
Abstract
Obstructive sleep apnea (OSA) is a common disorder affecting an estimated 18 million Americans. The cost of treating OSA is approximately $42 million annually for hospitalization alone in the United States. 1 Uvulopalatopharyngoplasty (UPPP), introduced by Fujita in 1981, has become a common surgical therapy for OSA.
Postoperative monitoring after UPPP has been a subject of controversy. Initially UPPP was generally carried out in conjunction with a tracheotomy and patients were monitored in the intensive care setting postoperatively. Reports by Terris et al 2 in 1997 as well as Mickelson and Hakim 3 in 1998 concluded that routine postoperative ICU monitoring is unnecessary for patients undergoing UPPP. Currently some surgeons advocate at least 24 hour inpatient observation after UPPP. Controversy has shifted recently to whether UPPP can be carried out safely as outpatient surgery. At our institution, virtually all patients undergoing UPPP are scheduled for outpatient surgery. Patients are then assessed in the postoperative period to determine whether they may be discharged home based on adequate oxygen saturation, oral intake, and pain control.
We undertook a retrospective study of patients undergoing UPPP with the objective of establishing the safety of this procedure as outpatient surgery. We sought to determine the postoperative admission rate and characterize the complications in patients undergoing UPPP.
PATIENTS AND METHODS
Institutional review board approval was obtained to review billing records and medical records with the assistance of an honest broker. Billing records were searched for patients undergoing UPPP with or without adjunctive procedures between 2000 and 2004. Adjunctive procedures included tonsillectomy, septoplasty, and supraglottoplasty. Patients with severe cardiopulmonary comorbidity and apnea associated cardiac events were not considered candidates for UPPP. Patients undergoing skeletal surgery or tracheostomy in conjunction with UPPP were excluded. All procedures were carried out by the senior author (J.T.J.). Medical records were reviewed to determine age, gender, height, weight, body mass index (BMI), operative procedures, reasons for postoperative admission, and complications. Preoperative polysomnography data was also collected including respiratory disturbance index (RDI) and lowest O2 saturation. Statistical analysis was carried out using Sigma-Stat 3.1 (Systat Software Inc., Point Richmond, CA). Fisher's exact test and t tests were used in comparing admission rates among groups of patients.
RESULTS
A total of 110 patients (98 males, 12 females) met the inclusion criteria. The average age was 44 years (19 to 71 years). Average RDI was 35 (2 to 103). Average BMI was 32.3 (20.5 to 61.4).
Ninety of 110 (82%) patients were discharged on the day of surgery. Twenty patients (18%) were admitted for observation. Table 1 shows admission rates according to procedure. There were no significant differences in admission rates according to procedure. No patients were admitted to the ICU. In terms of reasons for admission, 3 patients had desaturations, 8 patients had limited oral intake, 3 patients had nausea, and 1 patient was admitted for anticoagulation as he was on warfarin as an outpatient. The reason for admission in 5 patients was not attributable to medical reasons and was likely a transportation issue.
To assess whether patients undergoing nasal with palatopharyngeal surgery were more likely to require admission than those having palatopharyngeal surgery alone, patients undergoing septoplasty in conjunction with UPPP with or without tonsillectomy were compared to those patients undergoing UPPP with or without tonsillectomy. Patients undergoing nasal with palatopharyngeal surgery were significantly more likely to require hospital admission as shown in Table 2 (P = 0.02).
Three patients were admitted due to desaturations in the recovery room. Table 3 shows average BMI, RDI, lowest O2 saturation for these 3 patients compared to averages for the entire cohort. Although the small number of patients experiencing desaturation limits statistical comparison, several observations can be made. The average age and BMI for the patients admitted due to desaturation is similar to averages for the whole cohort. All 3 of these patients had septoplasty in conjunction with UPPP. Also, although 2 of these patients had severe OSA as defined by RDI, 1 patient had an RDI of 22. Lowest oxygen saturation during PSG ranged from 60% to 84%.
