
Abstract
Objective
To devise an effective postoperative analgesic protocol.
Study Design and Setting
Two consecutive groups participated in this study. In the first group (n = 100), the pain-control management was pro re nata (PRN). In the second group, (n = 109) we tailored a procedure-specific pain-control protocol for each patient according to the level of pain recorded in the first group. These patients were treated with analgesics given at predetermined hours. Pain was evaluated by using a verbal scale of 1 to 10.
Results
In the first group, a significant reduction in the level of pain was monitored 1 hour after PRN drug administration; however, patients reported the return of pain several hours later, after the drug effect subsided. Overall, the patients suffered a substantial level of pain during the entire postoperative period. In the second group, significant reduction in the level of pain was recorded throughout the hospitalization.
Conclusion
The PRN protocol is not adequate for management of pain after head and neck surgeries.
Significance
We can substantially reduce our patients' postoperative pain by adopting a procedure-specific analgesic regimen instead of a PRN regimen.
The technical development of craniofacial, skull-base, and reconstructive surgery has had a major positive impact on the long-term survival of patients with tumors in those anatomical areas. These procedures, however, involve a considerable level of pain during the early postoperative period. 3 Numerous studies have assessed pain issues in oncological patients during the last decade, 4 but the levels of pain after head and neck surgery in general and craniofacial or skull-base procedures in particular have not been systematically evaluated. Although many analgesic regimens are available (eg, pro re nata [PRN], scheduled dosing, and intravenous patient-controlled analgesia [IV-PCA]), little is known about the optimal therapeutic modality for the treatment of acute postoperative pain after head and neck procedures.
The aim of this study was to assess the level of pain in patients undergoing oncological head and neck surgeries and to develop a protocol to best treat pain during the early postoperative period. To this end, we performed a prospective, nonrandomized study designed to estimate the analgesic efficacy of a PRN protocol, which had been used in our institute as a basic pain treatment regimen. We performed an observational study of PRN patients and then used these results to design a procedure-specific pain-control regimen using scheduled dosing of nonsteroidal anti-inflammatory drugs (NSAIDs), IV-PCA, and tramadol or morphine in patients recovering from head and neck surgery.
Materials and Methods
The perioperative data of all patients who underwent excision of head and neck tumors in our tertiary care, university-affiliated medical center between May 2003 and May 2004 were included in our data analysis. Patients who suffered from specific drug intolerance were excluded from the study. All protocols were approved by the institutional Helsinki committee.
The nursing staff and treating physicians provided the patients with details about our plan for treating their pain after surgery. The patients were asked to estimate their pain by using a verbal scale of 0 to 10 (0 = none, 1-2 = mild, 3-5 = moderate, 6-8 = severe, 9-10 = worst imaginable). Pain was evaluated before as well as 3 times a day after the operation, for a period of up to 7 days. If the patient received a PRN pain-control medication, the level of pain was estimated before and 1 hour after administration of the drug.
Analgesic Protocols
All patients in our department received treatment for their pain, each group according to a specific protocol. In the first group (PRN), analgesics were administered only “as needed” if the patient asked for them or if the nurses felt it to be necessary. This group included patients undergoing maxillofacial or mandibular osteotomies (n = 9), skull-base surgery (n = 10), major neck surgery (ie, neck dissection, partial glossectomy, or laryngectomy, n = 15), and patients undergoing minor neck surgeries (ie, submandibular gland excision, thyroidectomy, neck biopsy, parathyroidectomy, and parotidectomy, n = 66). This treatment regimen consisted of an NSAID (diclofenac 75 mg intramuscularly or orally or rofecoxib 50 mg). As a second line, meperidine, 1 mg/kg intramuscularly (50-100 mg intramuscularly) repeated every 3 to 4 hours if required, but not exceeding a maximum of 150 mg as a single dose, or morphine, via slow intravenous injection (4-10 mg, titrated according to effect), was administered.
In the second group (n = 109), an analgesic protocol was tailored according to the results of the first study. These patients were administered specific drugs at predetermined times, irrespective of the pain they reportedly experienced. They were allocated to 1 of 4 specific drug protocol groups according to the type of surgery. These groups included patients undergoing maxillofacial or mandibular osteotomies (n = 16), skull-base surgery (n = 6), major neck surgery (n = 30), and minor neck surgeries (n = 57). All these patients received an NSAID in the morning before their operation and medications according to the following protocol.
