
Abstract
Revision surgery for a cochlear implant has been reported numerous times in the literature, both for adults and for children. From a cursory inspection of published reports, several interesting outcomes emerged. First, the prevalence of implant failure appeared to be higher for children relative to adults. For example, Arnoldner and colleagues 3 found a rate of failure to be 7% for adults and 14% for children in their study sample. Weise et al 2 reported a failure rate of 0.8% for adults relative to 5.4% in children. This difference was attributed to greater chances of impact to the head.
A second finding was that failure rate and revision rate often were not synonymous. Lassig et al 1 reported a failure rate of 3.7% with a revision rate of 5.1%. The difference was attributed to factors not related to device failure per se, but to other complications such as scalp flap problems or upgrades to new technology, among others. Device failures have recently been classified according to whether they are hard or soft. A hard failure is when the device completely stops working, whereas soft failures are intermittent device malfunctions or other device-related problems that result in deterioration in a patient's performance. 4,5
The third finding from published reports indicated that functional performance did not change significantly and, in fact, improved in some cases as a result of revision surgery, 6–10 although some patients were less satisfied with the results 11 or experienced sound quality differences. 12 Moreover, upgrades to newer technology did not always ensure improvements in outcomes, and an adjustment period was typically required. 5
The purpose of the present study was to identify those patients from the House Ear Institute/House Clinic pediatric caseload that required revision surgery for a cochlear implant and to ascertain the reasons for those revisions. Audiological results were compared prior to device failure and following revision surgery to determine clinical outcome. Before presentation of the pediatric data, the histopathology of 2 temporal bones from an adult implant user who underwent revision surgery in each ear is described. The implications of these findings are discussed in terms of potential effects of multiple implant surgeries.
Histopathology: Adult Case Study
Fourteen temporal bones from adult patients with multichannel cochlear implants were identified from the temporal bone collection of the House Ear Institute. Two temporal bones were from a female who underwent revision surgery in both ears. The patient had her first surgery in 1977 with a 20-mm single-channel electrode in the right ear that was revised to a Nucleus 22 multichannel implant in 1991. She was implanted in the left ear with a 3M/House single-channel short electrode (6 mm) device in 1984, which was later upgraded to a Nucleus 24 multichannel device in 1999.
Morphologic evaluation of structural elements including spiral ligament, stria vascularis, hair cells, peripheral processes, and spiral ganglion cells was performed on the 2 temporal bones. The bones were fixed in 10% buffered formalin for 1 month and the electrodes removed. The bones were then decalcified in ethylenediaminetetraacetic acid, embedded in celloidin, sectioned in 20-micron-thick slices, and stained with hematoxylin and eosin. Histopathological analysis determined the percentage of remaining spiral ligament, stria vascularis, hair cells, peripheral processes (dendrites), and spiral ganglion cells for each cochlear turn. The spiral ganglion cells were counted, using an ocular mounted grid, in every tenth section and the total number was calculated using the Konigsmark formula to prevent double counting. Ganglion cell counts were determined by multiplying the summed counts by 10 to account for unmounted sections and by a factor of 0.9 to account for cells that would be doubly counted because of their location on the interface between sections. Segmental spiral ganglion cells counts (segment I to IV) were also represented.