There were 25 patients with severe OSA, defined as RDI >50. Five of these patients (20%) were admitted; this is comparable to the overall admission rate of 18%. Six patients had RDI > 90, 2 of whom were admitted due to oxygen desaturation. The majority of patients with severe OSA as defined by RDI had outpatient surgery.
Ten patients (10%) had minor postoperative complications after discharge. Six patients had postoperative bleeding, 3 of which required hospital admission. Other minor complications included urinary retention (1 patient), seizure (1 patient), pneumonia (1 patient), and dehydration (1 patient). Dehydration is the only complication that may have been avoided by postoperative admission. There were no major complications.
Patients admitted and discharged according to procedure
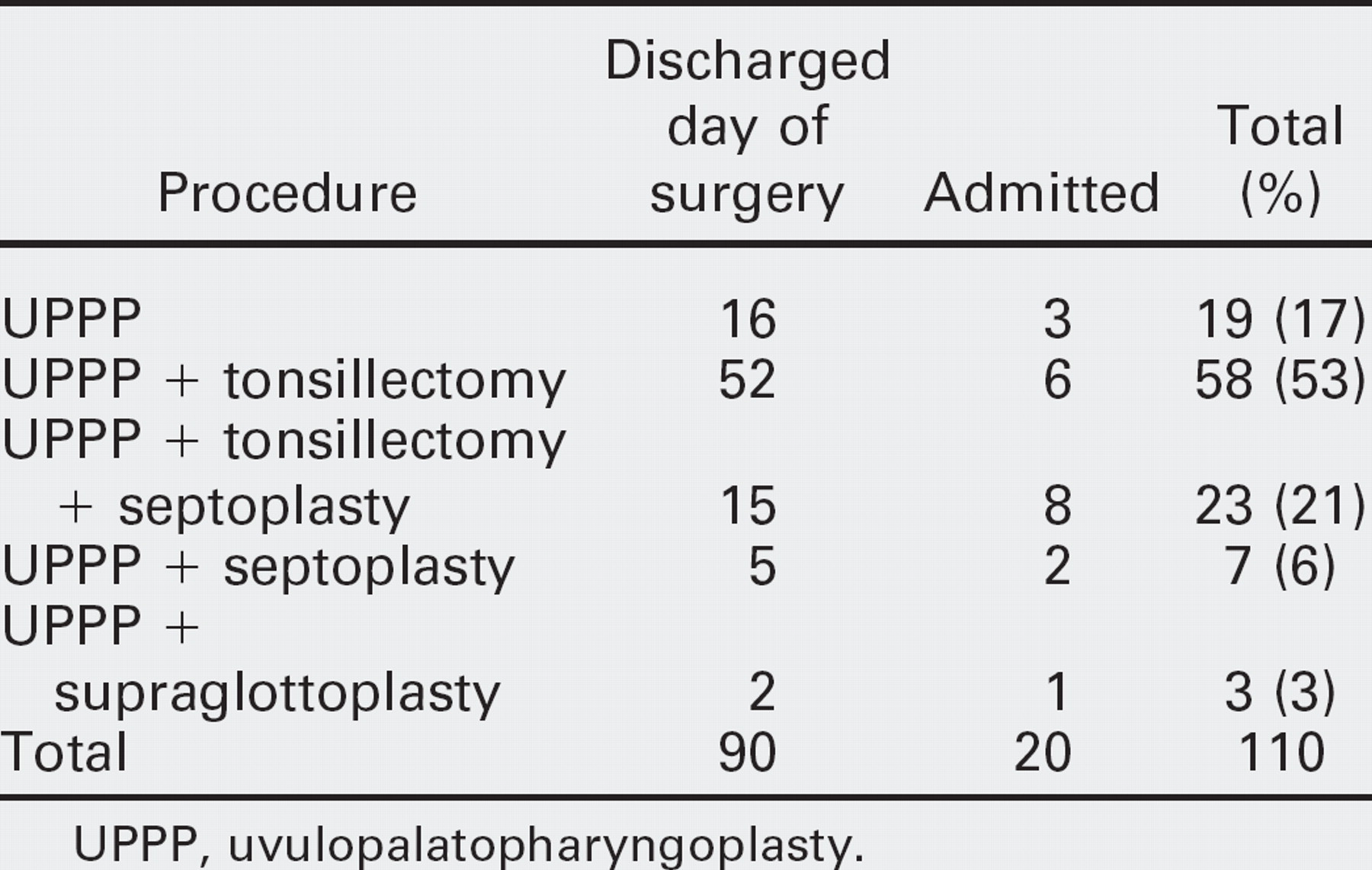
UPPP, uvulopalatopharyngoplasty.
