
Abstract
Objective
To review our favorable experience with maxillofacial disassembly for exposure and resection of tumors of the skull base.
Patients and Methods
This is a retrospective review of 31 patients from 1997 to 2005 treated by maxillofacial disassembly and includes 22 patients with midface disassembly and 9 patients with mandible with or without midface disassembly.
Results
Follow-up ranges from 2 weeks to 7 years: 23 of 31 patients are alive and disease free; 3 patients are alive with disease; 3 patients have died of distant metastasis. There were 14 complications in 12 (38.7%) patients; 13 of 14 complications were minor. One major complication (cardiovascular accident) resulted in the single postoperative mortality in this series.
Conclusion
Our technique of maxillofacial disassembly allows for tailored exposure of all regions of the anterolateral skull base with acceptable perioperative morbidity in appropriately selected patients.
The quest for more anterior exposure of the PPF and PPS in anterolateral skull base surgery has yielded a host of transfacial approaches that involve osteotomies of the maxillofacial skeleton. Several authors 3 4 have described maxillotomy “swing” procedures via Weber-Fergusson facial incisions that split the upper lip and create a maxillary osteoplastic flap based either on the cheek skin or hinged inferiorly on the palate. Various authors have described transmandibular approaches to the PPS and ITF. Dingman and Conley 5 popularized the lower lip splitting incision for access to these areas via horizontal ramus mandibulotomy. Biller et al 6 modified the midline mandibulotomy mandible swing approach for wide transmandibular access to the anterolateral skull base with additional exposure of the nasopharynx through the palate. Attia et al 7 described an osteotomy of the parasymphyseal region paired with a horizontal osteotomy of the ramus of the mandible above the lingula to raise the hemimandible segment superiorly as an osteoplastic flap attached to cheek soft tissue for wide exposure of the anterolateral skull base. Hirano et al 8 described a complete sagittal face splitting incision that allows complete lateral hemifacial degloving along with median mandible swing osteotomy and gives wide exposure of the PPF and ITF.
The latest innovation in anterolateral skull base exposure involves complete removal of the bones of the facial skeleton to be set aside and reimplanted as free grafts during the reconstructive portion of the procedure. Nuss et al 9 and Janecka et al 10 described this concept of modular craniofacial disassembly for access to the skull base and coined the term “facial translocation” to describe the technique. Key features of the craniofacial disassembly technique include judicious use of coronal and facial incisions for exposure of the skeleton followed by osteotomies for exposure of the area of interest.
Maxillofacial disassembly is more a philosophy than a specific surgical procedure, and as such is tailored to lesions in a range of locations. In this article, we will review our favorable experience with aggressive disassembly of the maxillofacial skeleton, including orbit, maxilla, zygoma, and mandible, as free grafts unattached to overlying soft tissue for exposure of the skull base.
Methods
This is a retrospective review of charts over 8 years from 1997 to 2005 of patients with aggressive, malignant, and/or recurrent tumors invading the anterolateral skull base performed by the senior author (Y.D.), who specifically underwent surgical removal of their tumors via maxillofacial disassembly techniques (Figs 1-6). The study group includes 31 patients, 9 of whom underwent disassembly of their mandible. The average age is 52.6 years (range, 16 to 74 years). The tumors include squamous cell carcinoma (7), meningioma (6), esthesioneuroblastoma (3), sarcoma (2), schwannoma (2), adenoid cystic carcinoma (2), and giant cell tumor (2) among others. Seventeen (54.8%) had prior radiation therapy or chemoradiation therapy. Also, 16 (51.6%) patients had prior surgical procedures. We considered major procedure-related complications to be CSF leak, tension pneumocephalus, and meningitis.