Results
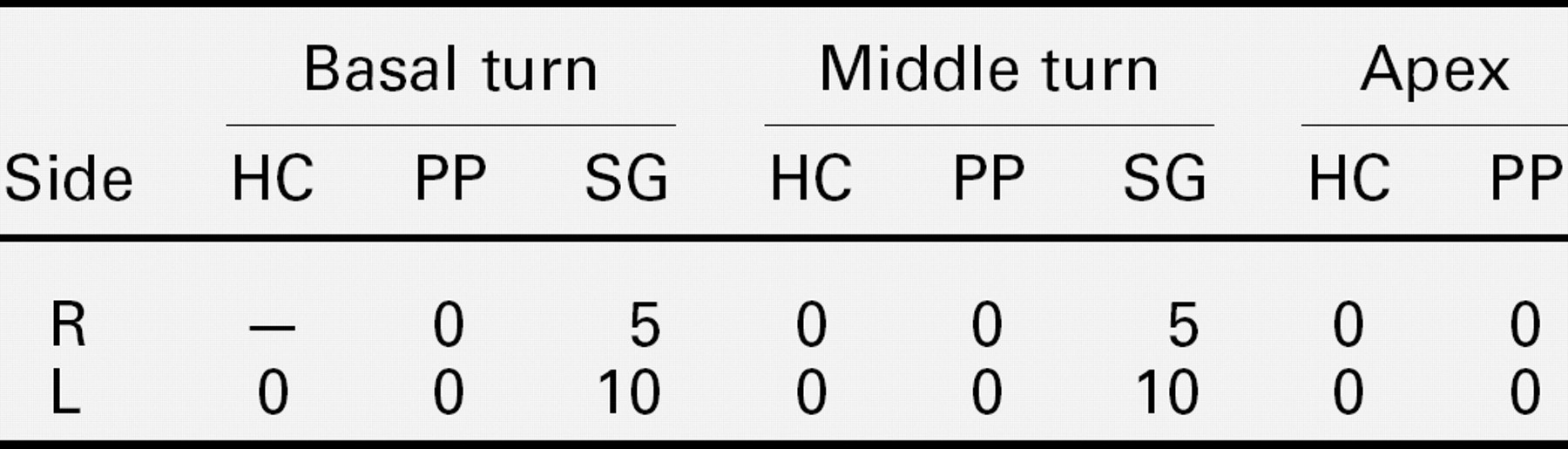
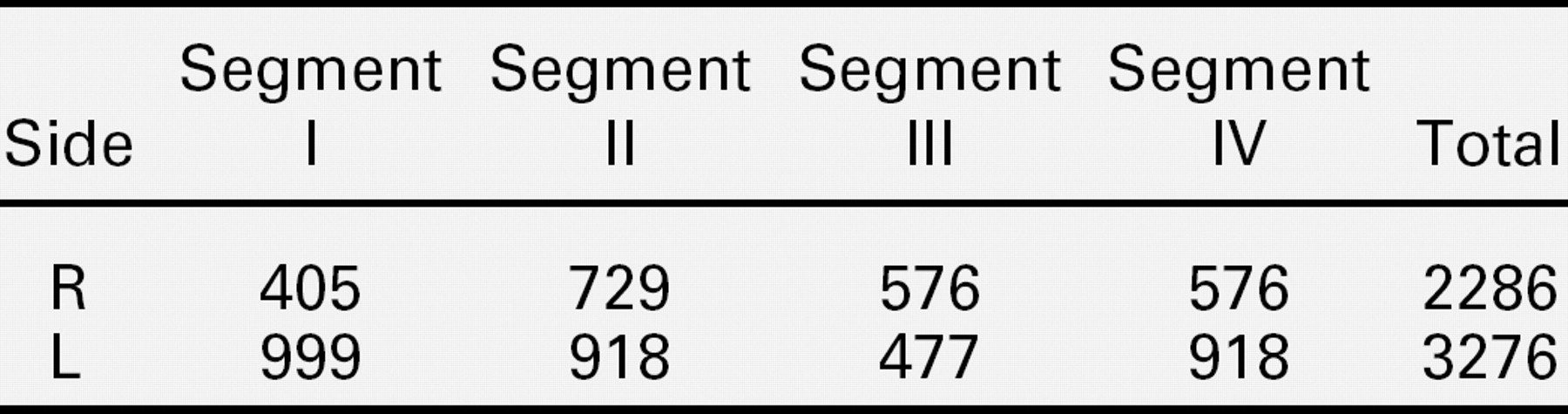
The estimated percent remaining hair cells, peripheral processes, and spiral ganglion cells are shown in table 1, and the actual segmental and total ganglion cell counts are shown in table 2 for right and left temporal bones. Microscopic examination, as seen in Figure 1, showed new bone formation around the electrode path in the scala tympani of the basal turn of the cochlea. The dendrites were absent across from the path of the electrode but also beyond its tip. The spiral ganglion cell count was extremely low in both ears, as shown in Figure 2, and represented less than 10% of the normal spiral ganglion cell population. Despite the low spiral ganglion cell count, the patient derived benefit from the implants with scores of 30% on open-set words and 66% on open-set sentences. Although new bone formation was attributable to trauma during both initial and revision surgery, it was not responsible for the severe degeneration of the neural elements in this pair of temporal bones.
