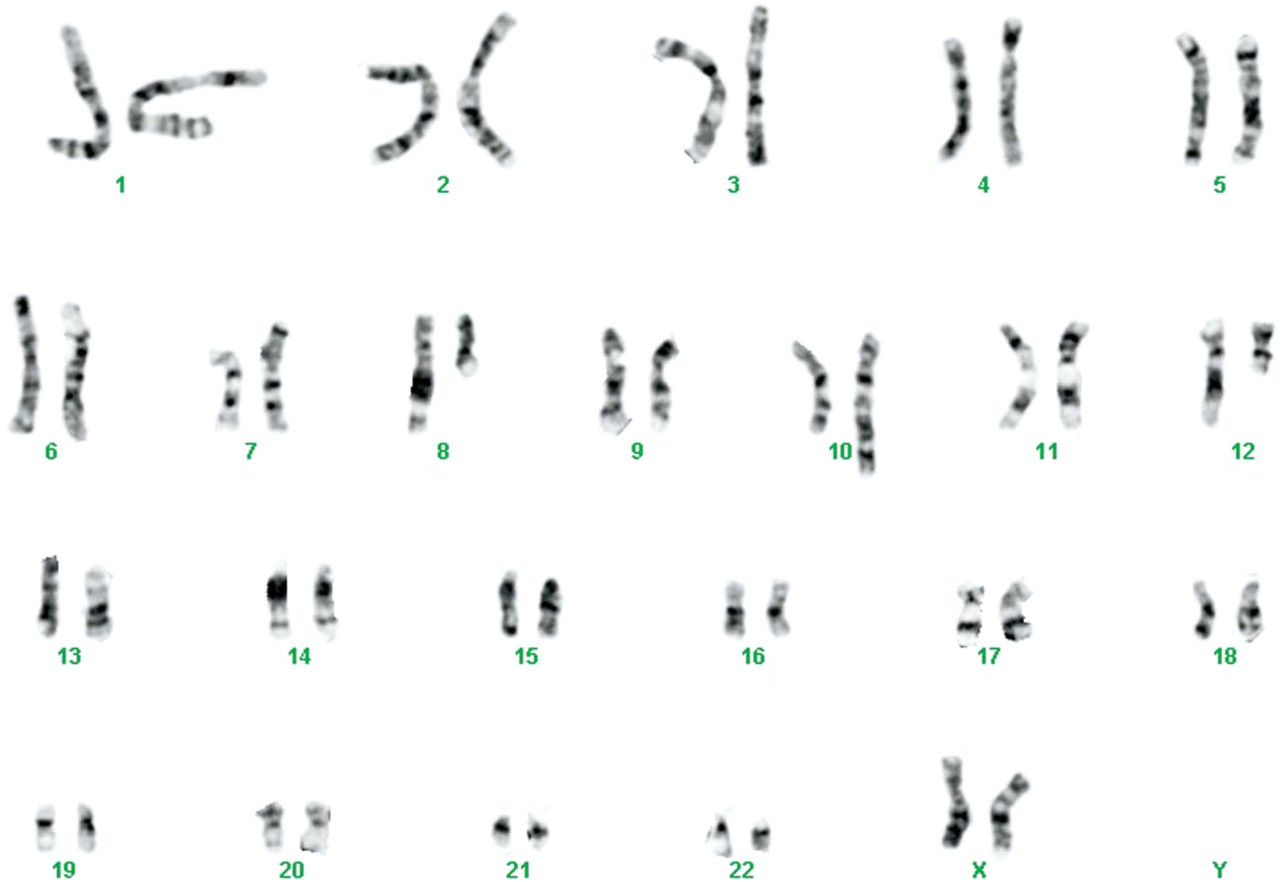
A representative karyotype from the poorly differentiated nonkeratinizing SCC of case 4.
