
Abstract
Similar to an increase in atopic conditions, numerous allergists believe that the prevalence of food allergy is rising. Food allergies in childhood have been found to vary in frequency from 6% to 8% in the general population. 1 Previous studies indicate milk allergy affects approximately 2.5% of infants, with 1% of these IgE mediated. Egg allergy has been estimated at 1.6% to 2.6%. 2
An association between serous otitis media and food allergy has been demonstrated. Nsouli et al 3 evaluated 104 patients with recurrent serous otitis media. Of the study population, 78% were found to meet criteria for food allergy. The study demonstrated a high concordance rate between recurrent serous otitis media and food allergy, however, a variety of methods to analyze allergy were utilized including skin prick, specific serum IgE antibodies (RAST), and open food challenge. The association between allergy and otitis media is still controversial, and the literature is cautious in relating the two. In our study, we utilized only the Pharmacia ImmunoCAP™ (Kalamazoo, MI) based on IgE and hypothesized that children requiring ENT procedures had a higher prevalence of food allergy than the general pediatric population.
PATIENTS AND METHODS
Children aged 0 to 18 years whose medical condition met criteria for an outpatient surgery center over a 2-year time period (2001 to 2003) were considered eligible. Children underwent ENT procedures, including bilateral myringotomy tubes (BMT) alone, BMT + adenoidectomy, adenoidectomy alone, or BMT + adenoidectomy + tonsillectomy. No effort was made to exclude children with syndromes or mild immune deficiency. Children were excluded if parents declined allergy testing. Clinical and demographic data was recorded. Patient history or family history of allergy was documented.
PharmaciaCAP™ IgE FEIA (Florescence Immunoassay) systems were utilized. Sera from 242 subjects were analyzed for increased total IgE antibodies, as well as specific IgE antibodies to antigens, including milk, egg, beef (from all but 10 patients), wheat, soy, and environmental allergens (excluding 1 patient).
The PharmaciaCAP™ system demonstrates a 15% increase in sensitivity over the original RAST (Radio Allergo Sorbent Test) system. A detailed explanation of the PharmaciaCAP system™ is beyond the scope of this study. Basically, however, it is a sandwich immunoassay with a solid-phase bound allergens are allowed to react with antibodies from a patient's blood sample. These specific antibodies are detected using IgE specific(Fc) portion generating florescence that is measured. The assay is calibrated against the WHO standard. The entire test system is built around the 0.35 kUA/1 calibrator for specific IgE antibodies.
The Alternative Scoring Method was used for the specific IgE allergens. With this method, 100% correlated to a value of 0.35 kU/L that corresponds to the conventional thresholds for IgE specific antibodies. The healthy individual has a very low level of specific IgE in the blood, normally below 0.35 kUA/1. The values were reported by conventional laboratory as percentages and classes: Class 0, <60%; Class 1, 70% to 110%; Class 2, 110% to 220%; Class 3, 220% to 600%; Class 4, 600% to 2,000%; Class 5, 2,000% to 6,000%; and Class 6, 6,000%. 4 Using these values, a positive food allergy was documented if the patient had a percentage ≥100% or >0.35 kU/L. Total IgE was recorded in kU/L, and elevated levels were determined in the lab based on age groups.