Estimated percent remaining hair cells (HC), peripheral processes/dendrites (PP), and spiral ganglion cells (SG) for R and L side

Spiral ganglion cell counts for 4 cochlear segments and total spiral ganglion cell count for 2 implanted temporal bones
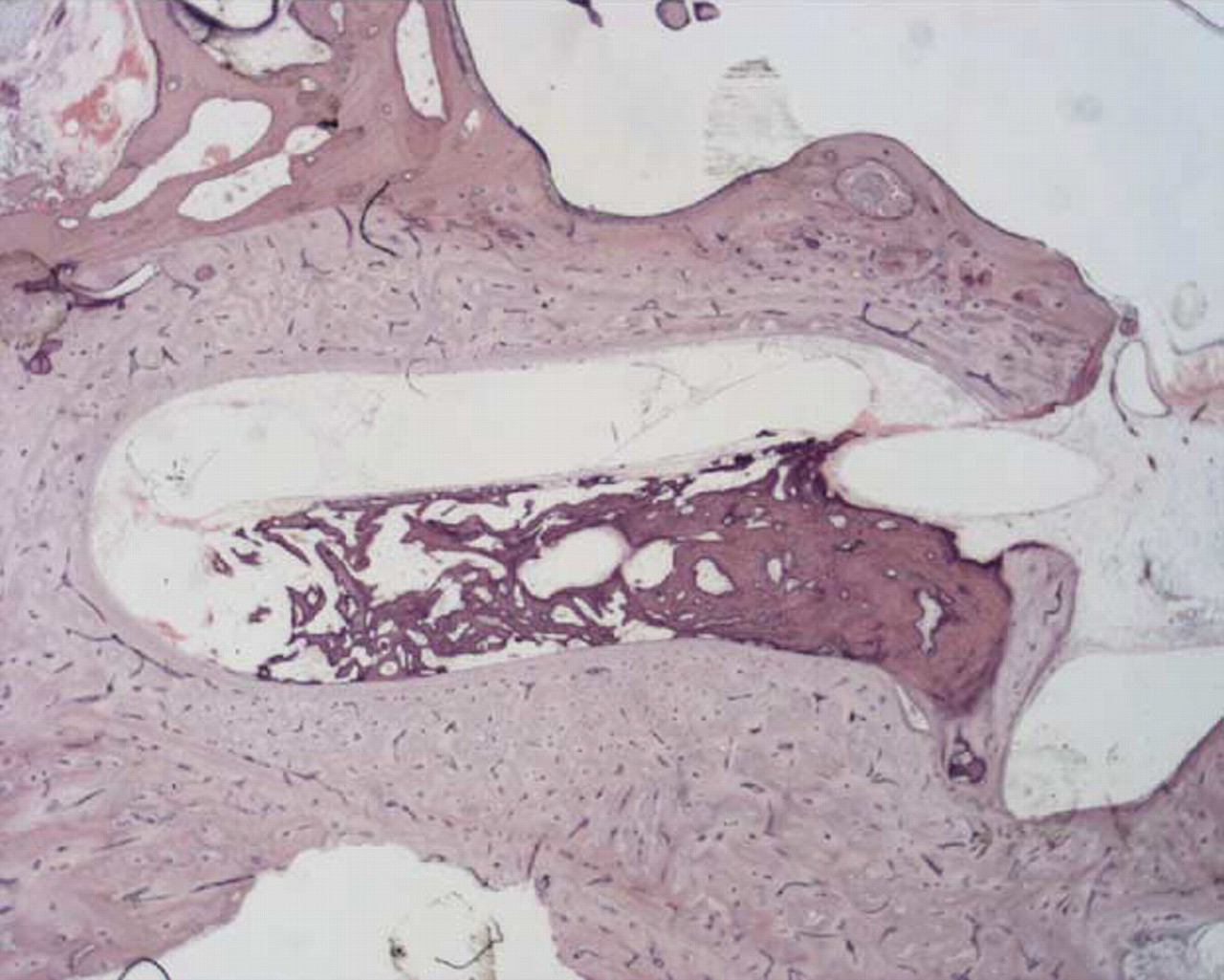
Path of electrode is seen within the scala tympani surrounded by new bone formation.