Admission rate in patients undergoing nasal with palatopharyngeal surgery compared with palatopharyngeal surgery alone
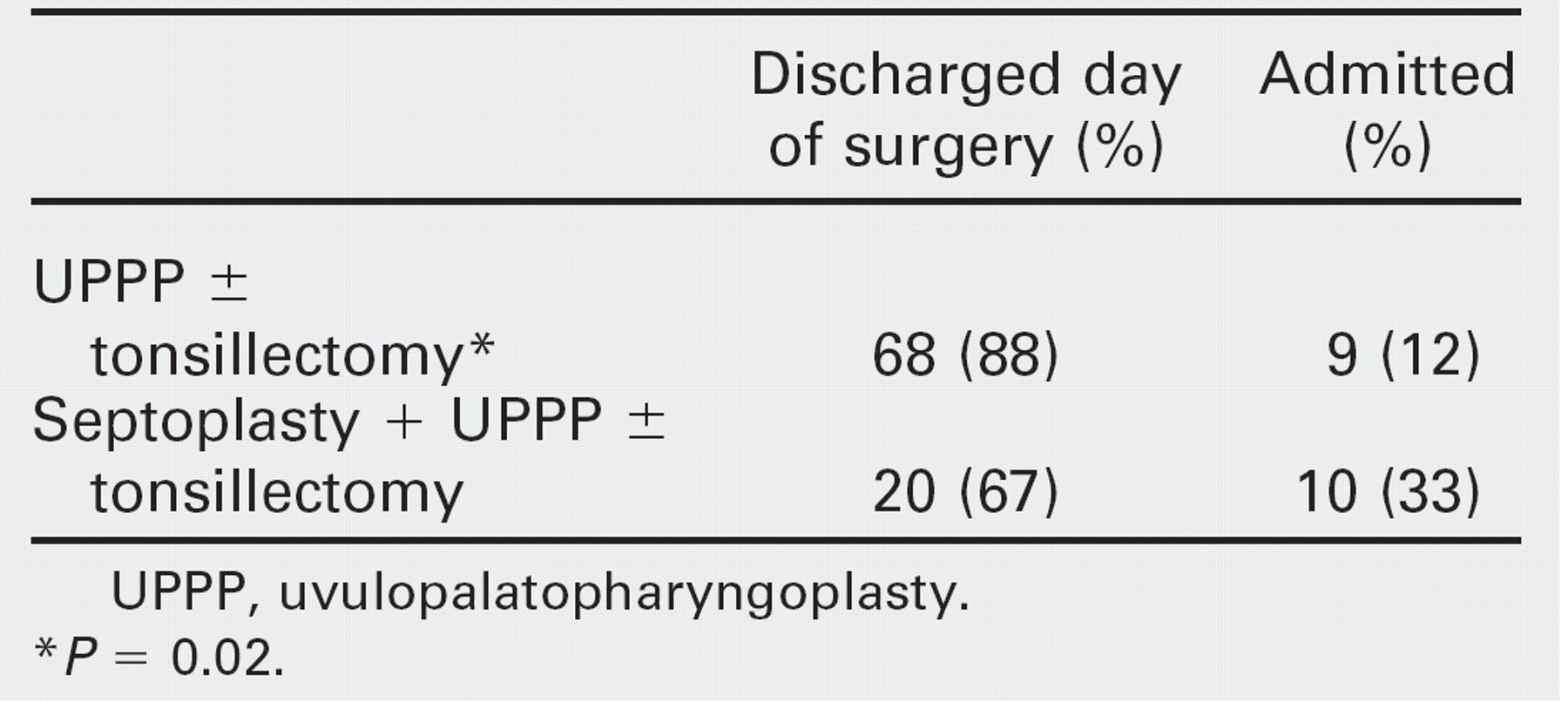
UPPP, uvulopalatopharyngoplasty.