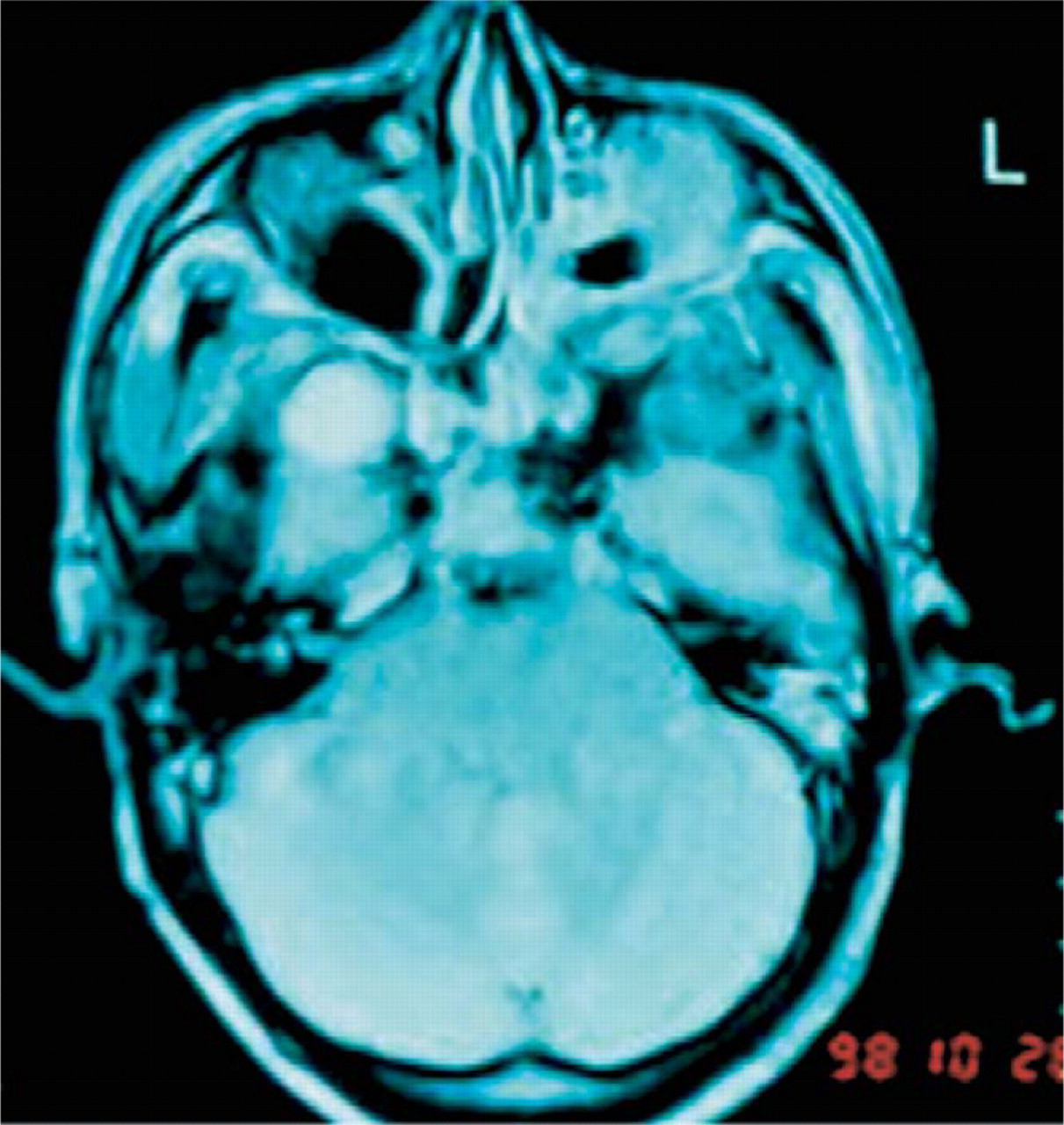
Axial MRI demonstrates right skull base osteosarcoma.

Exposure gained with disassembly of midface.
Results
Retrospective review of our study population shows that only 1 of 31 patients has been lost to follow-up. The follow-up of the remaining patients ranges from 2 weeks to 7 years; average follow-up is 3.8 years. Twenty-three (74.2%) of 31 patients are alive and disease-free; 3 (9.7%) of 31 patients are alive with residual or recurrent disease. Three (9.7%) of 31 patients have died of their disease, all from distant metastases. One patient died of unrelated causes, and 1 patient died of complications of surgery. Total survival rate for this study population is 83.9%, and disease-specific survival rate is 87.1%.
There were a total of 14 complications in 12 of 31 patients for a surgical complication rate of 38.7%. All complications were classified as minor, except 1 patient who had a postoperative stroke and died 2 weeks after her surgery. The 13 minor complications include 3 cases of nasal bone resorption, 2 cases of temporary palsy of the frontal nerve, 3 cases of wound dehiscence and/or exposed hardware, 1 case of minor wound infection, and 3 cases of eyelid complications (one each of ectropion, entropion, and upper eyelid ptosis). There were no major complications of CSF leak, tension pneumocephalus, or meningitis. There were no complications involving the replaced bone grafts, either bone necrosis or osteomyelitis. There were also no cases of trismus or malocclusion. No differences in complication rate as to dose or length of radiotherapy received were noted.
