
Abstract
Background
The pharyngeal constriction ratio is a ratio of pharyngeal area measured in lateral fluoroscopic view at the point of maximum pharyngeal constriction during the swallow to the pharyngeal area measured with the bolus held in the oral cavity. We hypothesize that the PCR may represent a surrogate measure of pharyngeal strength.
Objective
To investigate the relationship between the PCR and aspiration.
Study Design and Setting
Data from a computerized clinical database of individuals undergoing a videofluoroscopic swallow evaluation at a tertiary academic swallowing center was acquired.
Results
Two hundred sixty videofluoroscopic studies were abstracted. The mean PCR was 0.32 (± 0.02) for individuals who aspirated and 0.20 (± 0.02) for individuals who did not (P < 0.001). In a multiple logistic regression analysis, the PCR was significantly associated with the prevalence of aspiration (P < 0.01). Individuals with a PCR greater than 0.25 were 3 times more likely to aspirate (95% CI = 1.7, 5.1).
Conclusions
The pharyngeal constriction ratio is associated with the presence of aspiration on fluoroscopy. Before the PCR can be used as a surrogate measure of pharyngeal constriction, correlation with pharyngeal manometry will be necessary.
Significance
The pharyngeal constriction ratio is associated with the presence of aspiration on fluoroscopy.
Pharyngeal strength can be assessed endoscopically with the pharyngeal squeeze maneuver or with pharyngeal manometry. It can also be evaluated on videofluoroscopy during passage of a bolus. We have developed a fluoroscopic measure of pharyngeal constriction referred to as the pharyngeal constriction ratio (PCR). 5 6 The PCR is defined as the ratio of pharyngeal area measured (in lateral view) at the point of maximum pharyngeal constriction during the swallow to the pharyngeal area measured with the bolus held in the oral cavity (pharynx at rest). An elevated PCR suggests decreased pharyngeal constriction and may predict the likelihood of aspiration. The purpose of this investigation was to evaluate the association between an elevated PCR and the prevalence of aspiration on videofluoroscopic swallow evaluations.
Pharyngeal area was measured in the lateral view during the “hold” position; that is, with the bolus held in the oral cavity prior to the swallow. The outline of the pharyngeal area was defined posteriorly by the posterior pharyngeal wall from the midportion of the tubercle of the atlas down to the level corresponding to the height of the top of the arytenoid cartilage. The inferior outline was carried forward from this point over the arytenoid cartilage and anteriorly to outline the epiglottis, the vallecula, and the tongue base to the point at which the soft palate came into contact with the nasal spine. The superior border was a straight line between the posterior nasal spine and the midpoint of the tubercle. The area of the space was then automatically calculated (in cm 2 ) and referred to as PAhold.
Methodology
The records of individuals undergoing a videofluoroscopic swallow evaluation were acquired from a clinical database at the Center for Voice and Swallowing at the University of California, Davis. The PCR and information regarding patient diagnosis, demographics, and the presence of aspiration were abstracted. All radiographic studies were conducted at the Voice and Swallowing Center in accordance with the routine radiographic protocols approved by the institution. Permission to conduct this study was obtained from the Institutional Review Board (IRB) at UC Davis. All studies were performed on a properly collimated Phillips fluoroscopic unit that provides a 63-kV, 1.2-mA type output for the full field-of-view mode (9-in input phosphor diameter). Fluoroscopy studies were recorded on a high-quality videocassette VHS recorder/player. The videotaped images were later captured with a digitizing board from Data Translation, Inc. (Marlboro, MA) and a Macintosh computer (PPC 8100). The software program used for analysis of fluoroscopic images is called IMAGE (developed by Wayne Rasband et al at the NIH). Area measurements were made after calibration of the digitized image to the size of the 1.7-cm-diameter wire loop taped to the chin of the study subject.
