
Abstract

A 4-year-old Chinese boy presented to the pediatric gastroenterology clinic at Chang Gung Memorial Hospital with a complaint of poor appetite and postprandial vomiting. He also had a cough and rhinorrhea. Although his vomiting subsided after treatment with a prokinetic agent, his appetite did not improve.
Six months later, the child was reevaluated in the ear, nose, and throat clinic for an incidentally noted throat mass. Otolaryngologic examination revealed a well-circumscribed mass, 3 cm in diameter, located in the left supratonsillar fossa with extension into the paranasopharyngeal area. The cystic mass was not attached to the left side of the Rosenmuller's fossa and the left Eustachian tube orifice was normal. No other remarkable findings were noted in the neck. On palpation, the mass was cystic in consistency. Otoscopy revealed a dull left-side tympanic membrane.
CT scan of the nasopharynx showed a low-density mass, 2.7 cm in diameter, attached to the posterior and lateral walls of the left nasopharynx. To more clearly delineate the extent of the involvement and the relationship of the mass to the neighboring structures, MRI was obtained. T1- and T2-weighted MRI images demonstrated hyperintense signals in the left nasopharyngeal and paranasopharyngeal areas (Fig 1). The patient had a normal hearing threshold on playing audiometry; however, the tympanogram showed type C on the left. After completion of the preoperative evaluation and review of the treatment options with the family, the patient was taken to the operation theater where, under general anesthesia, a 3×2-cm cyst was excised via a transpalatal approach. Intraoperatively, the tumor was found to run into the parapharyngeal space, adjacent to the internal carotid artery. The left-sided tumor cyst and tonsil were totally excised.
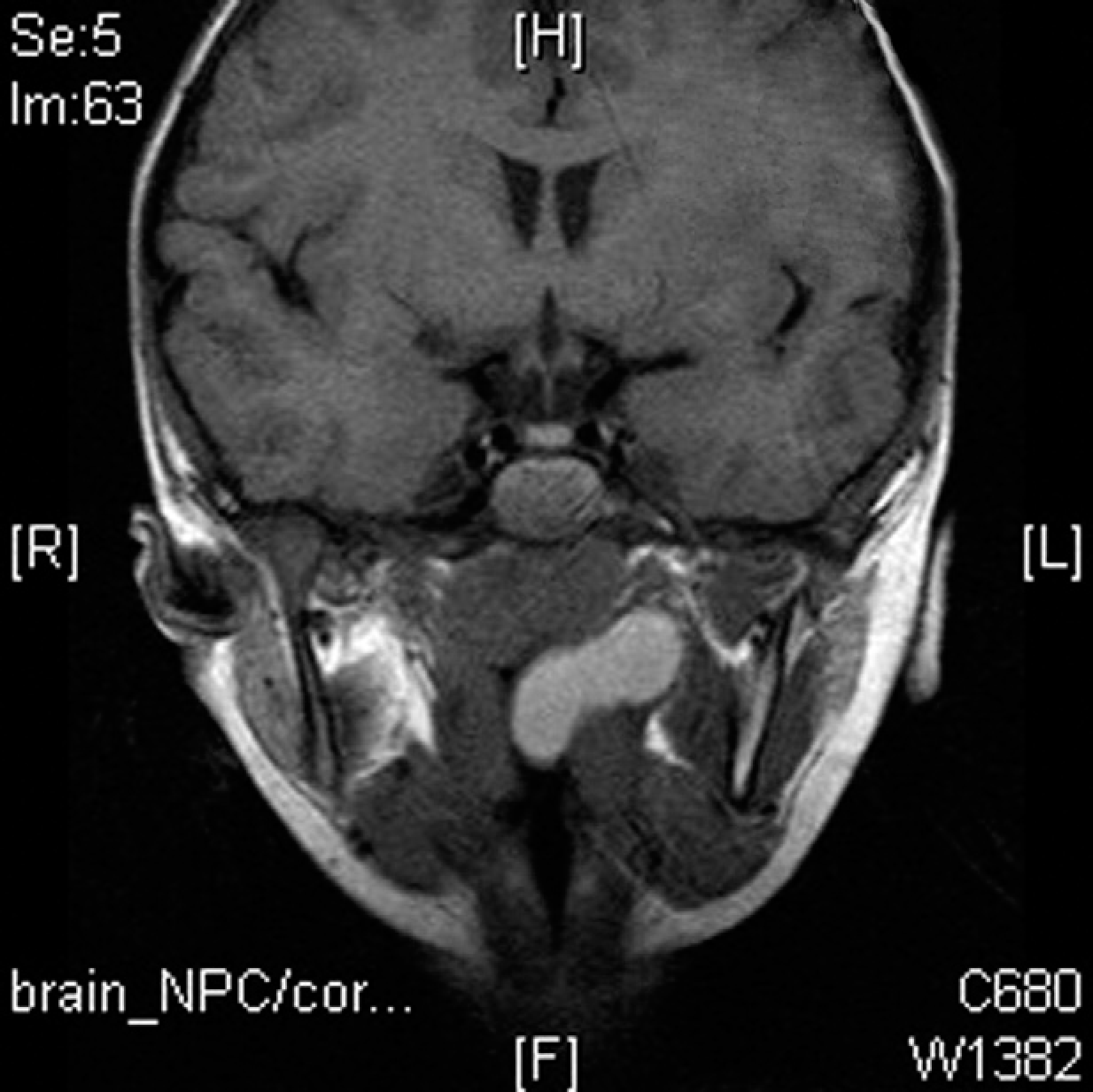
MRI, coronal view, T-1 weighted; the mass extends from the left lateral nasopharyngeal wall down to the parapharynx.