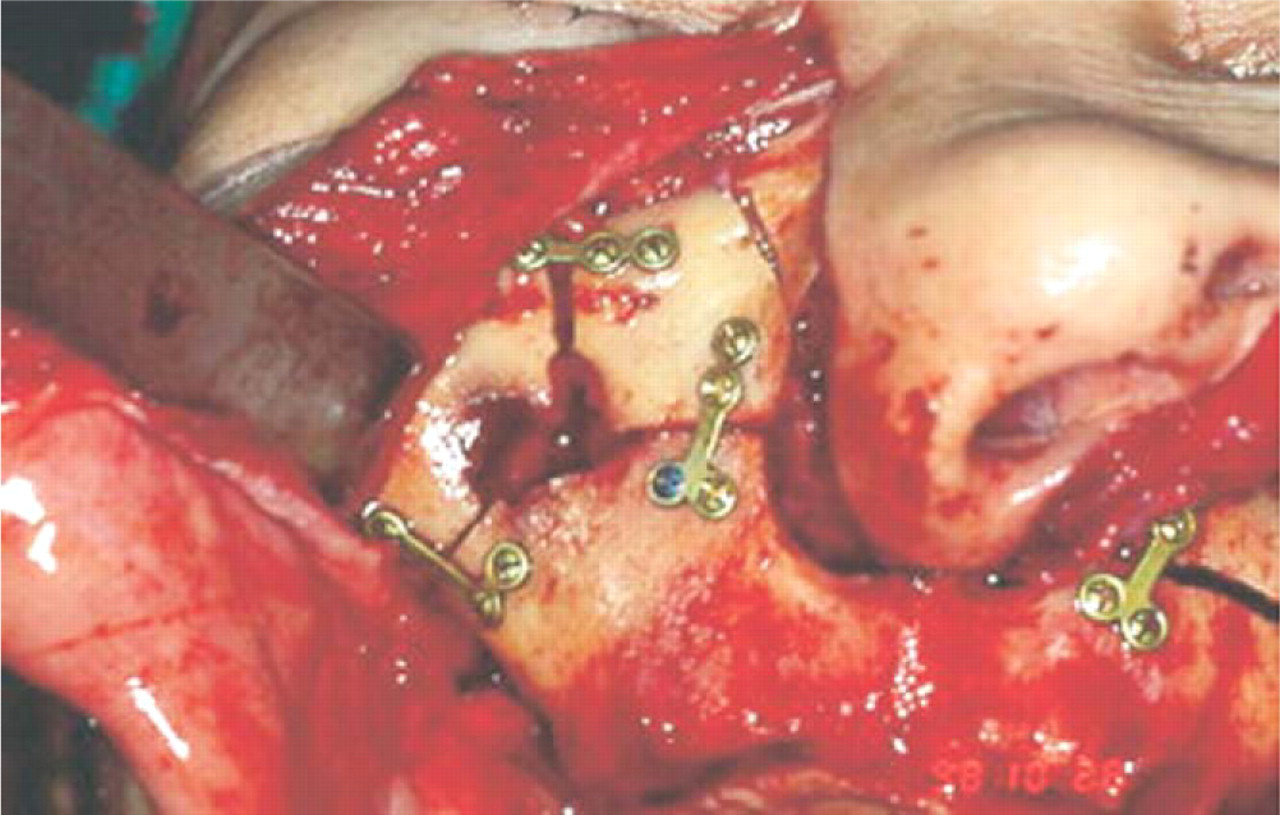
Disassembled segment is plated to LeFort 1 osteotomy.
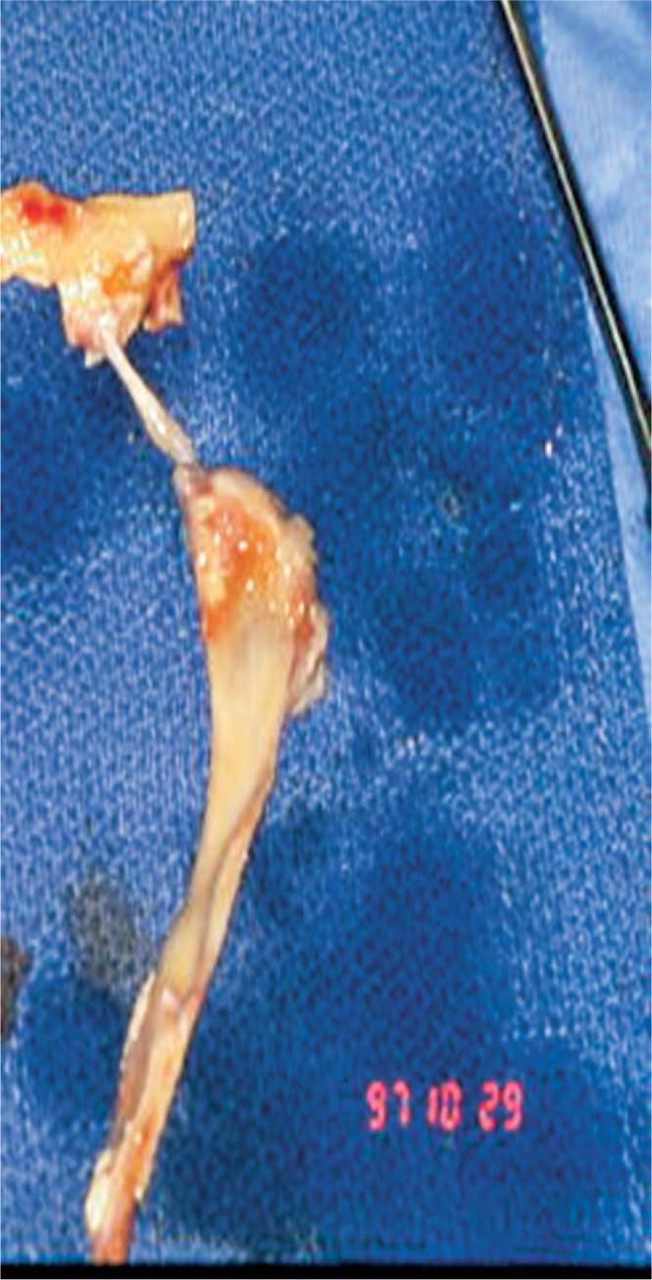
Osteotomized mandible.
Discussion
The maxillofacial disassembly technique allows for wide anterior and lateral exposure of the skull base with complete unobstructed view of the areas of interest without intervening facial bones pedicled on soft tissue flaps.