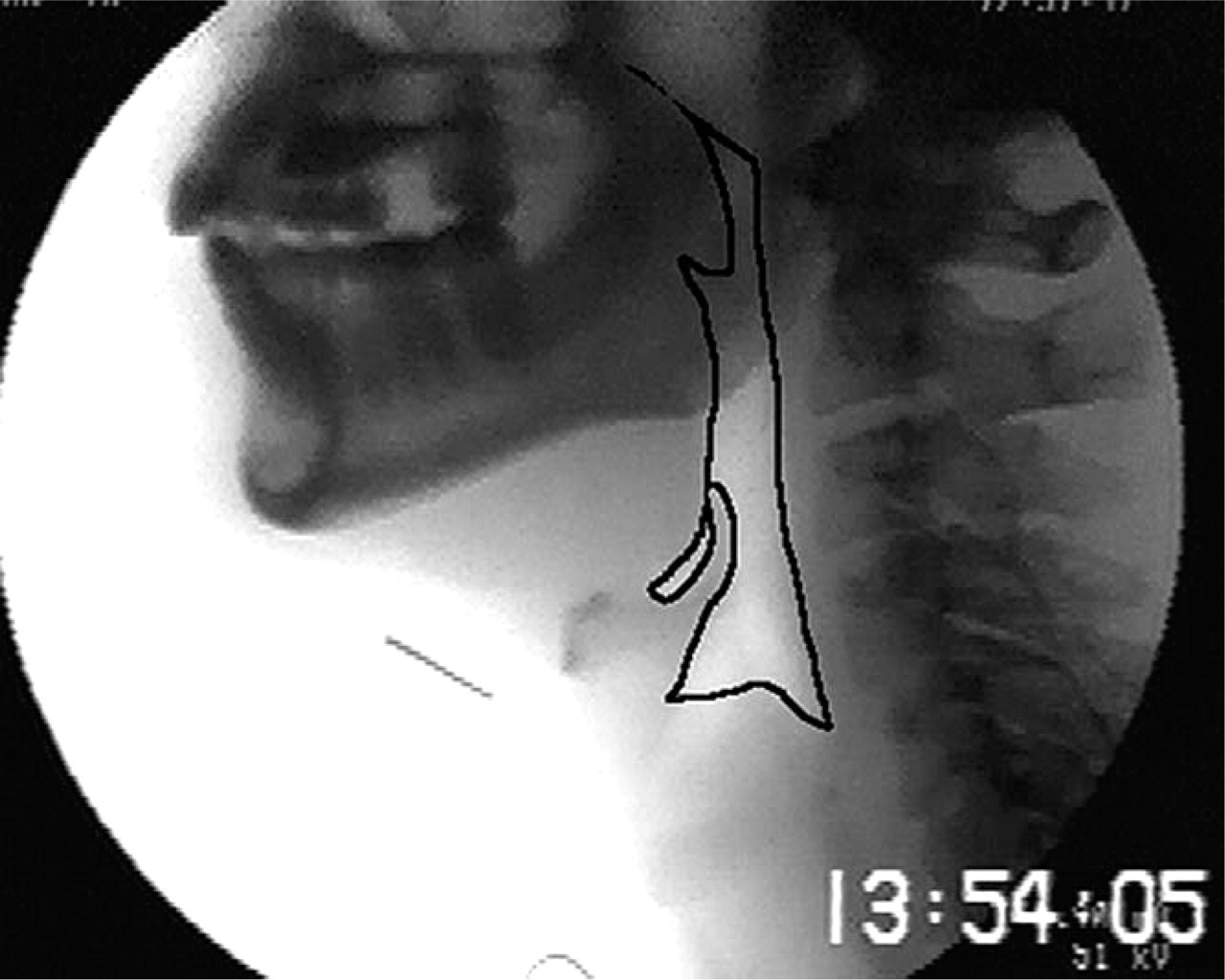
All measures were obtained from lateral views for the largest bolus swallowed during the study. A detailed technical description of these measures and their acquisition has been previously described and is briefly summarized here. 5 Pharyngeal area was measured in the lateral view during the “hold” position; that is, with the bolus held in the oral cavity prior to the swallow. The outline of the pharyngeal area was defined posteriorly by the posterior pharyngeal wall from the midportion of the tubercle of the atlas down to the level corresponding to the height of the top of the arytenoid cartilages. The inferior outline was carried forward from this point over the arytenoids and anteriorly to outline the epiglottis, vallecula, and tongue base to the point at which the soft palate came into contact with the nasal spine. The superior border was a straight line between the posterior nasal spine and the midpoint of the tubercle. The area of the space was then automatically calculated (in cm 2 ) and referred to as PAhold (Fig 1). Pharyngeal area was again measured at the point of maximum pharyngeal constriction during the swallow; this measure is referred to as PAmax (Fig 2). The ratio of PAmax/PAhold was defined as the pharyngeal constriction ratio (PCR). An elevated PCR suggests diminished pharyngeal constriction.