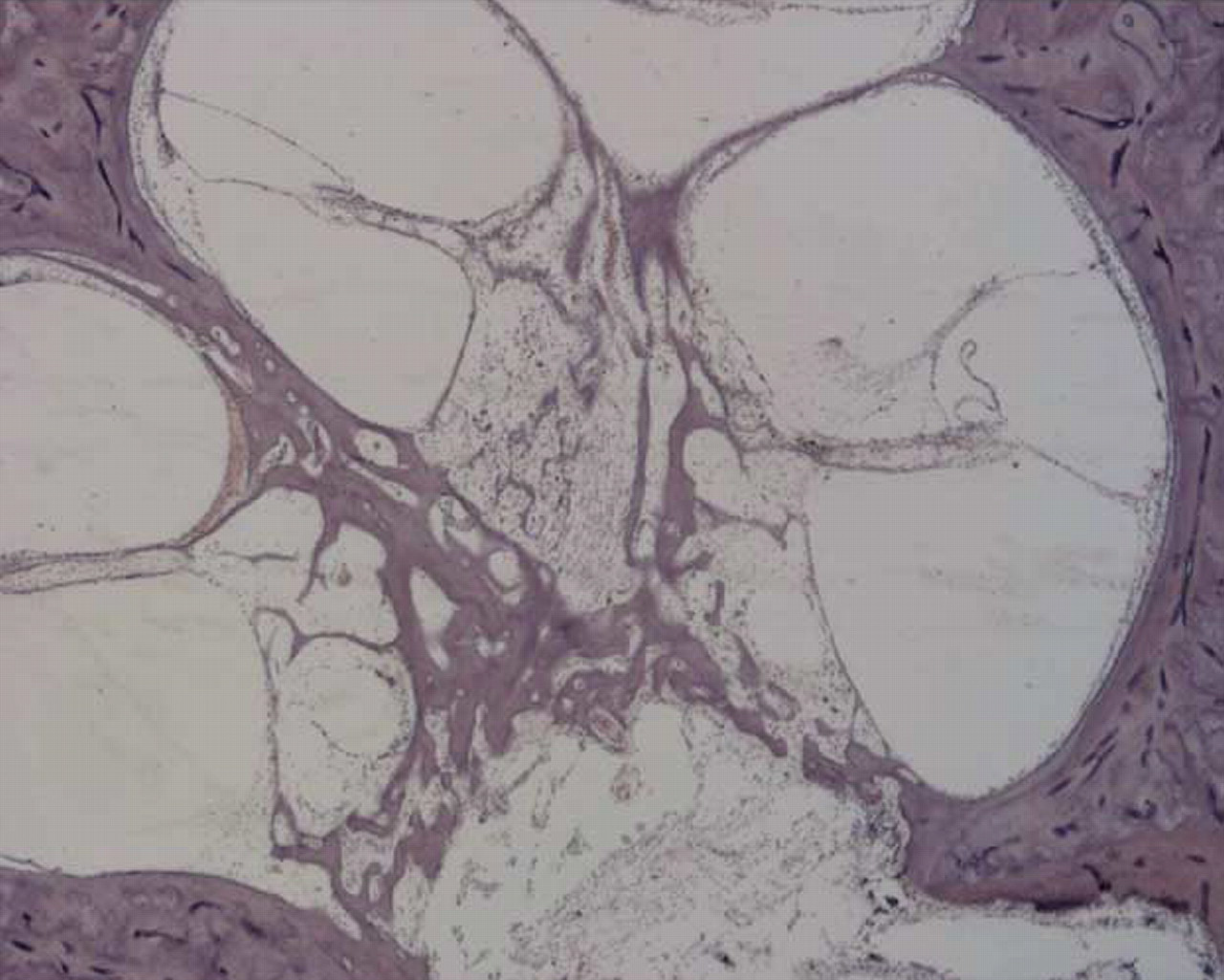
No inflammatory or bony reaction beyond the basal turn of the cochlea. Severely reduced spiral ganglion cell count.