For maxillofacial or mandibular osteotomies, IV-PCA with morphine (1-mg bolus) was administered during the first 3 postoperative days, followed by an NSAID once daily for 4 days. The PCA device was programmed to deliver 1-mg bolus doses of morphine, with a 10-minute lockout interval and no basal infusion. Tramadol was used as PRN treatment during this period, and a single starting dose of 50 mg (20 drops) was prescribed (40 drops, 100 mg/mL). If the desired analgesic effect was not achieved within 30 to 60 minutes, an additional 20 drops were administered. The total daily dose did not exceed 400 mg of tramadol (equivalent to 160 drops or 4.0 mL). A downward adjustment of the dose and/or prolongation of the interval between doses were carried out for the elderly. For skull-base and major neck surgeries, NSAIDs were administered once daily and PRN tramadol 50 to 100 mg. For minor neck surgeries, an NSAID was administered once daily. There was no significant difference in the anesthetic technique (ie, premedication, preoperative and intraoperative narcotic usage, and postoperative ventilation management) between the 2 groups.
Statistical Analysis
Statistical analysis was performed by using Microcal Origin version 5.0 (Northampton, MA). Data are expressed as mean values ± SD. Demographic data and efficacy of different pain-control regimens were analyzed and compared by using analysis of variance. A P value < 0.05 was considered to be statistically significant and a P value of 0.06 to 0.1 of borderline significance. The level of pain (y-axis) was plotted against time (x-axis) and an exponential decay function y = A-x/t was fitted to the graph, where A is the amplitude and t is the decay constant. The area under the curve (AUC) that represents the integral of the level of pain throughout the 7-day postoperative period was estimated from the exponential decay curve fitting. Statistical comparison was performed between groups and included the average level of pain during the 7 days (mean), time to reduction to half the level of pain (t0.5), and the integral of the level of postoperative pain (AUC).
Results
A total of 209 patients were enrolled in this study. The demographic data of the 2 protocol groups are shown in Table 1. A total of 100 patients (mean age 51 ± 18 years) received our PRN pain-control protocol, and 109 patients (54 ± 16 years) received pain-control medication specific to their surgical procedure. The types of surgical procedures are listed in Table 2. There was no significant difference in age, gender, type of surgery, or length of hospital stay between the 2 groups.
