
Abstract
EBM rating: C-4
In a significant number of patients, episodes of sometimes aggressive but nonproductive coughing continue, despite not only exhaustive workup of all of these possibilities, but also the use of a variety of empiric treatments, eg, antibiotics, steroid inhalers, cough suppressants, and proton pump inhibitors. Having not resolved spontaneously or in response to treatment over months or even years, such patients may be consigned to a permanent coughing problem, with sometimes devastating effects on eating, sleeping, social events, and even ordinary telephone conversation. The percentage of patients with cough who fit this description is reported to be as high as 31% in one prospective study. 4
Numerous therapeutic interventions have been tried in patients with idiopathic chronic cough. Examples include over-the-counter antitussive medications, centrally acting antitussives (opioids and nonopioids), nebulized topical anesthetics/steroids, antireflux regimens, and behavioral cough control techniques. 5–7 Unfortunately, when all of these approaches fail, there appears to be no remaining treatment option for chronic idiopathic cough. In this article, we describe our experience with a group with this problem and report on a new potential therapy for patients with chronic idiopathic cough.
MATERIALS AND METHODS
This study is a prospective uncontrolled cohort study of patients seen at the outpatient clinic of an academic referral laryngologic practice (Loyola University Medical Center, Maywood, IL, and Loyola Voice Institute). The treatment protocol used for these 12 patients did not differ from standard treatment offered to such patients both before and after this cohort. Records were maintained in compliance with HIPAA requirements and with IRB approval. Patients constitute a consecutive series of individuals who seek help for chronic cough and who fulfill all prior clinically established criteria for sensory neuropathic cough (Table 1, also see Description of Entity below). All patients were seen and treated by the principal author (RWB). All patients in this cohort had previously undergone extensive work-up elsewhere, including but not limited to: exclusion of smoking and use of ACE inhibitors; ENT evaluation excluding for post nasal drip; pulmonology consultation that included chest x-ray and pulmonary function test with metacholine provocation testing and sometimes bronchoscopy; and exclusion of acid reflux by proton pump inhibitor (PPI) empiric treatment and sometimes esophagogastroduodenoscopy or pH monitoring. After complete information was given and informed consent was obtained, all patients were treated with a single dose of open label 10 mg of amitriptyline at bedtime for 21 days. Patients' responses were evaluated by single nurse phone calls on days 2, 7, and 20 of treatment and again at least 20 days after discontinuation of treatment. Evaluations included subjective assessment of improvement by the patients themselves, their report of percentage of reduction of the symptoms, time to maximal effect, residual response on discontinuation of the drug, and recording of side effects. Patients were asked to rate their cough reduction (improvement) on a 0% to 100% scale during and after cessation of treatment. Note that the number of study subjects precludes assessment of statistical significance in the results section.
Proposal for diagnostic criteria in chronic sensory neuropathic cough
BACKGROUND
The idea that this patient population might be experiencing a neuropathic cough arose because of 3 patients who presented some years ago at nearly the same time. The first patient had been followed for several years for her larynx cancer; she spoke of her difficulties with postherpetic neuralgia after a severe bout of Herpes zoster oticus. Her pain had responded somewhat to amitriptyline, started by a colleague. The second patient presented with a 1-year history of episodic and abrupt unilateral severe burning sensation low in her throat. Given its neuralgia-like character, she was somewhat skeptically begun on amitriptyline, with excellent benefit. The third patient was seen soon thereafter, with the typical cough described in this article (subsequently understood to be neuropathic) over many years' duration. Empirically treated with amitriptyline, this patient also responded dramatically to a low dose of amitriptyline.