P = 0.02.
Patients admitted due to desaturation
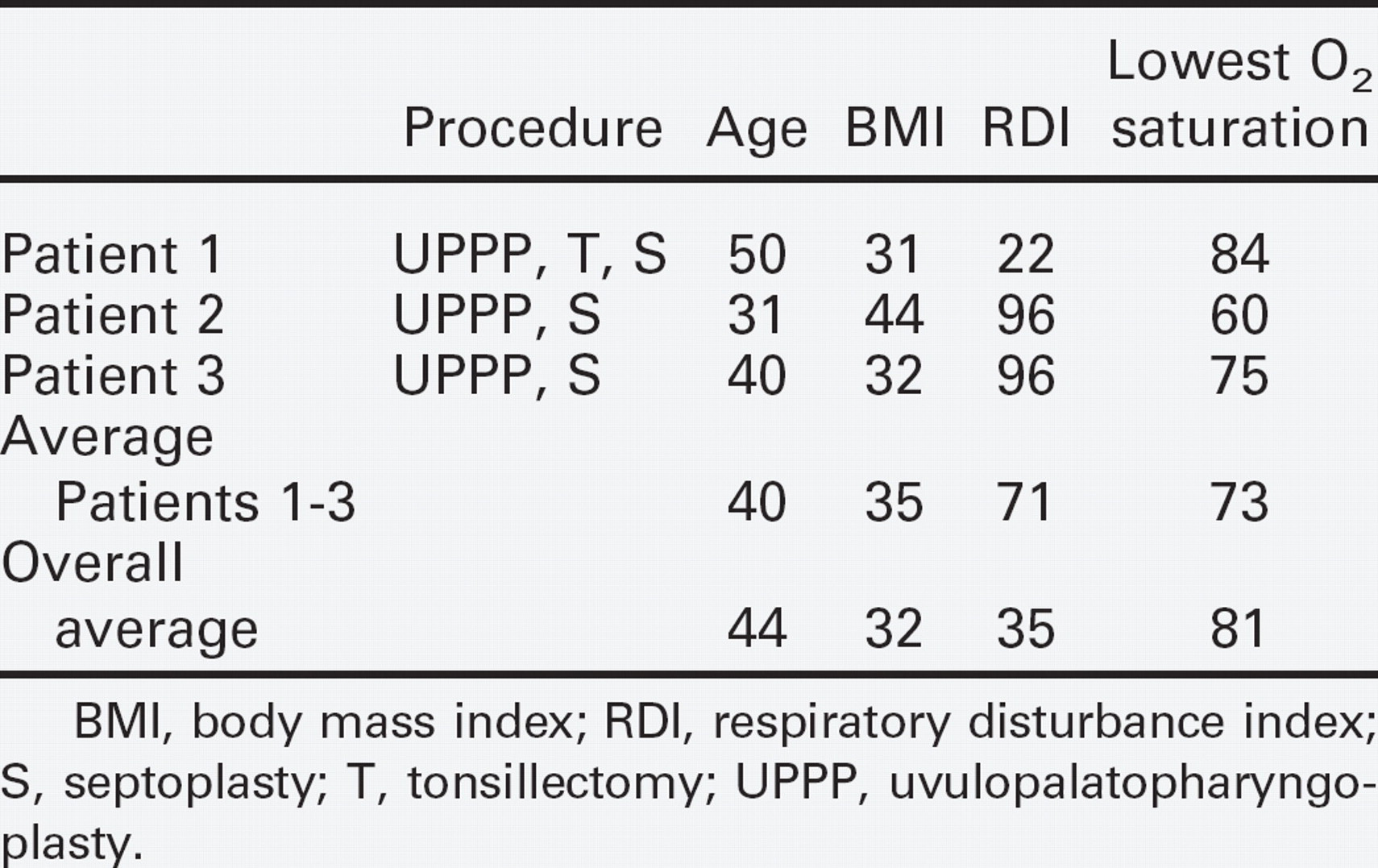
BMI, body mass index; RDI, respiratory disturbance index; S, septoplasty; T, tonsillectomy; UPPP, uvulopalatopharyngoplasty.