Preoperative Pain Evaluation
Pain was evaluated in 100 patients scheduled for oncological head and neck surgery 1 day before their operation. Nine patients reported that they were suffering from levels of pain varying from 1 to 7 on a scale of 0 to 10, with a duration varying from 1 to 24 hours per day and from 1 to 7 days per week. Five of these 9 patients had maxillofacial tumors and reported using an NSAID or dipyrone for pain control.
Demographic data of the study population
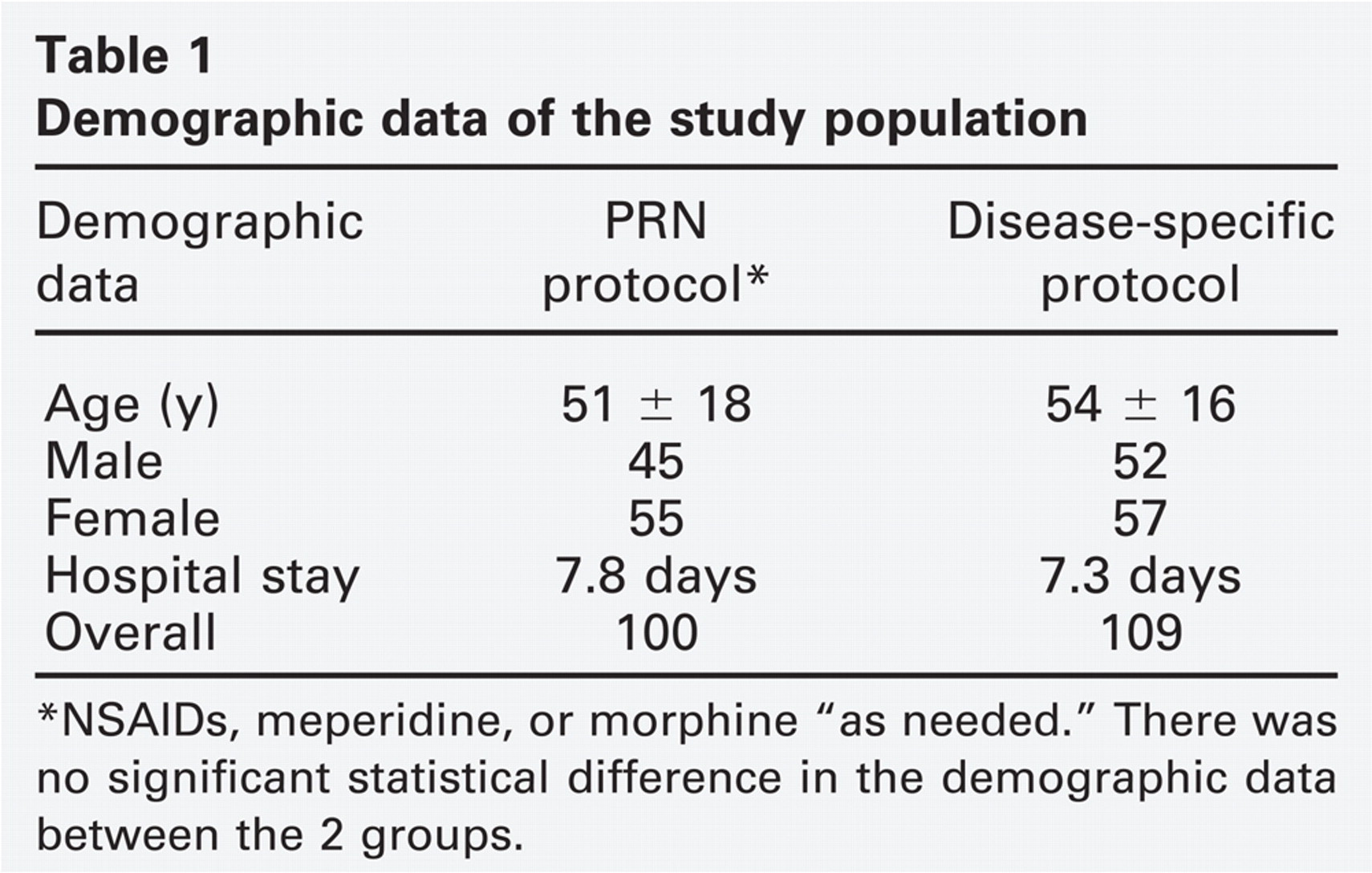
NSAIDs, meperidine, or morphine “as needed.” There was no significant statistical difference in the demographic data between the 2 groups.
PRN Pain-Control Regimen
We first evaluated the level of pain after surgery in patients who followed our PRN regimen (n = 100). Figure 1 shows the number of patients requiring drugs during the first 7 postoperative days. During day 1, 25% of the patients requested pain-control medication. There was a 50% decline during the following 2.8 days, and fewer than 7% required pain-control medication at 1 week after surgery. The most commonly prescribed drug was diclofenac.