Examination of the entire series of 14 bones with multichannel implants revealed different degrees of surgical trauma. In some cases, the reaction to implantation was minimal. Specifically, round window insertion was atraumatic and the electrodes were located completely within the scala tympani of the basal turn surrounded by a fibrous sheath that sometimes contained round cells and some inflammatory cells. Invariably, there was damage to the spiral ligament, the stria vascularis, and organ of Corti at the junction between the descending and ascending basal turn of the cochlea in some bones. In that precise location, the electrode frequently passed from the scala tympani to the scala media and sometimes into the scala vestibuli, following the path of least resistance. There also was fracture of the osseous spiral lamina in that location. 13,14
It is notable that when the periosteum is violated, it is usually followed by new bone formation around the electrode. However, in the pair of temporal bones from this single case who underwent revision surgery, there were surviving spiral ganglion cells despite the absence of dendrites and new bone formation. Spiral ganglion cells were seen across from the electrode path, even when dendrites were completely absent. Results from these analyses show that there are no deleterious effects from revision surgery on the surviving spiral ganglion cells. Recent reports have not shown clear positive correlations between spiral ganglion cell counts and clinical performance. 15
STUDY DESIGN AND SETTING
Patient Demographics
Retrospective chart review was approved by the Investigational Review Board at St. Vincent Medical Center in Los Angeles. From a total of 496 children implanted between 1987 and the summer of 2005 at the House Ear Institute/House Clinic, 28 children (17 males and 11 females) with multichannel cochlear implants required some form of revision implant surgery (5.6% overall revision rate). Their ages at time of the original implant ranged from 16 months to 13 years, 1 month, with a mean of 4 years. For the remaining demographics, data are reported for 27 of the 28 children, as one female moved out of the area and was lost to follow-up. The duration of time between the first surgery and the revision surgery ranged from 2 months to 6 years. The mean age at time of revision was 6 years, 5 months, and ranged from 1 year, 6 months to 15 years, 9 months. Five children received their first cochlear implant at other centers.
Of the 27 cases requiring revision surgery, 16 cases were congenitally deaf. Within this subgroup, 2 children were identified as having a family history of deafness, 2 had progressive hearing loss, and was 1 was deaf from maternal rubella, and the 11 remaining were of unknown origin. Of the 11 cases not diagnosed as congenital, 5 were deafened following meningitis. One child was born premature and was in the neonatal intensive care unit (NICU) for 7.5 months. According to parent report, this child was given ototoxic drugs while in the NICU. Four children had malformations of the cochlea, and 1 child was diagnosed with Goldenhar Syndrome.
Clinical Assessment Measures
The pediatric speech recognition battery used at the House Ear Institute is extensive, taking into consideration children's chronological age, developmental age, and functional hearing abilities. For the present analysis, results are reported from the measures that provided the most complete data for this sample of children; however, not all children were tested on every measure. These measures included soundfield thresholds for warble tones (250, 500, 1000, 2000, and 4000 Hz), Mr. Potato Head task—words and sentences, 16 Glendonald Auditory Screening Procedure (GASP)—words and sentences, 17 and the Test of Auditory Comprehension (TAC). 18
The Mr. Potato Head task is a modified open-set test that uses objects from the Mr. Potato Head toy kit to assess auditory comprehension of words and sentences. The task is presented live voice at conversational-level speech. The GASP is an open-set test consisting of word recognition and sentence comprehension, which also is presented live voice. The TAC is a closed-set, recorded task that assesses auditory comprehension of environmental sounds and speech in a hierarchy of 10 subtests. Subtest 10, the most difficult, asks the child to recall 5 details of a story in competition. The TAC is presented at 50 dB HL in a calibrated sound-field.