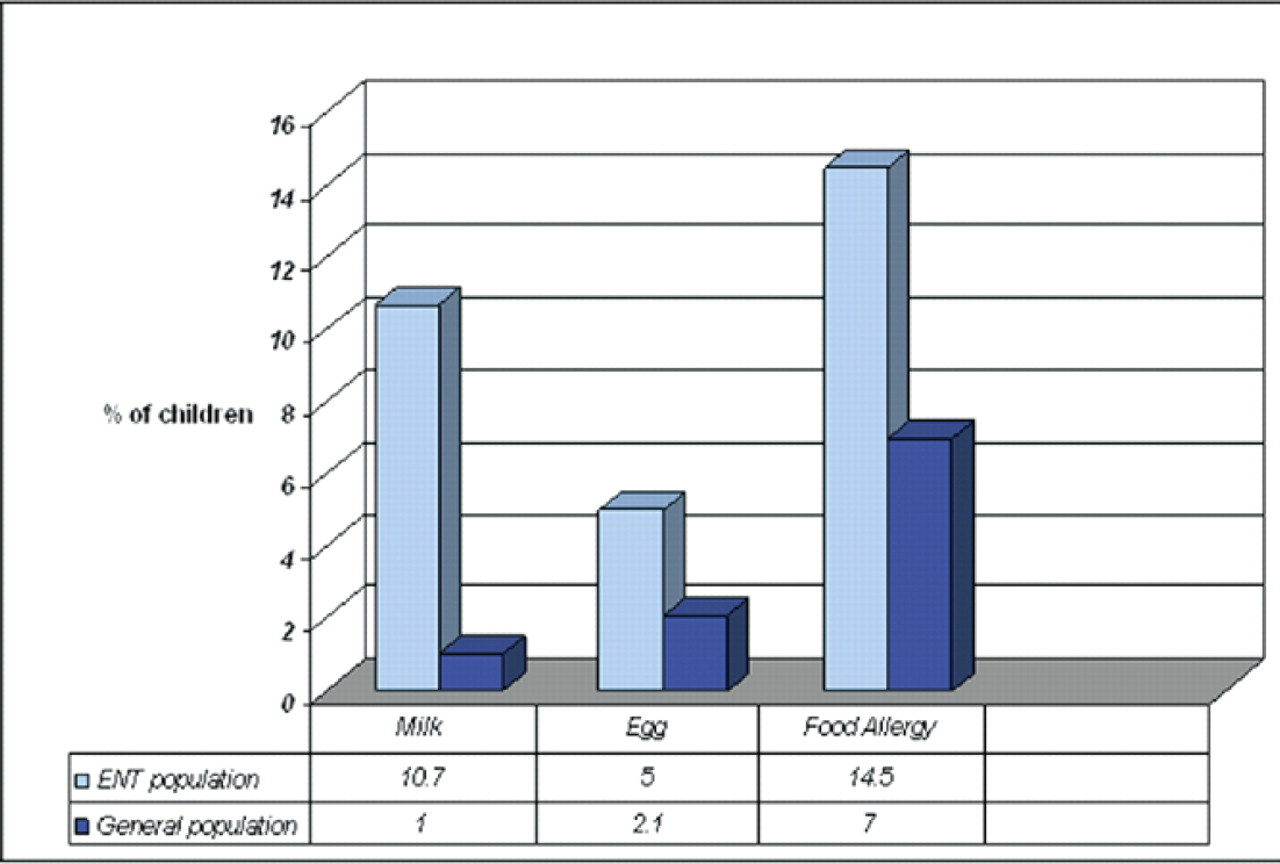
Prevalence of milk, egg, and total food allergy in the study population vs the general population. The numbers recorded in the ENT population correspond to percentage of patients with specific IgE ≥ 0.35 kU/L.