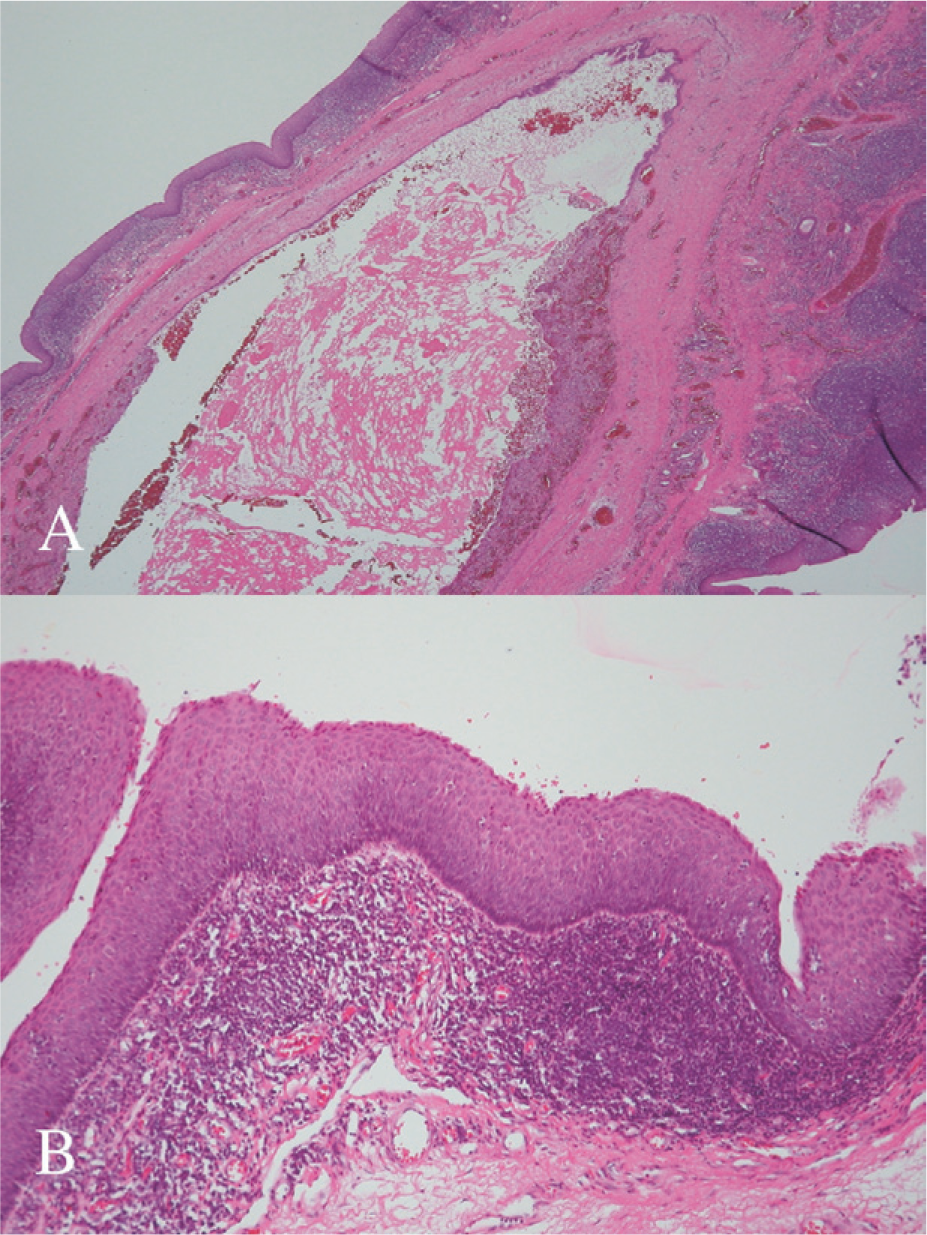
Histological examination confirmed a cystic mass containing lymphoid tissue and covered with both ciliated pseudostratified columnar and stratified squamous epithelium, consistent with a branchial cleft cyst (Fig 2A and B). There was no evidence of recurrence over 6 months of follow-up.