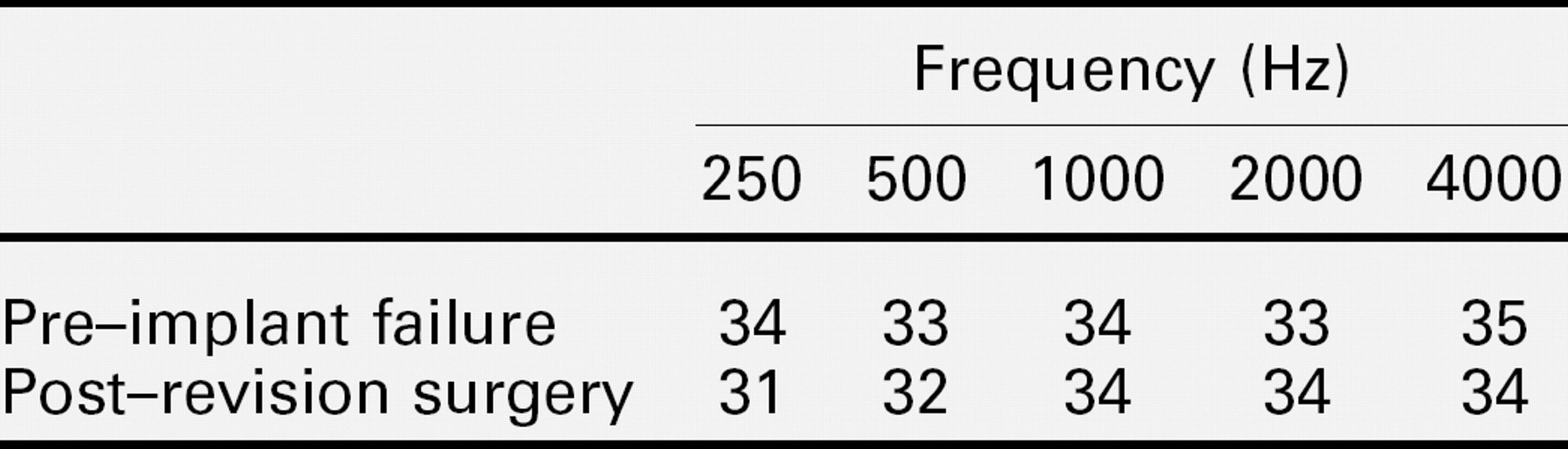
Mean soundfield thresholds (re: dB HL) with cochlear implant activated before implant failure and after revision surgery
RESULTS
Revision Surgery
Of the 27 patients requiring revision surgery, 18 patients underwent explantation of the original device and reimplantation in the same ear with a new electrode from the same manufacturer as the original (3.6% reinsertion rate). Sixteen of those 18 cases had their original surgery at the House Ear Institute/House Clinic (3.2% House reinsertion rate). Fourteen of the 18 cases were identified as experiencing device failure, of which 2 were Nucleus 22, 2 were Nucleus 24, 7 were Clarion CI, 2 were Clarion CII, and 1 was MedEl Combi-40+. One case required revision surgery because of infection (Nucleus 24). Two cases underwent revision because of head trauma (Clarion CI and CII), and one because of a cracked casing (Clarion CI).
The remaining 9 revision cases were not reinsertions. One was explanted due to infection but was not reimplanted, and 2 experienced surgical complications that necessitated revision surgery without reinsertion. In the first case, the child developed a cerebrospinal fluid (CSF) leak approximately 6 months after the original cochlear implant surgery. Upon return to surgery, a leak around the electrode was discovered entering the cochlea at the round window and was repaired. The leak reoccurred after 7 days and a lumbar spinal drain was surgically placed. This child experienced no further complications and the device was not removed. The second case underwent revision surgery 6 years after the original cochlear implant surgery because of a soft failure, ie, the patient's performance suggested a technical problem with the internal device (Clarion CI). During revision surgery, the surgeon encountered difficulty advancing the new electrode into the pathway of the previously placed electrode and there appeared to be an obstruction in the scala tympani. When removing the obstruction, CSF leak occurred. Due to the combination of CSF leak and malformation of the inner ear, it was decided to close the flap and implant the opposite ear. No further complications occurred. Four additional cases underwent implantation in their opposite ears. After thorough evaluation, in one patient, who did not receive her first implant at the House Ear Institute, it was decided to perform a second surgery to upgrade to a newer device in the opposite ear. Two cases required removal of the implants because of problems with wound healing, and new devices were implanted on the opposite side. One patient requiring 2 repositioning surgeries as a result of migration of the internal receiver was ultimately reimplanted in the opposite ear. Lastly, 2 cases that experienced infections underwent wound debridement without explantation.
Mean speech perception results before cochlear implant failure and after revision surgery
PHW, Mr. Potato Head task—words; PHS, Mr. Potato Head task—sentences; GASP-W, Glendonald Auditory Screening Procedure—words; GASP-S, Glendonald Auditory Screening Procedure—sentences; TAC, Test of Auditory Comprehension.