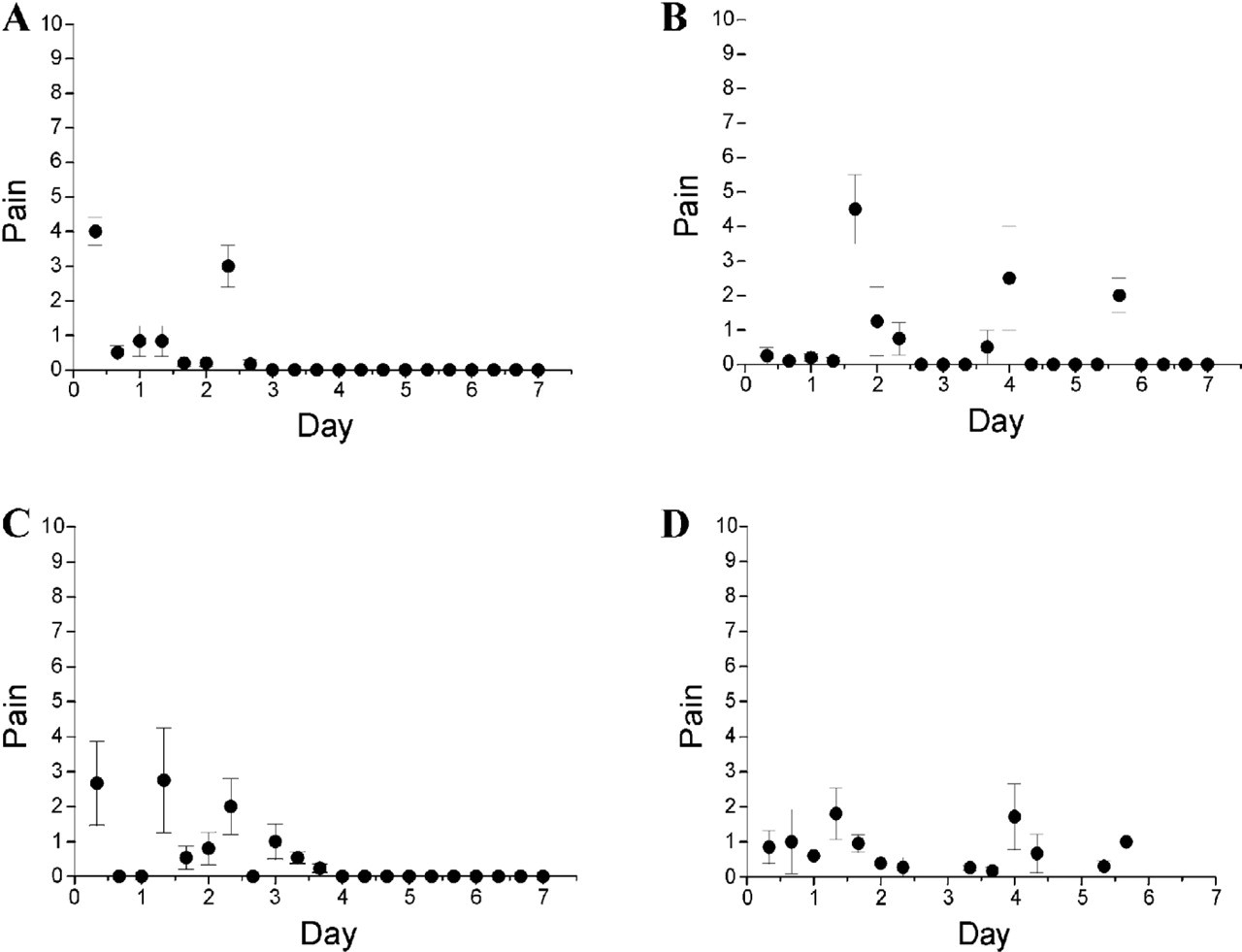
The PRN patients were categorized into 4 groups according to the extent and type of surgery: maxillofacial and mandibular, skull base, major neck, and minor neck. A statistical comparison was performed between groups and included the average of their levels of pain during the 7 days, time to reduction to one half the level of pain (t0.5), and the integral of the level of pain post surgery (AUC). Figure 2 shows the difference in the levels of pain during the first week after surgery. A significant degree of pain was recorded during the first 3 days for the patients undergoing maxillofacial and mandibular surgeries. The level of pain varied from 6 ± 1.5 immediately after surgery to 1 ± 0.6 seven days later (mean 2.63 ± 1.1, AUC 46). The level of pain declined by half (2.8 days) after surgery. A moderate degree of pain was recorded for the patients undergoing skull-base surgery; pain varied from 3.5 ± 2.5 immediately after surgery to 1.3 ± 0.6 one week later (mean 2.65 ± 1, AUC 53) and its decline was slow (t0.5 = 6 days). A mild degree of pain was recorded for the patients undergoing major neck surgeries (mean 1.5 ± 1, t0.5 2.8 days, AUC 28) and minor neck surgeries (mean 1.3 ± 1, t0.5 2.8 days, AUC 15). The 4 different groups of patients varied significantly in the level of postoperative pain that was reportedly experienced (P < 0.0001). There was a significant reduction in the level of pain 1 hour after drug application “as needed” (P < 0.001) after all operations (Fig 1, dashed line). Nevertheless, our data clearly showed that these patients reported the return of a substantial degree of pain as soon as the drug effect subsided several hours later.
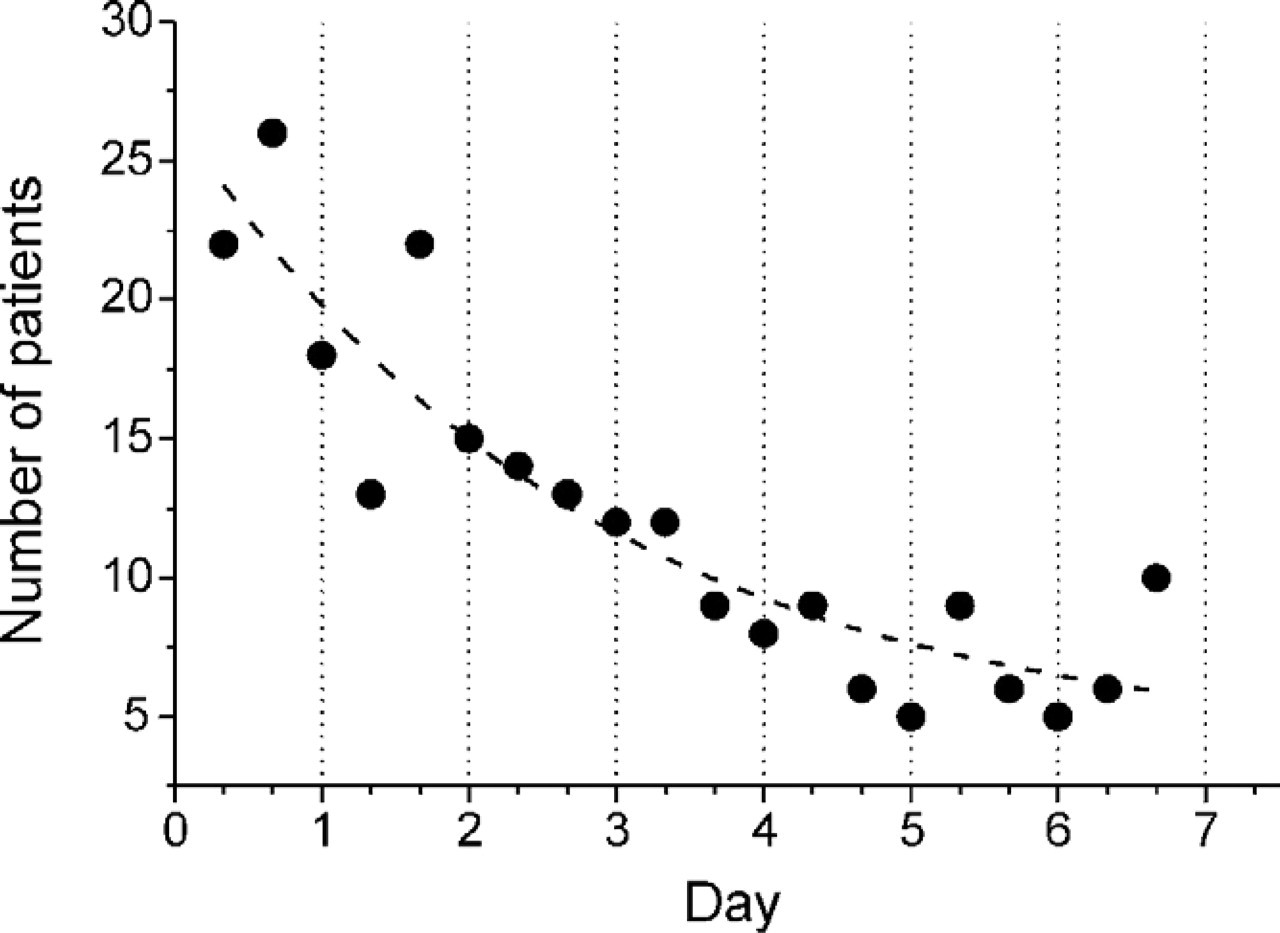
Number of patients requiring drugs during the first 7 postoperative days. All patients were treated using a PRN pain-control regimen.
Surgical procedures
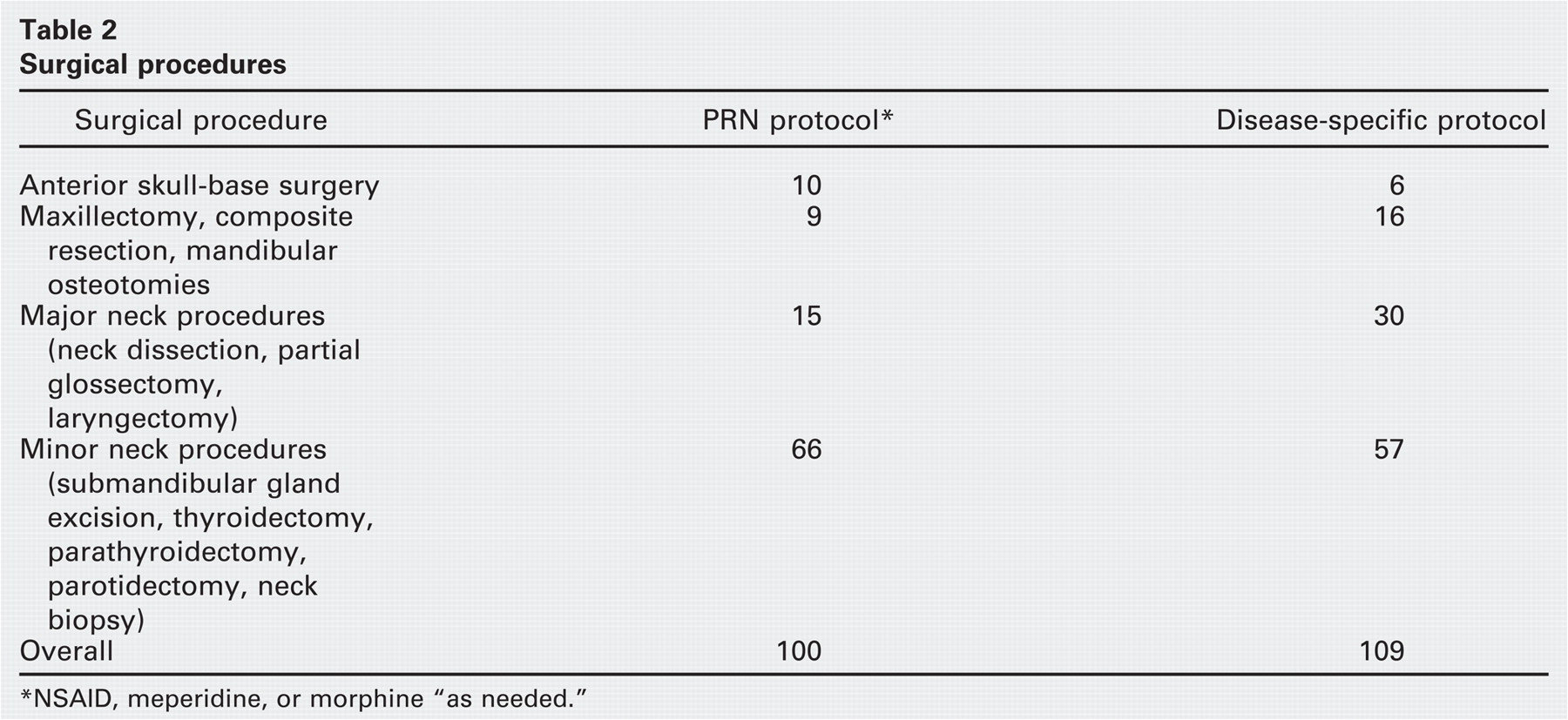
NSAID, meperidine, or morphine “as needed.”
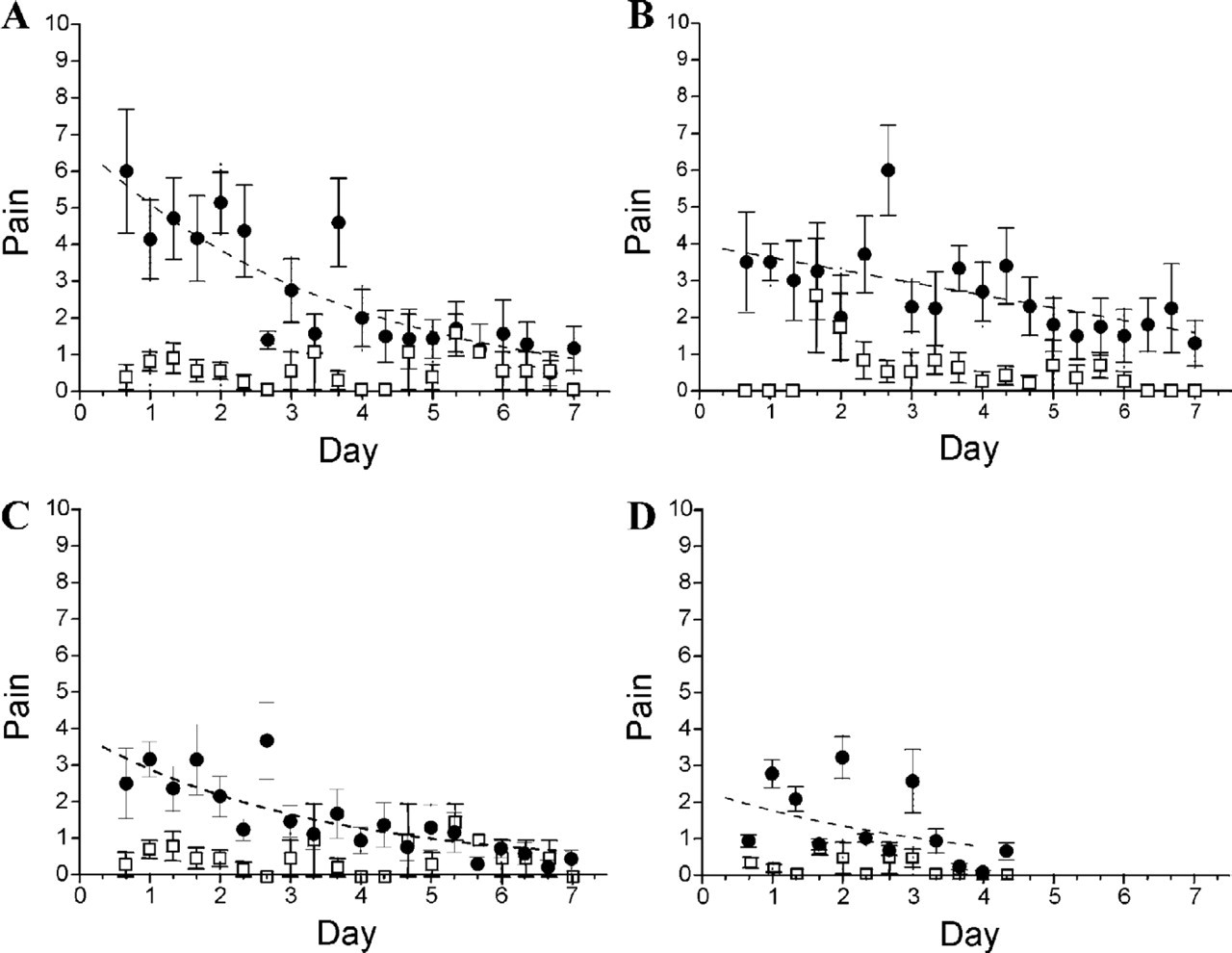
Differences in postoperative pain levels after 4 different head and neck procedures in patients treated using the PRN protocol (mean ± standard error). Black circles represent the average level of pain measured 3 times a day. Open boxes represent the level of pain measured 1 hour after application of the drug. (A) Maxillofacial and mandibular surgery, (B) skull-base surgery, (C) major neck surgery, and (D) minor neck surgery.