DISCUSSION
To our knowledge this is the largest reported series of patients undergoing UPPP with or without adjunctive procedures as outpatient surgery. The majority of patients (82%) were discharged on the day of surgery. We recognize that these patients may desaturate at home as surgery for OSA does not result in an immediate improvement. However, there were no reportable respiratory complications observed in this group of patients discharged on the day of surgery. Also, there were also no significant respiratory complications observed in the patients admitted for observation. Minor respiratory complications, defined as desaturation requiring admission, occurred in 3% of patients in this series.
Multiple authors have examined rates of respiratory complications after UPPP. 4 The definitions of respiratory complications vary widely in these studies with most authors only including major respiratory complications such as reintubation, emergent tracheotomy, pneumonia, and pulmonary edema. Riley et al reviewed 182 patients having surgery for OSA and found that 6 patients desaturated to the upper 80% range in the first 2 postoperative days, 5 which is comparable to the 3% incidence of desaturation requiring admission in our cohort.
Our results suggest that preoperative PSG indices, such as RDI, do not predict which patients may experience oxygen desaturation in the early postoperative period. Only 2 of 25 patients with severe OSA (RDI >50) were admitted due to desaturation in the early postoperative period. Both of these patients had relatively severe desaturation on preoperative PSG with nadirs of 60% and 75% respectively. Conversely, the other patient admitted secondary to desaturation had an RDI of only 22 on preoperative PSG.
We believe that careful preoperative selection is essential in successful UPPP surgery, particularly when carried out in the outpatient setting. That is, patients with severe comorbidities or apnea-related cardiac events are generally not appropriate candidates for UPPP. When these patients are unable to be effectively managed with positive pressure, they should be offered tracheostomy as the minimal procedure. Also, when carrying out UPPP as outpatient surgery, it is important to have an anesthesiologist with experience in managing OSA patients readily available in the perioperative period to closely monitor patients should problems arise. Further, hospital admission after UPPP should always be an option when the surgeon or anesthesiologist deems necessary. These procedures should be carried out at a facility prepared to admit any patient for overnight observation if necessary.
There are recent reports of UPPP carried out as outpatient surgery. Kieff and Busaba retrospectively reviewed 86 patients with OSA who underwent single-stage nasal and palatopharyngeal surgery. 6 Twenty-three of 86 patients met criteria for discharge on the day of surgery that included oxygen saturation of >94% on room air while asleep, no history of cardiopulmonary disease or diabetes mellitus, adequate pain control and oral intake, hemostasis, and normal vital signs. They observed no postoperative complications in those patients discharged on the day of surgery and concluded that same-day discharge is safe for selected patients undergoing combined nasal and palatal surgery. 6
Spiegel and Raval reviewed 117 patients undergoing UPPP with or without adjunctive procedures. 7 Ten of these patients (9%) were discharged home on the day of surgery. In the remaining patients they observed a 4.3% incidence of respiratory complications. The majority of these respiratory complications consisted of oxygen desaturation, which was comparable in severity to that observed during preoperative polysomnography. Two patients had presumed laryngospasm and subsequent pulmonary edema occurring immediately after extubation. They concluded thata2to3 hour monitoring period would detect virtually all significant early postoperative complications. 7
CONCLUSIONS
UPPP can be carried out safely on an outpatient basis. Careful preoperative selection of patients should permit many patients to undergo UPPP as outpatient surgery. Patients with severe cardiopulmonary comorbidity or apnea related arrhythmias are not appropriate candidates for UPPP. Factors requiring admission may be assessed in the early postoperative period. The rate of respiratory events requiring postoperative admission after UPPP is low.