Discussion
Two theories have been postulated to describe the etiology of internal branchial cysts. The first suggests that, due to the presence of subepithelial lymphocytes, the cyst is most likely derived from ectopic epithelial cells in the regional lymph node.3 The second theory, which is more widely accepted, suggests that the cysts are derived from remnants of the branchial apparatus.3 The branchial apparatus forms during the third to seventh weeks of embryonic life and contributes to many components of the head and neck region.4 It consists of 5 paired branchial arches, each separated externally by ectodermal clefts and internally by endodermal pouches.2 They may present as fistulas, sinus tracts, or cysts.2 Fistulas and sinus tracts of second branchial cleft origin run deep to the platysma muscle, ascend along the carotid sheath, and course between the internal and external carotid arteries, overlying the hypoglossal and glossopharyngeal nerves.2 They typically end in the upper half of the posterior faucial pillar, the supratonsillar fossa, or directly on the tonsillar surface. Because the dorsal portion of the second branchial pouch blends with the first pouch, there is still controversy regarding which pouch contributes to the nasopharyngeal branchial cleft cyst.4 Shidara and colleagues described two cases of nasopharyngeal cysts of branchial origin and considered them to originate from the dorsal part of the second branchial pouch or the layer of endodermal cells cut off from the lower part of the Eustachian tube, which was a derivation of the first branchial apparatus.5 Meanwhile, Papay and colleagues reported a case of nasopharyngeal branchial cleft cyst and explained that the embryologic origin was from the most lateral extension of the second branchial apparatus.1 Due to the presence of the parapharyngeal attachment and the lack of deformity in the first branchial apparatus derivatives such as the Eustachian tube, Rosenmuller's fossa, or external ear canal, the embryologic origin of the naso-pharyngeal cyst in our case was believed to be derived from the second branchial apparatus.
The differential diagnoses of nasopharyngeal tumors include Rathke's pouch, adenoid retention cyst, second branchial cleft cyst, Tornwaldt's cyst, chordoma, dermoid cyst, herniation of the central nervous system, sphenoid sinus mucocele, and nasopharyngeal carcinoma (NPC).
The appearance of a cystic mass in the lower nasopharynx is a rare occurrence. The location itself excludes many pathologic entities including NPC, one of the most common cancers among Chinese males, which is always among the list of differential diagnoses. However, NPC commonly presents as an ulcerative mass in the Rosen-muller's fossa in an adult male or, uncommonly, in a female. The case we reported is of a 4-year-old boy with a mass that was cystic in character and located right between the nasopharynx and oropharynx. Imaging studies revealed a cystic composition, which rightfully excluded the possibility of NPC.
The differential between a Tornwaldt's cyst and a branchial cleft cyst is initially based upon the anatomic location. A Tornwaldt's cyst is usually located in the mid-line whereas a branchial cleft cyst lies more laterally, close to the Eustachian tube orifice,6 as noted in our case. The epithelium of the branchial cleft cyst is stratified squamous or columnar ciliated epithelium underlayed by abundant lymphoid tissue, often with germinal centers. The cystic contents may be clear, mucinous, or seromucinous fluid. The microscopic feature of a Tornwaldt's cyst is an epithelial-lined cyst with no surrounding lymphoid tissue.6
The current recommended management of a second branchial cleft cyst is complete surgical excision, which, in the represented case, was very successfully done using a transpalatal approach.
(