Specific Pain-Control Regimen
In the second part of our study, we tailored a specific pain-control protocol to each type of operation according to the level of pain that had been recorded in the first group. These patients were treated with analgesics given at predetermined hours. Relative to the first group, there was a significant reduction in the level of pain for patients undergoing maxillofacial, mandibular and skull-base surgeries (P < 0.001), a borderline significant reduction for patients undergoing major neck procedures (P = 0.08), and no significant reduction for patients who underwent minor neck operations (P = 0.3). Figure 3 depicts the level of pain during the postoperative period by using a scheduled pain-control medication, and Table 3 shows the mean level of pain reported for the 2 different regimens. There were no cases of severe complications (ie, renal or gastrointestinal bleeding or postsurgical bleeding) among our patients.
Discussion
Surgical procedures for the resection of neoplasms of the head and neck can be associated with a significant degree of pain. Various surgical techniques for the extirpation of head and neck tumors have been well described in the literature during the past 100 years, but the level of pain characteristically experienced by the patient after specific types of surgery has not been defined to date. In a multidepartmental survey of acute pain level measured 72 hours after surgery, the otolaryngologic- and maxillofacial-related pain was rated 6 and 7 of 11, coming after orthopedic, abdominal, gynecologic, urologic, and neurosurgical procedures and before plastic, ophthalmologic, vascular, and oral procedures. 3
The postoperative pain levels after 4 different head and neck procedures in patients treated using the procedure specific pain-control protocol (mean ± standard error). (A) Maxillofacial and mandibular surgery, (B) skull-base surgery, (C) major neck surgery, and (D) minor neck surgery.
The objective of the current study was to estimate the level of acute pain after head and neck tumor resection. In the first part of the study, we evaluated the PRN protocol routinely used in our department for treating acute postoperative pain. We then used these results to tailor a specific pain-control protocol specific to each procedure.
The mean level of pain reported for the 2 regimens during 1 week postsurgery
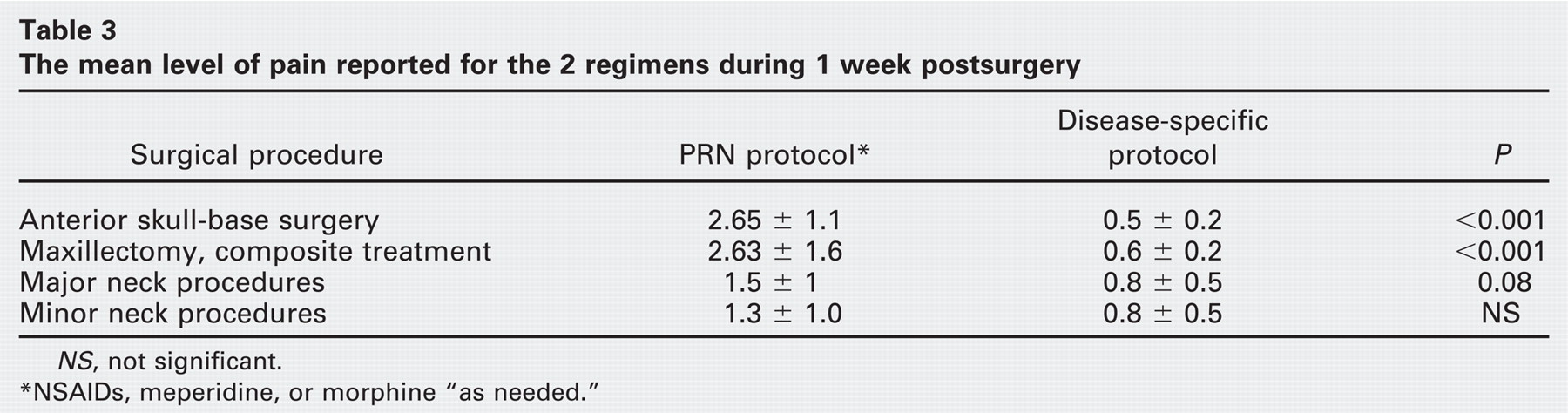
NS, not significant. *NSAIDs, meperidine, or morphine “as needed.”
