
Abstract
EBM rating: C-4
Immunotherapy has been shown to be an effective method for the treatment of inhalant allergy. The use of desensitization protocols for treating allergic rhinitis can be traced to their initial use in the early 20th century. 1 Over the last 75 years, several different methods have been developed to assess the presence of allergy, and these methods have been used in guiding the preparation of immunotherapy treatment sets. Broadly, these testing methods can be grouped into in vivo methods, through direct challenge of the patient with a suspected antigen, and in vitro methods, in which the serum or tissue of the patient is assessed with a laboratory test.
In vivo tests can be further classified into several different methods. The 2 most commonly used techniques recommended for the assessment of inhalant allergy are percutaneous tests, such as prick testing, and epicutaneous tests, such as intradermal testing. 2 In addition, testing methods can be classified as qualitative, in which the information obtained from the testing is primarily an assessment of the presence or absence of sensitivity to a specific antigen, and quantitative, in which an attempt is made to assess not only the presence of allergy, but the degree of sensitivity to each specific antigen. Traditionally, quantitative testing has involved an intradermal method known as skin endpoint titration, or SET, in which fivefold dilutions of antigen are used for testing, and the placement of sequentially more concentrated antigen onto the skin is used to determine the degree of sensitivity, known as the endpoint. 3 The advantage of quantitative testing in the delivery of immunotherapy is that it permits the use of more concentrated antigens to initiate treatment. Immunotherapy based on qualitative testing alone must employ very dilute concentrations at the outset to assure safety, since the precise level of antigen sensitivity has not been assessed. The safety of immunotherapy based on quantitative testing has been demonstrated to be excellent. 4
In the past several years, blended methods for assessing the degree of sensitivity have been developed that maintain the principles of quantitative testing yet are more efficient than previous techniques. One such method, modified quantitative testing or MQT, has been utilized successfully and continues to offer a clinically useful technique for the assessment of allergy and the initiation of immunotherapy. 5 MQT uses a blend of percutaneous and intradermal methods to estimate the degree of allergic reactivity in a similar manner to SET, yet involves less material, expense, and testing time. A recent study demonstrated an excellent degree of concordance with concurrent skin testing results obtained using SET and MQT methodologies. 6
While the precise mechanism through which immunotherapy is able to effect change in symptoms and immune function is not fully understood, it has been shown to be an efficacious technique for the treatment of inhalant allergy. Immunotherapy has been demonstrated to bring about changes in both immunoglobulin and cytokine levels, and to therefore have effect on both B and T lymphocytes. 7 After the initiation of immunotherapy, immunoglobulin E (IgE) levels have been shown to rise slightly, followed by a drop in IgE levels and a concurrent rise in levels of the IgG4 subclass of immunoglobulin G (IgG). 8 This “scissors effect” has been well described, although the rise in IgG4 levels using standard techniques is often not appreciated for more than 1 year following the initiation of immunotherapy. The increase in IgG4 levels with immunotherapy has suggested that it may play the role of a “blocking antibody,” decreasing the inflammatory effects promoted by IgE. A recent study suggests that changes in serum IgG4 levels to cat antigen can be noted as early as 5 weeks following the initiation of immunotherapy, and that these changes are predictive of response to immunotherapy at 1 year. 9
In addition, immunotherapy has been noted to have profound effects on T-lymphocyte function. 10 The initiation of immunotherapy creates a shift in the population of T helper cells from the pro-allergic Th2 orientation to the Th1 orientation. This shift is demonstrated through the decreased expression of the Th2 cytokines IL-4 and IL-5 and an increase in the Th1 cytokines IL-2 and IL-12. 11,12 While these immune modulations are noted to accompany the administration of successful immunotherapy, they are often not seen for at least 1 year after the initiation of treatment. 9
One of the observations that some clinicians have made through experience with various testing methodologies is that patients treated with immunotherapy based on quantitative techniques such as SET have a more rapid improvement in symptoms than those treated with immunotherapy based on qualitative testing alone. The hypothesis that is suggested by these clinicians is that higher concentrations of antigen can be safely delivered at the outset of therapy using quantitative testing since patient tolerance has been demonstrated through sequential testing of various antigen concentrations. While immunotherapy based on qualitative testing often uses antigen concentrations in the range of 1:1,000,000 weight to volume, quantitative testing can often permit the initiation of immunotherapy with antigen concentrations in the range of 1:12,500 or greater. The ability to deliver much higher amounts of antigen earlier in the course of therapy has been offered as an explanation for the observed rapidity of effect with quantitative techniques. 7 Even using quantitative methods, however, clinical change can often require 3 to 6 months, or even greater, to become apparent. 13
Despite these consistent observations, however, there has not been any research that would support the clinical and immune changes that would presumably occur with quantitative testing. If clinical change can be seen in patients within 3 months, as is often suggested by clinical observation and anecdote, this change should be demonstrable objectively, both through improvements in quality of life and in immune mediators. The present study was designed to assess these clinical and immunomodulatory effects using an accelerated approach to immunotherapy based on the quantitative testing technique MQT. The hypothesis of this study is that patients treated with immunotherapy over 12 weeks using MQT-based treatment would demonstrate objective changes in both immune mediators and quality of life.