RESULTS
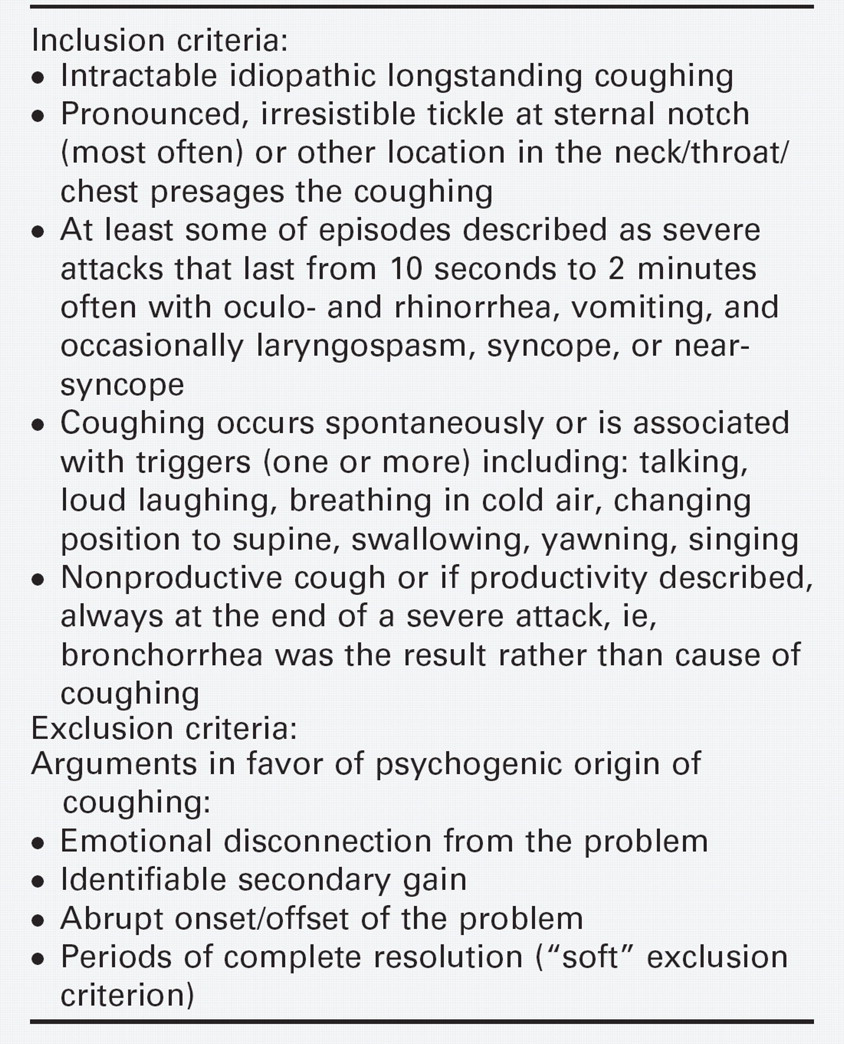
Each patient treated for idiopathic cough seemed to share the following criteria (also summarized in Table 1): each had been referred because of a longstanding intractable coughing, each lacked a definable cause of cough despite extensive work-up, and each had experienced no beneficial effect to exhaustive lists of empirically initiated treatments. In addition, a pronounced irresistible tickle most commonly at the notch of the sternum typically presaged the coughing. At least some of the episodes were described as severe attacks that lasted from 10 seconds to 2 minutes often with oculo- and rhinorrhea, vomiting, and occasionally laryngospasm, syncope, or near-syncope. (In unusually severe cases seen both before and after this cohort, patients may report a history of rib fracture or subconjunctival hemorrhage). Though each bout of coughing might seem to begin spontaneously, more often it seemed to be triggered by such things as talking, loud laughing, breathing in cold air, changing position, swallowing, yawning, singing, or touching a specific place on the neck (Table 2). The cough was typically nonproductive. If described as “productive” this was always at the end of a severe attack, ie, bronchorrhea as a result rather than cause of coughing. In addition, patients showed no signs of psychogenic cough identifiable by nonorganic indicators including: emotional disconnection from the problem, definable secondary gain, and abrupt onset/offset of the coughing syndrome with periods of complete resolution.