The overall results of the study show that a PRN protocol is not adequate for management of pain after surgery. Although we did find a reduction in the level of pain following drug administration, the patients reported a significant degree of pain during the intervals between drug administration as well as throughout the postoperative period. This outcome was most significant after operations that involved craniofacial and mandibular osteotomies. These patients had moderate to severe levels of pain during the first 3 postsurgical days whereupon the level of pain decreased by half. Based on these findings, we suggest treating these patients with IV-PCA during days 1 to 3 and then with scheduled NSAIDs, regardless of whether the patient complains of pain. Our results clearly showed a sharp reduction in the level of pain during the postoperative period among the patients who were medicated according to this protocol. Patients scheduled for skull-base procedures also suffered a moderate degree of pain shortly after surgery; unlike patients undergoing maxillofacial osteotomies, however, these patients reported a slow reduction in the level of pain (t0.5 = 6 days). Patients undergoing skull-base procedures most frequently required continuous drainage of cerebrospinal fluid because of violation of the dura during surgery, and this mandates bed rest for 5 days until the drain is removed. 5 These patients complained mainly of musculoskeletal and back pain because of lying in a supine position for a prolonged period of time. We therefore prescribed NSAIDs for these patients whether or not it was requested by the patient.
Patients after intracranial and skull-base procedures are at risk for developing severe intracranial complications, such as meningitis, tension pneumocephalus, and hemorrhage. 6 Treatment of pain with a nonopiate analgesic allows close monitoring of the patient's neurologic and mental conditions. We therefore preferred to administer tramadol PRN as an adjuvant pain control because this drug does not cause much sedation.
NSAIDs have analgesic properties that are associated with opioid-sparing options and few side effects. Adequate postoperative analgesia may be provided by the routine administration of these drugs. 7 Furthermore, because these drugs do not induce respiratory depression or sedation, their administration may facilitate less intensive postoperative monitoring and allow close neurologic follow-up after intracranial procedures. In addition, NSAIDs do not require sophisticated delivery mechanisms. If administered at regular intervals, regardless of whether or not the patient requested pain relievers, NSAIDs can decrease patient dependence on opioids with satisfactory results.
Few articles have assessed the level of chronic pain in head and neck cancer patients,4,8-12 and none of them assessed the level of pain during the early postoperative period. In our current study, we also assessed the level of pain in 100 patients scheduled for oncological head and neck surgery 1 day before their operation. Nine of them reported that they were suffering from levels of pain varying from 1 to 7 on a scale of 0 to 10, with a duration varying from 1 to 24 hours per day and from 1 to 7 days per week. Five of these 9 patients had maxillofacial tumors and reported using NSAIDs or dipyrone for pain control. In agreement with our findings, Chaplin and Morton 4 have also reported that 8% of their 93 reported patients had suffered from severe pain before surgery (48% suffered some degree of pain). They noted that the highest level of pain was among patients suffering from tumors originating in the nasopharynx and that the level of pain decreased significantly 12 to 24 months after surgery.
Conclusions
We present the results of a prospective evaluation of acute pain in patients with head and neck tumors during the early postoperative period using 2 different regimens for pain control. The PRN protocol was found to be inadequate for the management of pain after major head and neck, craniofacial, and skull-base surgeries. Our results suggest that patients undergoing maxillofacial procedures should best be treated with IV-PCA during days 1 to 3, followed by the use of scheduled NSAIDs, and that patients undergoing major neck surgery should be treated with scheduled NSAIDs or tramadol for 5 to 7 days, whether or not they complain of pain.
We propose a standard protocol for the treatment of acute pain after head and neck surgeries. Further prospective, multicenter comparative studies are needed to delineate the most appropriate management of these patients and to determine the value of specific pain-control regimens in this setting.
Acknowledgment
The authors thank Esther Eshkol for editorial assistance and Shoshana Chazan, RN and Victoria Brik, RN, for their contribution.