METHODS
Subjects
Sixteen adult patients were recruited into this study from the clinical patient base of University Otolaryngology, P.C., the faculty practice plan associated with the Wayne State University School of Medicine.
Procedure
All patients who entered this study had a clinical history of perennial allergic rhinitis for at least 2 years. This diagnosis was confirmed clinically by the attending physician. Patients then underwent skin testing for inhalant allergy using the standard MQT protocol as described elsewhere. Patients were eligible for study if they were allergic to at least 1 of 3 perennial antigens by MQT: Dermatophagoides pteronyssinus (Der p1), Dermatophagoides farinae (Der f1), or cat dander (Fel d1). They were permitted to have positive skin testing for other perennial and seasonal allergens as well. If they met study criteria, they were then enrolled into the study. The study method and procedure were approved by the Human Investigation Committee (HIC) of Wayne State University. The study was conducted and consent obtained through this HIC-approved protocol.
Means and (standard deviations) for physiological measures
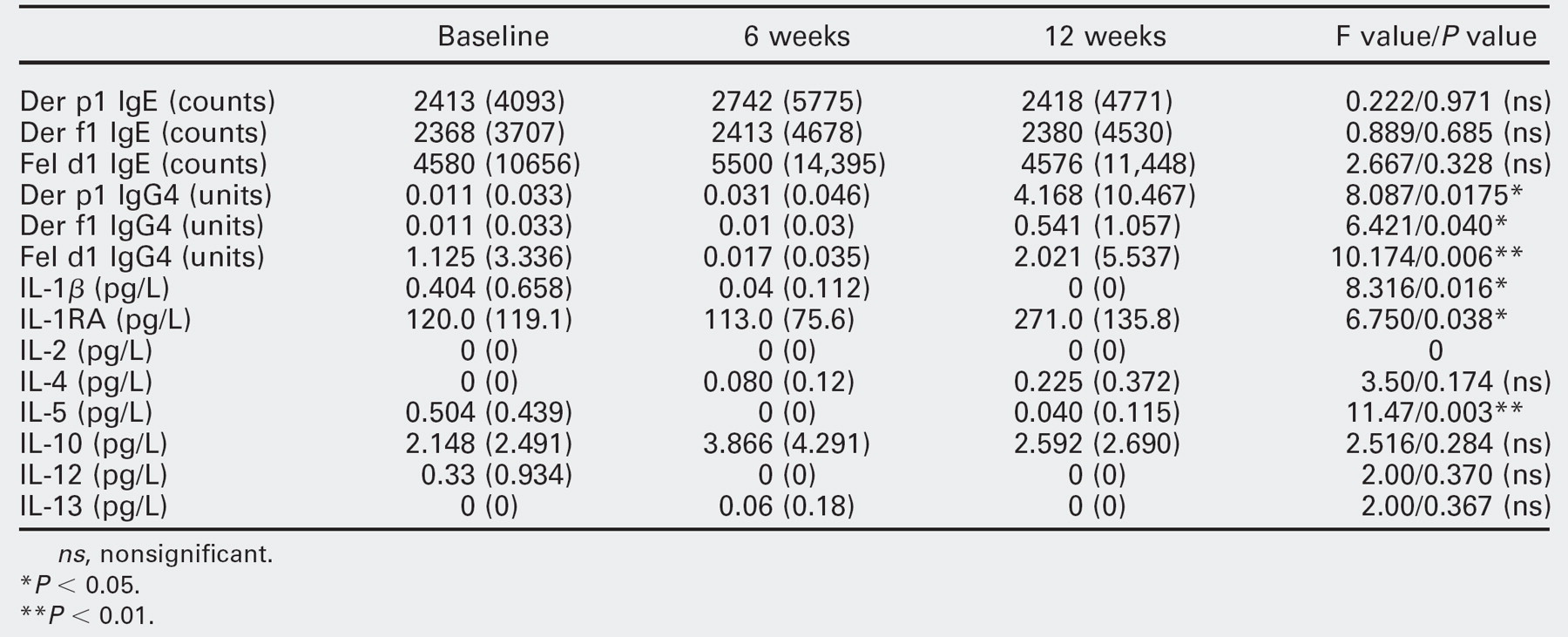
ns, nonsignificant.