Pharyngeal area was again measured at the point of maximum pharyngeal constriction during the swallow; this measure is referred to as PAmax.
Results
Two hundred sixty videofluoroscopic studies were abstracted. The mean age of the cohort was 65 (± 20) years. Fifty-five percent were male. The most common diagnoses were head and neck cancer (40%) and stroke (30%). Other diagnoses included gunshot wounds to the neck, dysphagia of unclear etiology, globus sensation, vocal cord paralysis, skull base tumors, cerebral palsy, developmental delay, and neuromuscular weakness. The mean PCR was 0.32 (± 0.02) for individuals who aspirated and 0.20 (± 0.02) for individuals who did not (P < 0.001). After adjusting for age, gender, and diagnosis, the multiple logistic regression analysis revealed that the PCR was significantly associated with the presence of aspiration (P < 0.01). Individuals with a PCR greater than 0.25 were 3 times more likely to aspirate (95% CI = 1.7, 5.1).
Discussion
Pharyngeal strength can be assessed in various ways, including the pharyngeal squeeze on fiberoptic endoscopic evaluation of swallowing (FEES) and pharyngeal peak pressures on manometry and during a fluoroscopic evaluation of swallow. Weak pharyngeal strength assessed by the pharyngeal squeeze maneuver has been associated with an increased prevalence of aspiration. Perlman et al 1 demonstrated that the risk of aspiration of pureed food in patients with dysphagia is related to both sensory deficits and pharyngeal muscular tone evaluated on flexible endoscopy. They concluded that the aspiration of pureed food might depend more on muscle tone (pharyngeal constriction) than sensation. A comparable study by the same authors using thin liquids showed similar findings. 2 It seems that while both pharyngeal sensation and muscle tone play important roles in directing the bolus into the esophagus, disturbances in the latter are more likely to lead to aspiration.
The present findings support those of previous investigators and suggest that decreased pharyngeal constriction contributes to an increased prevalence of aspiration. 1 2 It is important to note, however, that the PCR is only a 2-dimensional assessment and does not measure pharyngeal volume. Neither does it consider separately the contributions of tongue base, hyoid, pharynx, or other structures to pharyngeal constriction. The act of swallowing is a dynamic process dependent on oral preparation, lingual propulsion, laryngohyoid elevation, epiglottic eversion, and pharyngo-esophageal segment opening. We chose to omit these additional measurements from the analysis of our investigation and focus solely on the PCR as a predictor of aspiration. Our investigation supports the work of previous researchers and suggests that pharyngeal strength has an essential role in airway protection during deglutition.
Takehara et al have recently attempted to use helical computerized tomography to obtain transverse plane information of the pharyngoesophageal segment and demonstrated good association between videofluoroscopy and CT. 7 However, at most institutions, the use of helical CT in the evaluation of the hypopharyngeal dimension is unlikely to be widely embraced currently due to cost and logistical constraints. Pharyngeal manometry provides a more reasonable method to measure pharyngeal strength, but this technology is not as readily available as is fluoroscopy.
The primary role of pharyngeal constriction in swallowing is pharyngeal clearing and bolus propulsion. We feel that the PCR provides a useful surrogate measure of pharyngeal constriction. Current efforts are underway in our institution to correlate fluoroscopic determinations of the PCR to manometric measurements of pharyngeal peak pressures during the swallow. Preliminary results (not shown) from our institution suggest that the PCR is inversely proportional to pharyngeal pressure detected on manometry (ie, an elevated PCR indicates diminished pharyngeal pressure). This is further evidence of the use of the PCR as a surrogate measure of pharyngeal strength and constriction.
Conclusion
The pharyngeal constriction ratio is associated with the presence of aspiration on fluoroscopy. Before we can definitively state that the PCR is an accurate surrogate measure of pharyngeal constriction, correlation with pharyngeal manometry will be necessary.