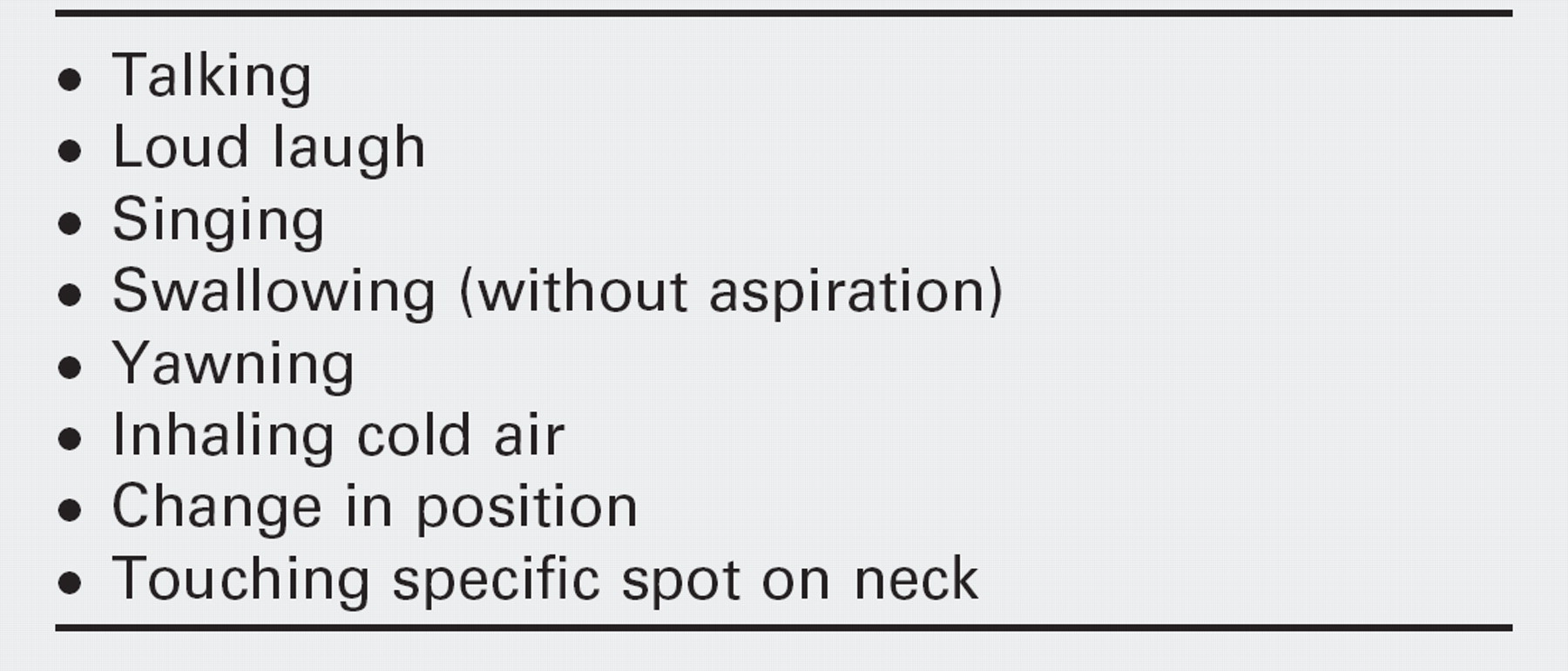
Common triggers for sensory neuropathic cough
The cohort treated consisted of 12 (4 females) consecutive patients. Median age was 52 (range, 20 to 75 years). All patients fitted the abovementioned criteria and had a chronic debilitating cough for a median duration of 24 months with no response whatsoever to a variety of medications that always included at least: antibiotics, asthma inhalers, and proton pump inhibitors. All patients were treated on amitriptyline 10 mg 2 hours before bedtime for 21 days.
Table 3 summarizes the response to amitriptyline. All patients except 1 had prompt significant reduction of their cough with this treatment. The patients reported an average maximal improvement of 75% (range, 10% to 100%). Four (33%) patients experienced complete relief of symptoms and 1 patient reported 95% resolution of his cough. Patient number 12 had only a 10% response to treatment despite 3 months of treatment at increasing doses of amitriptyline (but subsequently responded well to gabapentin with durable benefit for the past 5 years). There appeared to be no significant relationship between duration of the cough and response to amitriptyline. In this cohort, a maximum benefit was observed after a median of 5 days (range, 1 to 10 days). Two patients (2 and 7) had a decline in their response during the initial 3-week protocol. However, both of these patients still retained enough of a response to motivate them to continue with the medication for the entire 3 weeks. Six (75%) of 8 evaluated patients had a sustained clinical response more than 20 days off treatment. No side effects attributable to amitriptyline occurred in this small cohort of patients on this 10 mg dose.
DISCUSSION
Chronic cough is often a true diagnostic challenge and puts a big burden onto patients. Although several causes have been well described, a significant proportion of patients remain with no clear diagnosis. Alternatively, they are diagnosed with asthma or acid reflux, but ongoing treatment for these entities fails to provide any discernible benefit. All patients in this cohort underwent extensive work-up that excluded traditional causes of cough. In addition several other empiric treatments had failed.