*P < 0.05.
** P < 0.01.
Subjects then completed 3 quality-of-life and symptom measures in the office: the 20-item version of the Sino-Nasal Outcome Test (SNOT-20), 14 the Allergy Outcome Scale (AOS), 15 and the Rhinosinusitis Disability Index (RSDI). 16 They were then sent to have blood drawn for evaluation of immune mediators. These mediators included the specific immunoglobulins IgE and IgG4 for Der p1, Der f1, and Fel d1, and the cytokines interleukin 1p, IL-2, IL-4, IL-5, IL-10, IL-12, and IL-13 and interleukin 1 receptor antagonist (IL-1RA). Immunoglobulin levels were sent to MRT Laboratories (Hackensack, NJ) for analysis, and cytokine levels were sent to the University of Maryland Core Cytokine Laboratory (Baltimore, MD) for analysis. Handling of serum specimens was managed according to protocols recommended by the prospective laboratories.
After these outcome measures were completed, the subjects had immunotherapy treatment vials prepared based on quantitative endpoints derived from the MQT protocol. They then began immunotherapy on an accelerated basis, receiving weekly injections that were started at 0.1 cc of the initial treatment sera and advanced by 0.1 cc per week over 12 weeks. No patients demonstrated systemic or significant local reactions to the administration of immunotherapy in this manner. Subjects were allowed to continue their medications in the usual manner for symptom control over this period.
Subjects then completed outcome measures at both 6 weeks and 12 weeks following the initiation of immunotherapy. They completed again the 3 quality-of-life and symptom measures and had blood drawn for immunoglobulin and cytokine analysis. After 12 weeks, their participation in the study was completed. Subjects did not receive any monetary honoraria for participation, but they did have all immunotherapy and related care provided without cost during this period.
RESULTS
Of the 16 subjects who began the study, 7 terminated therapy within the first 4 weeks. Nine subjects, therefore, completed the entire 12-week course of immunotherapy. Of these 9 subjects, 1 did not complete the 12-week assessment measures. The final outcome analysis, therefore, is based on 8 subjects. No subject experienced adverse local and/or systemic reactions. Means and standard deviations were calculated as summary statistics. Friedman's nonparametric analysis of variance (ANOVA) was used for inferential analysis and probability calculations. 17
The mean age of the final 9 subjects was 38 years, and there were 6 female and 3 male subjects that completed the study. While IgE levels remained constant over the 12-week course of the study, levels of IgG4 increased significantly at 12 weeks in all 3 perennial antigens assessed, Der p1, Der f1, and Fel d1. In addition, significant declines were noted at 12 weeks in IL-1p and IL-5, with a concurrent significant increase in IL-1RA at 12 weeks. No changes were noted in IL-2, IL-4, IL-10, IL-12, or IL-13. Summary statistics and probability values are noted for these variables in Table 1.
In addition to the changes noted in the above immune mediators, positive changes were observed in both the AOS and the RSDI. There was a significant decline in symptom scores on the AOS at 12 weeks. In 2 of the 3 subscales of the RSDI, the emotional and functional subscales, significant improvements were noted as well at 12 weeks. No changes were noted in the physical subscale of the RSDI or in the SNOT-20, although changes in SNOT-20 scores approached statistical significance over time. Summary statistics and probability values for these variables are presented in Table 2.
Improvement in both symptom scores and immune indicators was seen in the majority of subjects within the 12-week period of the study. Of the 8 subjects with complete data sets, 7 demonstrated improvement in both AOS and RSDI subscales and 6 demonstrated decreased levels of IL-1β and IL-5 and increased levels of IL-1RA. Only one individual experienced no clinical or immunologic change after 12 weeks of immunotherapy.