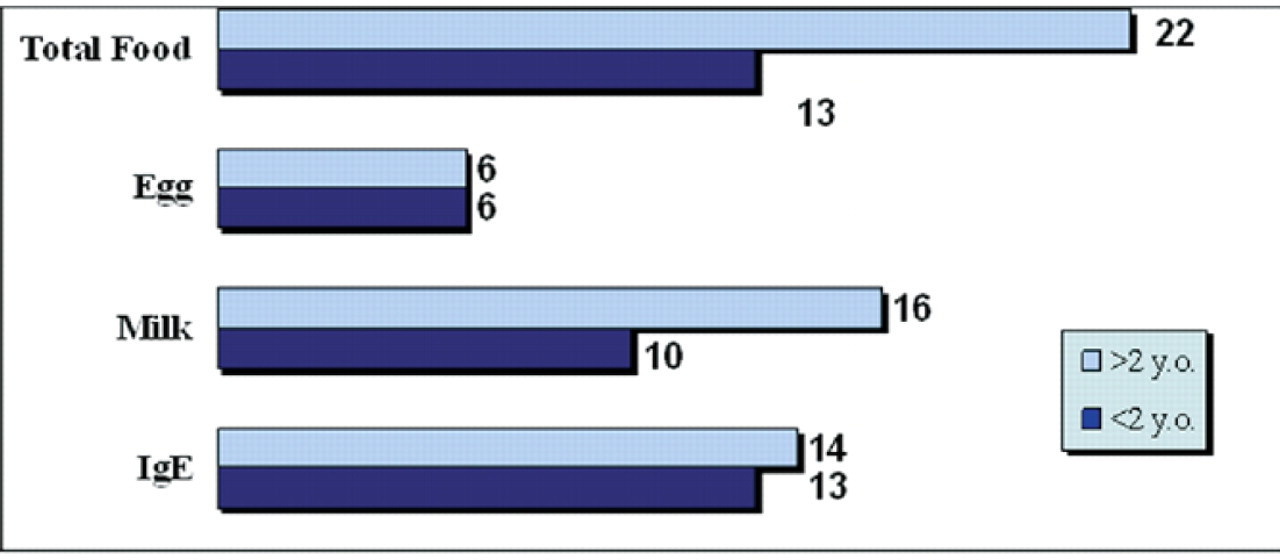
Research has suggested that after 2 years of age, children with food allergy begin to decrease response to allergens. In this study, children >2 years of age demonstrated a higher prevalence of food allergy.
The food allergy panels utilized did not include peanut, which may have resulted in a slight decrease in prevalence of food allergy. It is important to note that peanut is not a common allergy, but is more noted for its association with anaphylaxis. The prevalence of peanut allergy in the pediatric population has been approximated at 0.6%. 2
RESULTS
The study population included 242 patients. Children ranged in age from 5 months to 15 years. Mean age was 4.7 years with a SD of 2.9 years. A total of 140 (57.9%) patients were male and 102 (42.1%) were female. A positive family history of allergy was found in 77.3% of patients. Family perception of allergy in their children was 70.7%. Elevated IgE was found in 27 of 242 (11.2%). Milk allergy had a prevalence of 26 of 242 (10.7%). Egg white allergy was found in 12 of 242 (5.0%). The prevalence of overall food allergy in the study population was 35 of 242 (14.9%). In addition, increased specific IgE to environmental allergens (tree, grass, mold, dust, dog, cat) was found in 29 of 242 (12.0%).
Figure 1 compares the prevalence of specific and overall food allergy in the study population vs. the general population. Children in the study population >2 years of age had a food allergy prevalence of 17.7% and a milk allergy in 12.9%, whereas those <2 years of age had a food allergy prevalence of 11.1% and a milk allergy in 8.5% (Fig 2).
DISCUSSION
Much debate has surrounded food hypersensitivity and its impact on other childhood diagnoses. The link between food allergy and otitis media, as mentioned previously, is still being ascertained. Precedent has been established regarding food allergy and eczema where the ‘skin’ is the target organ. Moreover, food withdrawal has resulted in successful treatment. Eigenmann et al studied the association between food allergy and atopic dermatitis, finding that over one-third of the patients with atopic dermatitis had evidence of food allergy. 5 More recently, Sampson 6 has emphasized the importance of food allergy in atopic dermatitis, discussing that physicians should identify food allergens when patients are young and eliminate them from their diet, with the belief that the condition will improve.