Chronic cough was included as one manifestation of the irritable larynx by Morrison et al. 8 More recently, Lee and Woo 9 have described cough as a possible sign of laryngeal sensory neuropathy. Two earlier reports mentioned cough among other symptoms as a postviral laryngeal nerve disturbance. 10,11 As also suggested by these earlier publications, cranial sensory neuropathy may provide a useful new category of thought to apply to patients with chronic undiagnosed or refractory cough. Other terms that might be applied include cough paresthesia, dysesthesia, and neuralgia. The term cranial neuralgia refers to various distinct pain syndromes in the head and neck that result from sudden and excessive discharge from the involved nerve. Neuralgic pain appears to result from a lowered threshold and/or exaggerated response to stimuli. Trigeminal, glossopharyngeal 12–14 and postherpetic neuralgias have been well described. On the other hand, vagal neuralgia has been less well documented, and where mentioned is reported as a pain syndrome, usually not a cause of coughing. These other head and neck neuralgias typically present with characteristic lancinating pain in the affected nerve's distribution. 15,16 The idea of sensory neuropathic cough can be thought of by analogy. The actual source of the neural discharge in each of the above circumstances is not well explained. We speculate that a vagal neuralgia could manifest as a sudden and exaggerated, but nonpainful sensation that the vagus nerve normally mediates—a bogus tickle that leads to uncontrollable coughing. The idea is that the threshold for initiation of a cough reflex is significantly lowered. Thus, a strong, irresistible signal to cough could result from minimal stimuli, or perhaps no stimulus at all.
Summary of therapeutic response to amitriptyline
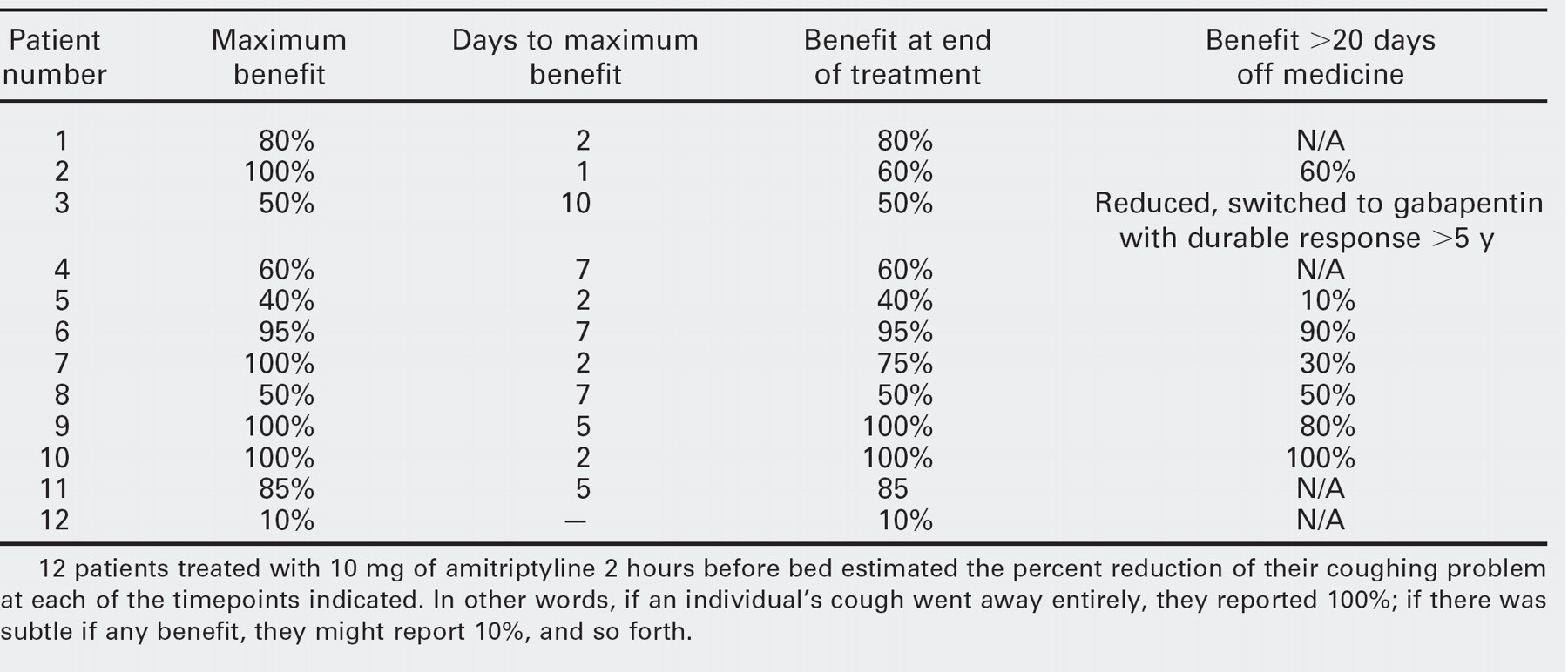
12 patients treated with 10 mg of amitriptyline 2 hours before bed estimated the percent reduction of their coughing problem at each of the timepoints indicated. In other words, if an individual's cough went away entirely, they reported 100%; if there was subtle if any benefit, they might report 10%, and so forth.