Means and (standard deviations) for psychometric measures
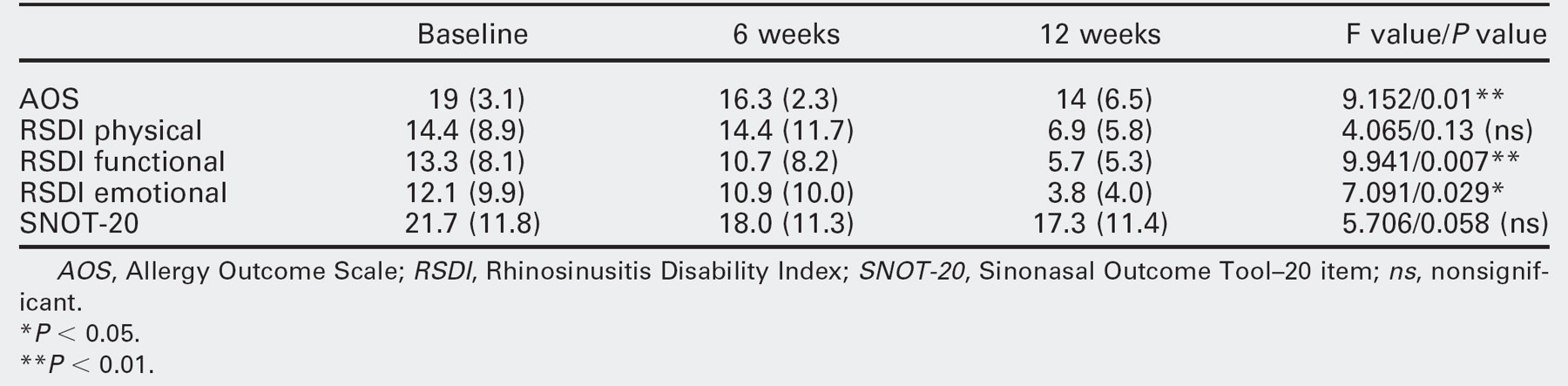
AOS, Allergy Outcome Scale; RSDI, Rhinosinusitis Disability Index; SNOT-20, Sinonasal Outcome Tool-20 item; ns, nonsignificant.
*P < 0.05.
** P < 0.01.
DISCUSSION
The provision of immunotherapy based on quantitative testing using MQT and delivered through an accelerated schedule of dose escalation was demonstrated to promote changes in immune mediators and quality-of-life measures within 12 weeks of the initiation of therapy. These changes reflect both physiological and symptomatic improvement in relevant parameters among subjects with allergic rhinitis. The presence of these significant changes over time supports the hypothesis of this study, that MQT-based immunotherapy can generate changes in both immune mediators and quality-of-life and symptom measures over a relatively short period.
Otolaryngologists have noted rapid improvement in patient symptoms using quantitative testing methodologies such as SET. Despite careful clinical description and anecdotal experience, objective evidence supporting these observations has been limited. The ability to deliver concentrated antigen in a safe manner should theoretically promote rapid change in both immune mediators and symptomatic assessments. The present study supports the robustness of quantitative testing in generating significant physiological and symptomatic improvement through documented and significant modulations within 12 weeks. It provides evidence to confirm clinical observations of the efficacy of immunotherapy based on quantitative testing principles.
In addition, the present study confirms the utility of MQT as a quantitative testing methodology for inhalant allergy. MQT endpoints were used successfully in this study to direct immunotherapy that was delivered safely through an accelerated protocol and resulted in rapid physiological and symptomatic change. The improvement in subject-rated symptoms was confirmed by corresponding modulation of immune mediators, both of which demonstrated significant improvement within 12 weeks. Immunotherapy based on MQT, therefore, appears to be a safe, efficient, and highly efficacious method of promoting improvement in symptoms and immune function among patients with inhalant allergy.
In addition to the group changes noted in this study, the ability to measure immune changes easily among patients with allergic rhinitis may allow physicians to objectively assess the progress of patients receiving immunotherapy. Changes in immunoglobulin and cytokine profiles may offer an objective serological measure that can be used to determine whether an allergic individual is having the desired response to therapy. Further research is necessary to confirm the utility of these markers as reflecting response to immunotherapy among individual patients.
CONCLUSION
The administration of immunotherapy based on quantitative testing using MQT and delivered through an accelerated protocol demonstrates significant changes in immunoglobulin and cytokine levels by 12 weeks following its initiation. In addition, positive changes in symptom and quality-of-life measures are also demonstrated by 12 weeks. These findings support the rapid onset of physiological and symptomatic improvement with MQT-based treatment of inhalant allergy.