The concept of removing the bones of the midface and placing them back as free grafts has its roots in extensive experience in treating comminuted midfacial fractures. Janecka et al 10 popularized the concept of maxillofacial disassembly specifically for tumor access. Mann et al 11 described an approach to the nasopharynx, ITF, and PPF essentially through a large antral window that they used to resect recurrent JNA tumors in 5 patients and recurrent nasopharyngeal carcinoma in 1 patient, with replacement of the malar bone graft during reconstruction. Jackson et al 12 described the concept of directed osteotomies of the orbit, maxilla, and zygoma custom tailored to allow en bloc resection of “deeply situated tumors in difficult areas.” The Janecka et al series included over 250 cases of limited maxillofacial disassembly with only 6 infections of the bone grafts or surrounding soft tissues and 12 cases of formal facial translocation with no complications aside from the expected frontal branch facial nerve palsy from his exposure technique. A recent study from China by Hao et al 13 reviewed their 6-year experience using the formal facial translocation procedure to remove benign and malignant tumors from the nasopharynx, paranasal sinuses, and/or ITF in 75 patients. Unlike the Janecka et al series, these authors reported a 31% perioperative morbidity rate, including 16% incidence of necrosis of the bone graft.

Bone segments removed and facial nerve retracted allows direct access to the parapharyngeal space.

Postoperative panorex.
Demographic data
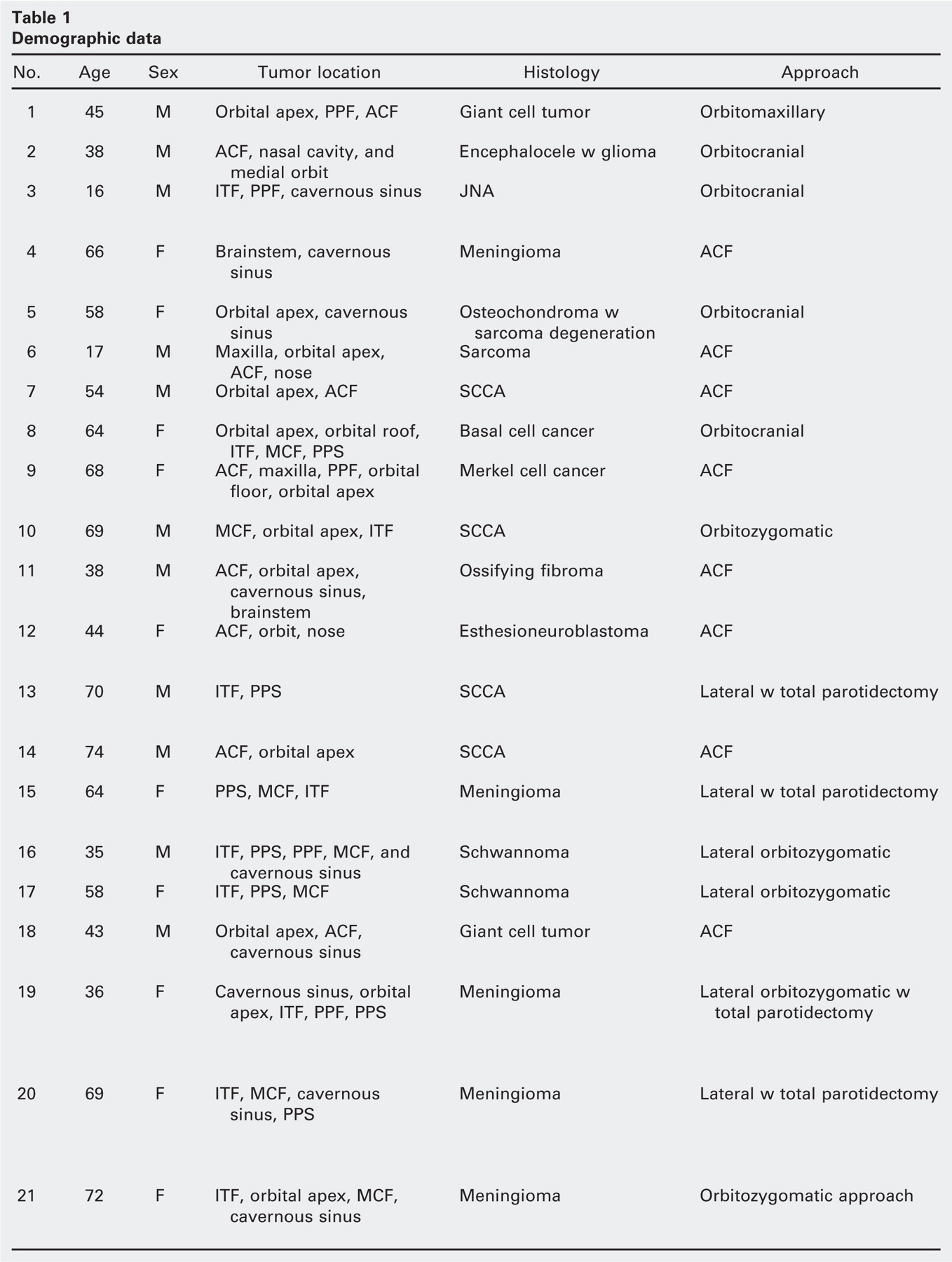
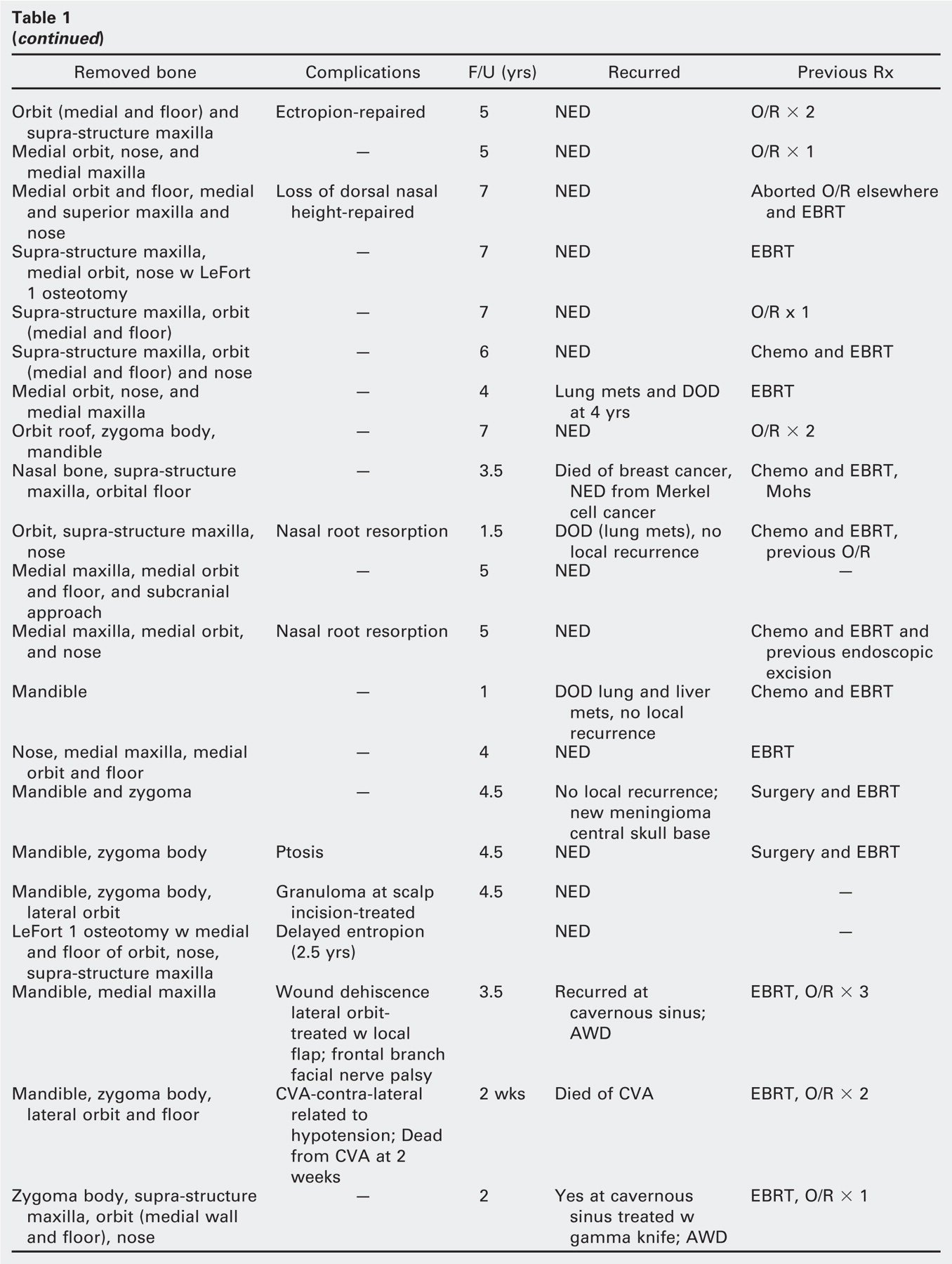
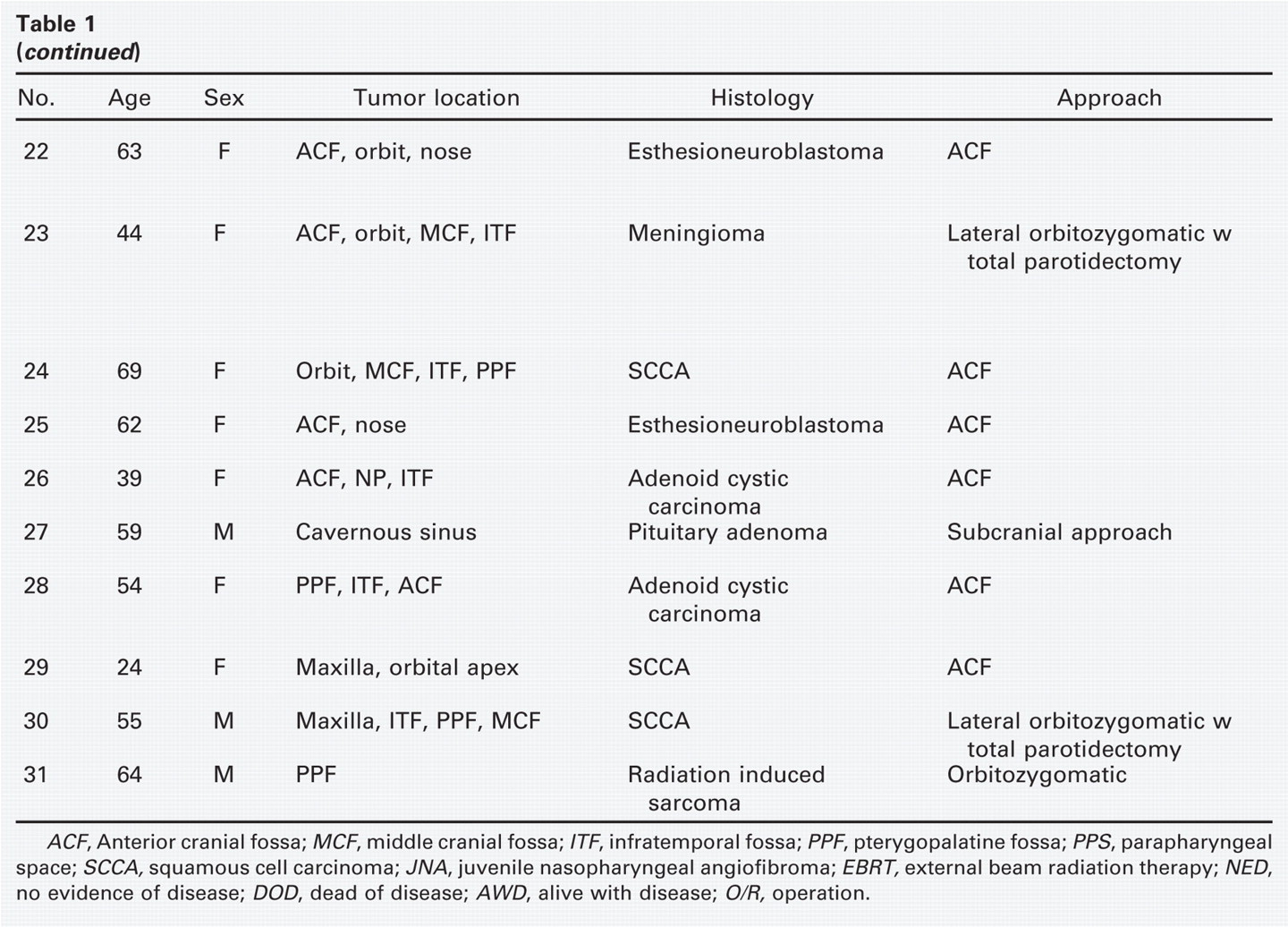
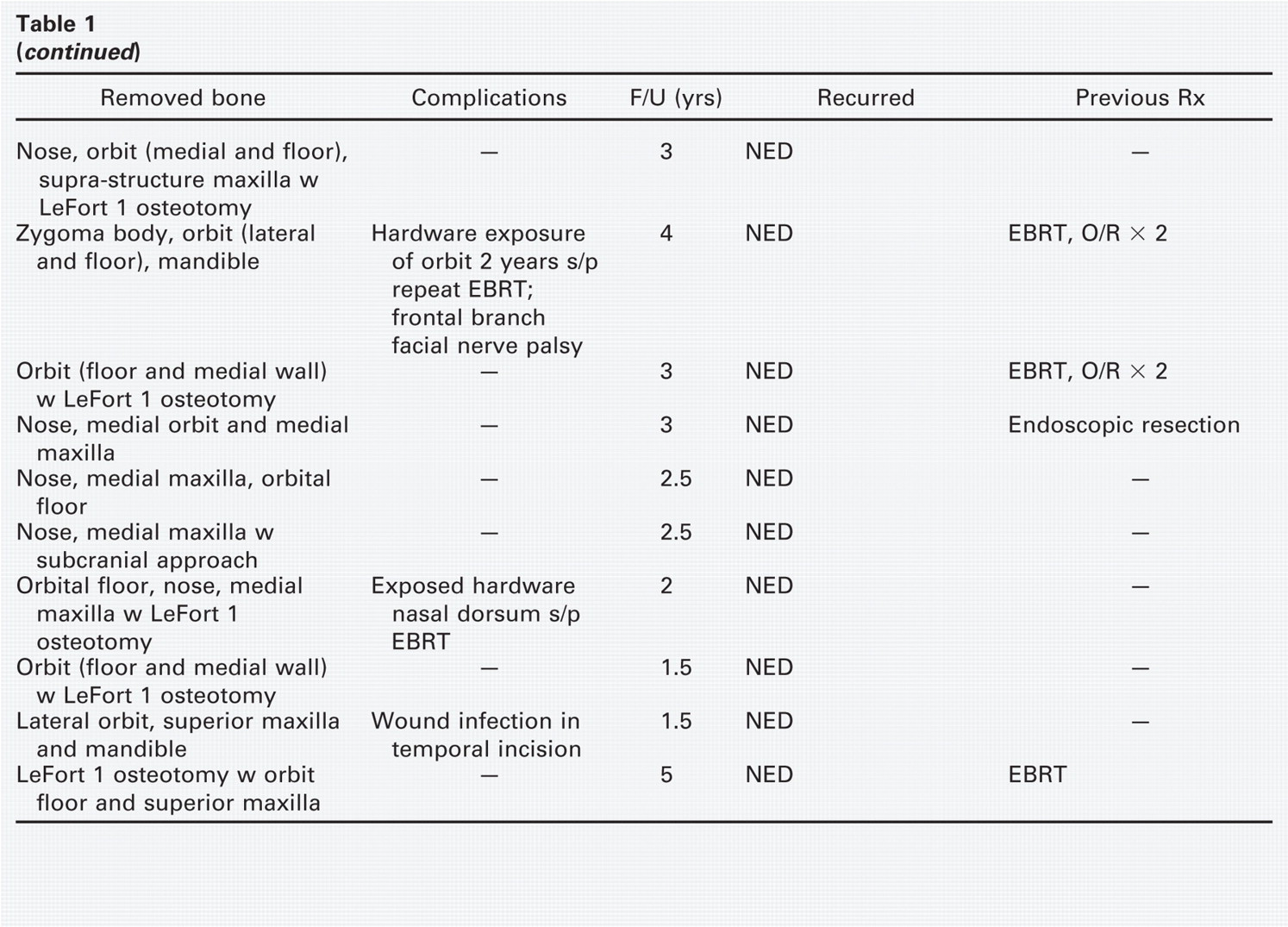
ACF, Anterior cranial fossa; MCF, middle cranial fossa; ITF, infratemporal fossa; PPF, pterygopalatine fossa; PPS, parapharyngeal space; SCCA, squamous cell carcinoma; JNA, juvenile nasopharyngeal angiofibroma; EBRT, external beam radiation therapy; NED, no evidence of disease; DOD, dead of disease; AWD, alive with disease; O/R, operation.
Our technique of maxillofacial disassembly offers several advantages. We have not found a need for a lateral facial incision that transects the frontal nerve. In fact, we have found the Weber-Fergusson extension below the eyelid unnecessary. This prevents prolonged lower lid edema. We preserve the integrity of the infraorbital and inferior alveolar nerves with all our osteotomies. We also try to minimize the use of facial incisions altogether, using the midfacial degloving approach whenever possible. A recent series of facial translocation technique by Suarez et al 14 reviewed 39 cases, including 19 cases approached through midfacial degloving without facial incisions. They concluded that adequate anterior and lateral exposure and room for the osteotomies is possible without facial incisions through midfacial degloving in selected cases. Their series also had a 38% perioperative complication rate, including 13% incidence of osteomyelitis of the bone graft.