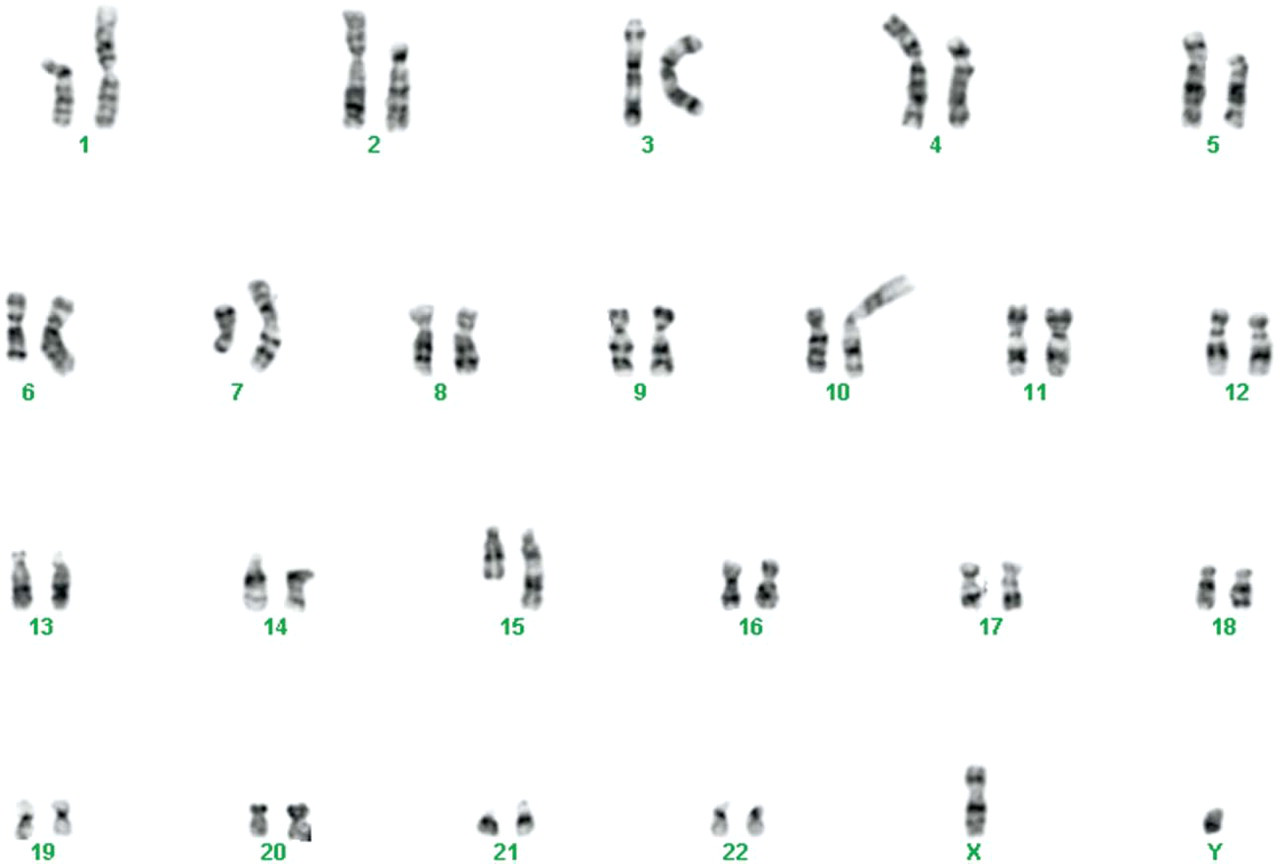
The karyotype of case 18 with nonkeratinizing squamous cell carcinoma showing a diploid complex karyotype.
It is worth noting that several chromosomal arms were involved in breakage and rearrangement at various breakpoints such as 1p (cases 1, 4, 18), 6p (cases 1, 4, 15), 7p (cases 4, 15, 18), and 12q13 (cases 1, 4, 15).
All patients were followed on a regular basis using both clinical and radiological examinations. The mean follow-up time was 24 ± 8 months and the 2-year survival rate was 78%. Three of the patients enrolled in this study have died of disease (cases 1, 2, and 18) and all 3 of them displayed an abnormal karyotype. Two of the 11 patients who are alive had a complex karyotype (cases 4 and 15). Statistical analysis of the data suggested that abnormal karyotype may be associated with poor prognosis of patients with paranasal SCC (P = 0.027 Fisher Exact test).