Audiology
Results were analyzed only for the children who required reinsertion surgery. Shown in table 3, the mean soundfield thresholds (obtained with implants activated) indicated no change between pre–device failure and post–reinsertion surgery. The greatest difference was 3 dB for 250 Hz. Paired t tests confirmed that differences did not reach statistical significance. It must be emphasized that soundfield thresholds are a reflection of how the processor is adjusted by the audiologist, so equivalence between pre–device failure and postreinsertion is not analogous to psychophysical equivalence (ie, electrical threshold and comfort levels across electrodes). Soundfield thresholds, however, do convey detection of sound in the environment. The clinical implication of these findings was that the same levels of audibility were able to be maintained.
Mean scores on speech perception tests are shown in table 4. The data indicated no significant change in performance from pre–device failure to post–revision surgery, as verified by nonparametric statistics (Wilcoxon signed ranks test). No individual patient stood out as having markedly different scores between the 2 test intervals. On the livevoice open-set tests (Mr. Potato Head and GASP), mean scores reflected moderate to high levels of performance of speech identification and comprehension. On the closed-set recorded TAC, the mean score of 4.75 (pre–device failure) and 5.08 (post–reinsertion surgery) demonstrated that this group of children were identifying single nouns (level 4) and recalling 2 critical elements within a sentence (level 5).
DISCUSSION
Revision surgery for a cochlear implant will be necessary in a small but significant percentage of children. It has been our clinical experience that approximately 3% to 5% of children will require revision, in agreement with other clinical reports. Revision surgery is performed without difficulty for the majority of cases and children generally maintain or improve upon the same level of performance as pre–device failure. Nevertheless, this type of surgery remains challenging, particularly for those cases where an electrode cannot be placed in the original site. There also are cases that may never approach prerevision levels of performance with the newly implanted device. This difficulty is further compounded by the fear of inflicting additional intracochlear damage that potentially could result in additional loss of residual spiral ganglion cells, the neural elements that are electrically stimulated by the implant.
In our series, all revision patients received new devices from the same implant manufacturer; the devices were either the same model or upgrades to a newer model. However, in other clinical series 6 device crossovers did occur, which didn't affect performance outcomes. Although the final decision is that of the parents, our preference is to stay with the same implant manufacturer even though the same depth of insertion may not be achieved during revision surgery.
On the strength of histopathological analysis of temporal bones from one adult who underwent 2 revision surgeries with reinsertion of new electrodes, there is no evidence to suggest that additional degeneration of spiral ganglion cells occurred. Other histopathological support for this finding comes from another series of implanted temporal bones in which implant bones were compared to their corresponding contralateral, nonimplanted bones. 13 No significant differences were found between implant and nonimplant bones on spiral ganglion cell counts and neural survival, ie, peripheral processes. In certain bones there was increased bone formation within the scala tympani that was due, in our opinion, to electrode insertions that traumatized the endosteum of the basal turn. There also were bones with minimal reaction to the presence of the implant. Revision cochlear implant surgery should be performed with the same utmost level of caution as the initial surgery in terms of electrode insertion trauma. 19,20
In order to maximize reinsertion of the new electrode while minimizing trauma during revision surgery, it would be helpful to leave the original electrode within the cochlea as a stent until the new electrode is ready to be inserted. Precautions should be taken to prevent tissue from collapsing into the cochleostomy site and obscuring its location. In addition, a wide facial recess should be made for better visualization. The surgeon should be prepared when reorienting the internal receiver to perform a full revision surgery lest the electrode become dislodged while manipulating the receiver. Lastly, adequate instrumentation should be available to clean the scala tympani or to drill new bone formation.
In the majority of our pediatric patients who required revision surgery with insertion of a new electrode, clinical performance was essentially the same as before, in agreement with numerous other studies. Previous publications have emphasized that a significant number of patients, up to 30%, may not reach their preoperative clinical performance. 11 Patients should be counseled accordingly, especially those high-performing “star” patients who usually have the most to lose.
CONCLUSION
Revision cochlear implant surgery is technically feasible. At some point, every implant surgeon will face the reality that a small percentage of children will require revision surgery. If medically indicated, this surgery should be performed as soon as possible so that children are able to progress with minimal disruption to their auditory and speech/language development.