We add temporary removal of the posterior half of ascending ramus of mandible to the maxillofacial disassembly technique in selected cases of tumor in the PPS and/or inferior ITF, recognizing that the mandible is a major obstacle to lateral exposure. 15 Many different techniques of mandible osteotomy have been described to expose the PPS, but the ideal osteotomy preserves the path of the inferior alveolar nerve. Donovan et al 16 described their transmandibular-zygomatic approach that includes pedicled reflection of the zygomatic arch, vertical ramus osteotomy with inferior displacement of the condyle and posterior ramus attached to the lateral pterygoid muscle at the condylar neck, resection of the coronoid process of mandible, and resection of the TMJ disk with subsequent reconstruction of the TMJ using a free galeal graft.
Guinto et al 15 modified the same technique to reach large tumors of the ITF and PPS in 10 patients. In 7 patients, they performed a similar vertical ramus osteotomy but rotated the posterior ramus and condyle segment upward and laterally hinged on the TMJ.
Jian et al 17 published their series from China describing their approach to the PPF in 9 patients using osteotomies of the midface and mandible. The surgeons made orbitozygo-matic and oblique mandible osteotomies at the mandibular angle and removed the malar complex and mandible segments after disarticulating the condyle from the TMJ to expose the PPF. During reconstruction, all disassembled bone grafts including mandible were placed back and secured with titanium miniplates without postoperative maxillomandibular fixation. Follow-up for this series ranged from 3 months to over 9 years. All patients in this series had transection of the frontal branch of the facial nerve, infraorbital nerve, and inferior alveolar nerve during the procedure. The authors had no complications that involved the replaced bone grafts. They also reported no cases of trismus or malocclusion. To our knowledge, this is the largest published series to date of mandible disassembly for exposure with subsequent fixation as a free graft. Our own series matches this study in terms of number (9 cases) of patients who underwent mandible disassembly and also reports no cases of complications that involve the replaced mandible bone graft or postoperative mastication or occlusion. By preadapting the miniplates to the bone grafts prior to making the osteotomies, we have also not found the need for either intraoperative or postoperative maxillomandibular fixation. Our technique, however, spares all cranial nerves during exposure and osteotomies. Particularly, the vertical ramus osteotomy spares the inferior alveolar nerve.