DISCUSSION
Cytogenetic information on sinonasal SCC is scarce due to the low incidence of this tumor. Three reports with 5 cytogenetically abnormal karyotypes of paranasal SCC 4,8,9 and one of undifferentiated carcinoma 10 have been described. All of the previously reported tumors displayed a complex karyotype with unbalanced translocations and deletions. In our study we have found that 5 of the 14 analyzed sinonasal specimens displayed an abnormal karyotype. Most of the chromosomal abnormalities involved few clones with composite karyotypes.
This report is also the first to describe 2 novel translocations, t(1;6)(p22;p23) and t(12;17)(q13;p13), in sinonasal carcinoma. The loss of chromosome Y in tumor 09 was not described before in SNUC. However, loss of Y-chromosome can be present in both normal and malignant cells and its frequency is known to increase with age in both situations. 11,12 Therefore the presence of a 45,X,-Y cell population in a 76-year-old patient is most likely associated with advancing age, and should not be interpreted as a marker of the malignant clone. The cytogenetic features of sinonasal NK SCC described herein resemble those previously reported by Jin et al, 4,8 while the karyotype of the SNUC is different from that previously described by Gollin and Janecka, which had a complex diploid karyotype. 10
SCC of the upper aerodigestive tracts frequently harbors a highly complex karyotype as found in our study. Chromosomal aberrations involving similar breakpoints were previously described in SCC of the oral cavity, larynx, hypopharynx, and nasopharynx. 8,13,14
Translocation (12;17)(q13;p13) as found in case 1 was previously described in breast adenocarcinoma and acute monoblastic leukemia. 15,16
Our search of the literature revealed few candidate genes that may be involved in oncogenesis of this tumor. Tumor protein 53 (TP53) is a tumor suppressor gene which is mutated in about 50% of human cancers. TP53 mutation can be also found in about 40% to 60% of head and neck cancer cases. 17 This gene was mapped to a region on 17p13, the same region that involved the first translocation reported here. Another important gene located on chromosome arm 12q13 is the activating transcription factor 1 (ATF1) gene, a member of the CREB/ATF subfamily of bZIP transcription factors. This gene is also rearranged in clear cell sarcomas of soft tissue with t(12;22)(q13;q12), where its DNA-binding domain is fused with the N terminus of the EWS gene. 18 The other translocation in this tumor, t(1;6)(p22;p23), was never described before. The human DEK gene is located on chromosome arm 6p23 and codes a site-specific DNA binding protein involved in transcriptional regulation and signal transduction. 19 This protein was discovered in a subset of patients with acute myeloid leukemia. Further research is required to study the role of these cancer-related genes in the development of SNUC.
A representative karyotype from the sinonasal undifferentiated carcinoma of case 1.
Chromosomal abnormalities involving 1p, 6q, and 12q were found in 3 of our cases. Although not specific, such aberrations may be found in SCC of the oral cavity, larynx, nasopharynx, and hypopharynx. 20
Ariza and his colleagues have used comparative genomic hybridization to detect recurrent chromosomal abnormalities in a large series of patients with sinonasal adenocarcinoma. 21 Sinonasal adenocarcinoma differs from other carcinomas of the paranasal sinuses in its histological appearance. Adenocarcinoma has strong association with wood and leather manufacturing, and therefore serves as a model for identification of carcinogenesis initiated by environmental mutagens. Common aberrations found in this tumor involve gain of chromosomal arm 19p and Xp22. Interestingly, we have found gain of chromosomes Xp22 in one patient with SNUC. This data may indicate a common mechanism for the development of SNUC and sinonasal adenocarcinoma.
In addition to the cytogenetic data, we assessed the association between karyotype and prognosis. We have found that all of the 3 patients who died of disease displayed an abnormal karyotype, whereas 2 of the 11 patients who are free of tumor had chromosomal changes. These differences were statistically significant. Nevertheless, our series involves a small number of patients and further studies are required to evaluate the clinical significance of these findings.
In our series, 64% of the tumors had a normal tumor karyotype. This may suggest that the tumor cells have not undergone cytogenetic changes and therefore the biological behavior of the tumor is relatively slow. Another explanation for a normal karyotype is that the analyses represent normal stromal cell proliferation in culture rather than tumor cell growth, and therefore represent the constitutional karyotype of the patient.