The diagnosis of allergy in children can be especially difficult. Those <2 years of age show lower skin reactivity to histamine, which can complicate the diagnosis. Although some children tolerate prick testing and weekly allergy shots, most do not like the multiple ‘sticks’ needed to evaluate common allergens. Obtaining a blood sample in the operating room can satisfy both child and parent. 7 The ImmunoCAP system™, a fluoro enzymatic immunoassay, quantitatively measures IgE. As noted previously, the CAP system demonstrates a 15% increase in sensitivity over the original RAST system. This increase is due to numerous reasons, including greater binding capacity, quicker time to equilibrium of antigen-antibody reactions, and also combinations of monoclonal and polyclonal anti-IgE antibodies. 6
Utilized with increased frequency in the field of allergy, it is becoming evident through ongoing research that utilizing the CAP FEIA may decrease the need for the current gold standard of diagnosing food allergy: double-blind, placebo-controlled food challenge (DBPCFC). This, in turn, could make the diagnosis of food allergy easier and less time-consuming. Sampson 6 discussed a ‘decision point’ for each allergen concluded that for egg, milk, peanut, and fish the levels of IgE could predict clinically reactivity with >95% certainty. Values were reported in kU (egg, 6 kUA/L; milk, 32 kUA/L; peanut, 15 kUA/L; fish, 20 kUA/L). 1 These numbers, however, can be confusing to the clinician because usual reports are in percentages or classes. For milk, this corresponds to a Class 4. According to Pharmacia Diagnostics Class 4 has a range of 17.5 to <50 kUA/L. 8 Therefore if a patient has a ≥ Class 4 ImmunoCAP result they have a 95% certainty of clinical reaction. False negative testing has beleaguered the view of in vitro testing in physician and patient's opinion. Values <95% decision point should be confirmed with oral challenge because they may still be reactive clinically. 1
In this study, the level of specific IgE in the blood >0.35 kUA/1 was considered significant. Using the alternative scoring method, a positive ImmunoCAP food allergy was documented if the patient had a percentage ≥100%, thus, Class 0 and part of Class 1 was not considered positive for this study. The Alternative Scoring Method increased the sensitivity of our study, but utilizing the ‘decision points’ for each allergen suggested by Sampson may increase specificity for each antigen.
In this IgE analysis, we found approximately a 2-fold increase of food allergy prevalence in the children undergoing an ENT procedure as compared to the general population. A 10-fold increase was noted to cow milk. Although we cannot imply causality between increased food allergy and children requiring ENT procedures, this research suggests that infants and children may benefit from a simple blood test with specific antigen IgE analysis, potentially while under anesthesia for procedures, to help with further management of allergies.
Research has also suggested that after the age of 2, the prevalence of food allergy decreases, however, we found a higher prevalence of food allergy in children >2 years of age vs those younger than 2 (17.7% vs 11.1%, and milk allergy of 12.9% vs 8.5; Fig 2). Our patient population was self selected for ENT problems and may reflect the higher prevalence of food allergy in the ENT population. Further study of pediatric ENT patients compared to ‘normal’ controls would be of great value in interpretation of results.
An extensive discussion between food allergy and food intolerance is beyond the scope of this study. Food allergy, in particular, may involve other cells within the immune system, including cell-mediated immunity and immune-complex reactions, and would have been missed if only using IgE testing. Evidence has shown increasingly that T-lymphocytes may play an important role in food allergy. Testing methods such as patch testing, food allergy-induced cytokine production by T-lymphocytes, and eosinophil and cytokine measurements in stool, have been suggested. 9
CONCLUSION
This prevalence study found approximately a 2-fold increase of food allergy in the children undergoing an ENT procedure as compared to the general population. A 10-fold increase was noted to cow's milk. Although causality can not be implied between increased food allergy and children requiring ENT procedures, this research suggests that children needing ENT procedures may benefit from allergy testing. Further study of pediatric ENT patients compared to other pediatric patients should be done. Diagnosis and management of the underlying etiology of many pediatric ENT problems will make their future management more comprehensive and may prevent need for further surgical procedures.