Our series of patients surgically treated with maxillofacial disassembly technique for tumors that involved the anterolateral skull base shows a favorable clinical outcome with an acceptable postoperative complication rate (38.7%) that is comparable with the complication rates reported in the series by both Hao et al 13 and Suarez et al. 14 Most of our complications are minor, aside from 1 case of mortality from postoperative stroke that was not specifically due to the exposure but rather early postoperative hypotension. We did note several cases of nasal bone resorption that required a secondary calvarial bone graft to the nasal dorsum. We report no instances of bone graft failure, osteomyelitis, or nonunion in contrast to the 16% and 13% bone graft complication rates reported by Hao et al and Suarez et al.
Hao 18 published another study where he compared his postoperative results for 42 patients undergoing facial trans-location with detachment and replacement of the maxillofacial bone grafts to 14 patients where the bone segments were left attached to the soft tissues of the cheek. He concluded that postoperative radiation therapy significantly increased the incidence of free bone graft necrosis compared with the pedicled bone flap group. He also found a much higher incidence of bone necrosis in the free bone graft group (11 of 42 patients, 26.2%) than the attached bone flap group (1 of 14 patients, 7.1%), but this didn't reach statistical significance.
Another study by Pogrel et al 19 compared the success rate of reconstructing segmental mandibular defects in 39 patients primarily with fibula or iliac crest flaps to 29 patients reconstructed secondarily with iliac crest or rib nonvascularized bone grafts. 19 All bone graft fixation to the mandible was done with titanium plates. They found an overall 95% success rate with vascularized flap compared with 76% success rate with bone graft. They also showed a direct correlation between the length of free bone graft and the risk of failure and concluded that bone grafts for mandibular reconstruction should be limited to defects less than 9 cm. Furthermore, 2 of 3 patients reconstructed with bone graft with preoperative radiation therapy failed compared to only 1 of 16 patients with preoperative radiation therapy who failed vascularized flap reconstruction.
Both studies by Hao and Pogrel et al suggest that bony reconstruction of the maxillofacial skeleton and/or mandible in patients who undergo radiation therapy is best accomplished with vascularized or pedicled bone flaps compared with free bone grafts to prevent bone segment necrosis. All of the patients in our series who undergo maxillofacial disassembly have aggressive and/or recurrent tumors or cancers that justify this radical approach for exposure. Many (54.8%) of these patients have had prior radiation therapy, yet our follow-up of up to 7 years has no cases of bone graft necrosis or nonunion. We believe we minimize the risk of complications to the disassembled bone grafts by carefully handling and preserving the grafts in saline-soaked moist gauze, using sound principles of rigid stabilization and internal fixation with plates during reconstruction, and covering or wrapping the bone grafts with vascularized flaps like pericranium, temporalis, or temporoparietal fascia. Hao 18 recognized in his series of facial translocation that he was able to minimize bone graft necrosis by using rigid 3-point fixation to facilitate bony union and resuspending the soft tissues to the maxillofacial bone grafts. Suarez et al 14 noted in their series that most of the surgical complications happened in patients undergoing standard facial translocation with extensive facial incisions. The patients undergoing midfacial degloving technique did not have perioperative complications in this study. We also minimize the risk of mandible bone graft necrosis or nonunion in our patients who undergo the vertical ramus disassembly by using a purely extraoral lateral retromandibular approach to avoid contamination from the mouth and by removing a posterior ramus and condyle bone graft smaller than 9 cm in size as recommended by the Pogrel et al study.
The patients reviewed in this study are a subset of many patients at our institution treated surgically by a wide variety of techniques for tumors that invade the skull base. Our technique of maxillofacial disassembly provides a direct approach to all regions of the anterolateral skull base with 270 degree exposure of all areas of interest without any intervening pedicled tissue to obstruct the field of view. No other technique provides this degree of exposure. We feel that the disassembly technique does carry significant potential risk of morbidity and, therefore, should be applied judiciously for selected recurrent and/or aggressive neoplasms of the anterolateral skull base.
The vertical ramus osteotomy bone graft in particular is our own unique contribution to traditional maxillofacial disassembly and allows excellent lateral exposure of the lower ITF and PPS. 20 Our case example for mandibular disassembly has been reported previously as a pathology article. 20 Traditional approaches to the PPS, such as transparotid, transcervical, or midline mandibulotomy, are sufficient to resect the vast majority of tumors in this area. We think that the vertical ramus osteotomy and disassembly is unnecessary and inappropriate for lesions confined to the PPS in light of its morbidity and potential complications to the replaced bone graft. We advocate this technique only for large tumors that invade multiple regions of the anterolateral skull base, including the inferior ITF and PPS, or to allow access for a low infratemporal fossa craniotomy through the glenoid fossa.
Conclusions
Our experience with aggressive maxillofacial disassembly of the midface and mandible demonstrates that this is a very useful approach for wide unobstructed exposure of the regions of the anterolateral skull base, including the infratemporal fossa, pterygopalatine fossa, and parapharyngeal space, for the resection of large aggressive and/or recurrent tumors. Our surgical technique and modifications of traditional facial translocation allow for preservation of the facial nerve and infraorbital nerve, minimize the use of visible facial incisions for anterior exposure, and improve inferior exposure of the skull base through temporary removal of the condyle and posterior ramus. We believe that this is a very useful technique to add to the armamentarium of the skull base surgeon. Table 1.