A prominent characteristic of neuralgia is the presence of trigger phenomena. A patient with trigeminal neuralgia, for example, may note that touching a particular place at the corner of the mouth triggers intense pain. Another, with glossopharyngeal neuralgia, may report that swallowing triggers the throat pain. Interestingly, several of the sensory neuropathic cough patients also described trigger phenomena. A number mentioned that talking tended to bring on coughing, eg, “I talk for a minute or two on the phone, start coughing, and just have to hang up.” Another, a professional singer, experienced an intense tickling sensation followed by paroxysms of coughing whenever he tried to sing. Yet others have mentioned the triggering effect of inhaling cold air in the wintertime or of changing body position as when lying down to sleep at night. Other patients reported their cough being triggered by yawning or swallowing saliva without evidence of aspiration.
Sensory neuropathic cough, as defined here, appears to respond well to amitriptyline. Amitriptyline is the best-studied tricyclic antidepressant (TCA). In addition to its role in the treatment of depression, it has been used in lower doses in the management of chronic pain syndromes and neuralgias. 17,18 The mechanism of action of the analgesic effect has been related to its serotonin activity and receptor-reuptake inhibition. 19 Because of the pharmacokinetics of this medication, the time required for full effectiveness has been shown to be quite variable, sometimes requiring up to 6 weeks. 13,19–21 Overall, TCAs are considered to be safe, especially when used in low doses. Some side effects, rarely seen with the low doses used in these patients, include its sedative effects, anticholinergic effects, and potential to cause postural hypotension.
The guidelines we used for amitriptyline administration were borrowed from experience in its use for chronic pain syndromes. Thus, a low dose of 10 mg at night was used. The time required to peak clinical effect is known to vary. This was somewhat the case also for cough. Although most noticed benefit within a week, our experience is that a trial should encompass 3 weeks before final assessment of benefit. In this series of patients, the median duration of maximum effect was 5 days. This is somewhat in contrast with the usual time to response in other indication for which amitryptiline is used. At this moment it is unclear at what level amitryptiline may interfere in the cough reflex. However, recent pain literature suggests that amitryptiline has a quick and long-acting nerve-blocking effect superior to that of a classic local anesthetic. 23 We postulate that amitryptiline lowers the sensory treshold of the afferent nerve endings hereby inhibiting the cough reflex.
As noted in the results, 2 patients had a decline in response while still on the amitriptyline, which suggests a tolerance to the medication. This phenomenon is also consistent with the literature about the use of amitriptyline in chronic pain syndromes. 21,23,24 In these cases, the dosage may be increased. It will be interesting to see if an increased dose would re-establish a higher response rate in these patients. In addition some patients have had a durable cough-free period after cessation of the amitriptyline. The available literature that describes amitriptyline use in other neuralgias and pain syndromes does not seem consistent with this finding. Other patients, however, may need treatment on a permanent basis.
We agree that a placebo response cannot be excluded, but given the very high and durable response rate in most patients (inconsistent with the placebo effect as usually seen), the very long duration of the symptoms, and the multiple other treatments tried without benefit, this seems unlikely. However, larger controlled studies with longer-term follow-up are warranted to confirm our findings.
Another objection might be that the cough was abolished or diminished via the psychotropic effects of amitriptyline. In the light of a major experience we have had with nonorganic voice (psychogenic aphonia) and breathing (pseudo-asthma) problems, we find psychogenic cough to be easily distinguished from neuropathic cough. Our caseload includes not only several hundred with SNC, but also a large population with psychogenic cough, primarily in teenagers. The latter entity is typically easily taken care of with behavioral treatment.
The work reported here represents our early short-term experience with amitriptyline for sensory neuropathic cough. In a caseload of at least another 300 cases of sensory neuropathic cough treated both before and after this study cohort, we have learned that minimal responders and those with more severe symptoms respond better to increased dose levels of amitriptyline, to other neurologic drugs used in neuropathies, eg, gabapentin, as also shown by Lee and Woo, 9 or by use of oxcarbazepine or pregabalin.
CONCLUSION
Chronic noninfectious cough is a common disruptive condition. This article describes our experiences with sensory neuropathic cough, a diagnosis that may be considered after thorough exclusion of other potential causes. Open label use of a low dose amitriptyline in a prospective cohort appears to provide surprising benefit in most patients. 22,25
We are indebted to Ms Elga Heintzen, RN, for invaluable help with the telephone interviews and collection of all the data.