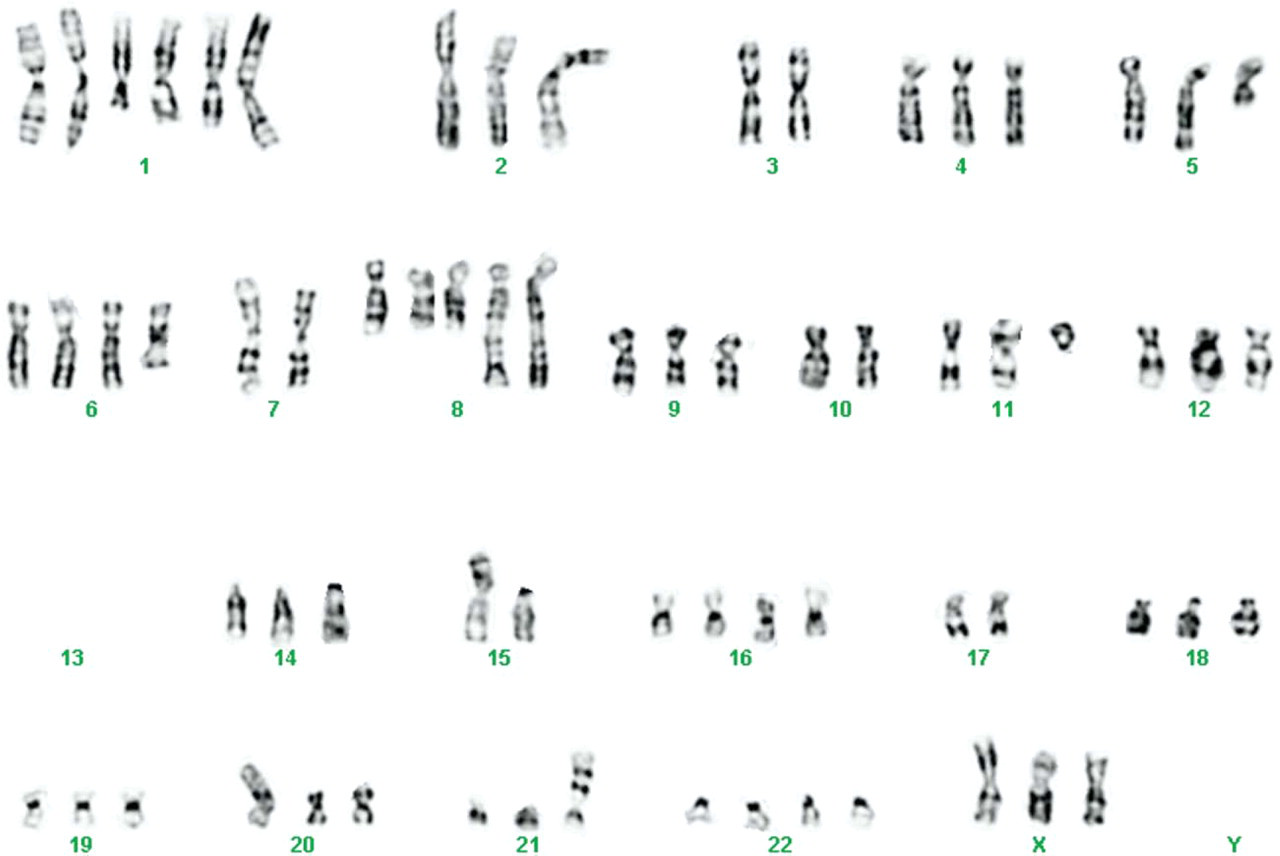
The karyotype of case 15 with sinonasal undifferentiated carcinoma showing a triploid complex karyotype.
Previous studies have demonstrated the prognostic value of cytogenetic data in head and neck SCC. 17 To date, the extent of the cytogenetic data on sinonasal carcinomas is too limited to furnish precise association between karyotype and prognosis. Additional studies are required in order to determine whether cytogenetic data may serve as an adjunct to conventional pathology for the diagnosis and prognosis assessment of these rare and highly aggressive tumors.
This work was supported by the Israeli Cancer Association Grant to Z.G. and A.O-U.