
Abstract
© 2007 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
The recurrence rate of oral cancer is relatively high when compared with that of other cancers.4 Locoregional tumor failure reported in several large-scale studies varied from 19 percent to 34 percent of oral cancer patients.5–7 It is well known that oral cancer patients with neck recurrences have a poor prognosis.6,8 Schwartz et al's study on the salvage treatment for recurrent oral cavity cancer showed that the recurrence interval was a reasonable predictor of survival.9 However, this is debatable because recurrence within 6 months might represent a residual tumor. Another study using meta-analysis studying salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract revealed that recurrence interval was not related to survival.10 Nevertheless, they included a variety of cancers rather than oral cavity cancer patients. Therefore, this study aimed to analyze the survival rate after local recurrence of oral cavity squamous cell carcinoma patients in a medical center in central Taiwan and to investigate whether the recurrence interval influences survival status.
Materials and Methods
This is a hospital-based study and has been approved by the Institutional Review Board of Taichung Veterans General Hospital (TCVGH). All patients who were admitted under the diagnosis of oral squamous cell carcinoma in TCVGH from March 1995 to November 2003 were included and the observation endpoint was set at 31 November 2005. The definition of oral cavity cancer in this study included cancer of the lip, mouth floor, tongue, gingiva, buccal mucosa, palate, and retromolar trigone. This study retrospectively reviewed the chart records of over 1600 patients. Those who had no pathological report, had been treated at other institutes, did not complete therapeutic protocol in our hospital, or had inadequate chart records were excluded. After these exclusions, there were 1282 cases that fulfilled the requirements and were included for further analysis.
The variables included: age of recurrence, gender, initial tumor stage, initial treatment modalities, tumor location, recurrent tumor stage, type of salvage treatment, histological features, recurrence interval, and survival duration after local recurrence. Local recurrence was characterized by reappearance of tumor near the primary site without cervical lymphadenopathy at least 6 months after completion of treatment with the same histological type and lacking distal metastasis. On the other hand, residual tumor after a full course of therapy was not considered as local recurrence. Recurrence interval was defined as the duration from the end of initial treatment to the day of local recurrence confirmed by pathological examination. Survival duration after recurrence was defined as the interval from treatment of local recurrence to the day of death or follow-up endpoint. Surgical resection was the first choice for management of local recurrence in our institute. Radiation or chemotherapy was reserved for those who were not suitable or reluctant to receive surgery or as an adjuvant therapy after surgical salvage. All cases were restaged according to the guideline of the American Joint Committee on Cancer.11
Statistical Analysis
This study used descriptive statistics for general data presentation. Comparisons of nominal or ordinal variables between survival and nonsurvival groups were analyzed by the χ2 test, whereas continuous variables were analyzed with Student's t test. Survival analysis was investigated by the Kaplan-Meier method. The differences between subgroups were examined by the log-rank test. Furthermore, relevant factors influencing the survival period were examined by the Cox proportional hazard model. All statistical analyses were performed by the SPSS software system for Windows (version 10.1; SPSS, Chicago, IL). Statistical significance was considered as P < 0.05.
Results
A total of 1687 patients were admitted to our hospital diagnosed with oral cavity squamous cell carcinoma from March 1995 to November 2003. Thirty-five patients (2.07%) had no pathological report at all. In addition, 105 cases (6.22%) did not complete the therapeutic protocols while 72 cases (4.27%) had incomplete chart records and 193 cases (11.44%) were referred from other hospitals due to recurrent disease. Adequate data were obtained from chart records of 1282 patients. Recurrence was identified in 648 cases (50.5%). Local recurrence happened in 401 cases (31.3%) whereas 247 cases (19.3%) had regional or locoregional recurrence. Among those with confirmed local recurrence, the average age of recurrence was 53.0 years (± 11.1 years). Males accounted for 95.8 percent (n = 384) of recurrent patients. The recurrence interval ranged from 6 to 62 months with an average of 20.5 months (± 16.1 months). Two hundred and seventy-four patients (68.3%) developed local recurrence within two years. The average follow-up period was 40.7 months (± 28.6 months) and there were only 29 cases (7.2%) of loss of follow-up before observation endpoint.
All patients had surgical excision as their initial treatment. Two hundred and twenty-four patients (55.9%) had no further adjuvant therapy, whereas 177 cases (44.1%) received postoperative radiotherapy with/without chemotherapy. After local recurrence, the majority of patients (n = 277, 69.1%) received salvage surgery only. Other therapeutic modalities included: salvage surgery plus radiation with/ without chemotherapy in 49 patients (12.2%), concomitant chemo-radiotherapy in 56 patients (14%), and supportive care only in 19 patients (4.7%). For ease of analysis, the various treatment arms were divided into two subgroups: salvage with surgical treatment and salvage with nonsurgical treatment. Other descriptive statistics are detailed in Table 1.
Bivariate Analysis
After dividing all cases into two groups by survival status, the survival group consisted of 186 patients and the nonsurvival group consisted of 215 patients. Comparison of variables between the two groups is presented in Table 1. A significant difference existed in the distribution of age between the two groups (χ2 value = 12.36, P = 0.006). In addition, the proportion of nonsurgical-treated cases was higher in the nonsurvival group (χ2 value = 6.98, P = 0.006). Furthermore, there were significant differences between the two groups in initial tumor stage, initial treatment, previous neck dissection, recurrence interval, and recurrent tumor stage. On the other hand, there was no significant difference between the two groups in gender, histological grade, and primary tumor site.
Descriptive, bivariate, and Kaplan-Meier analyses of oral cancer patients with relapse
SRAR, survival rate after relapse; RT/CT, radiotherapy with/without chemotherapy; WD, well differentiated; MD, moderately differentiated; PD, poorly differentiated or undifferentiated.
Among continuous variables, recurrence interval was longer in the survival group (25.4 ± 18.0 months vs 16.2 ± 12.9 months, t value = -5.78, P < 0.001) and survival duration after recurrence was shorter in the nonsurvival group (12.2 ± 14.1 months vs 27.6 ± 24.7 months, t value = −7.56, P < 0.001).
Survival Analysis
Based on the Kaplan-Meier survival analysis, the 5-year survival rate after recurrence in oral cancer patients was 31.56 percent. There was a significant difference in the 5-year survival rate after recurrence between those who received surgical and nonsurgical treatments (34.19% vs 20.72%, P < 0.001). In addition, there was a significant difference among several age groups (P = 0.006) and this was also the case for histological grade, initial tumor stage, initial treatment, second recurrence, and recurrent tumor stage.
By using receiver operating characteristic (ROC) curve, a proper cut-off point at which to divide the cases into two groups was identified (recurrence interval ≥18 months and recurrence interval <18 months). A significant difference was noted in 5-year survival rate after recurrence between the two groups (38.16% vs 27.55%, P < 0.001).
Conversely, there were no significant differences in the 5-year survival rate after recurrence in gender and primary tumor location. Detailed data are listed in Table 1.
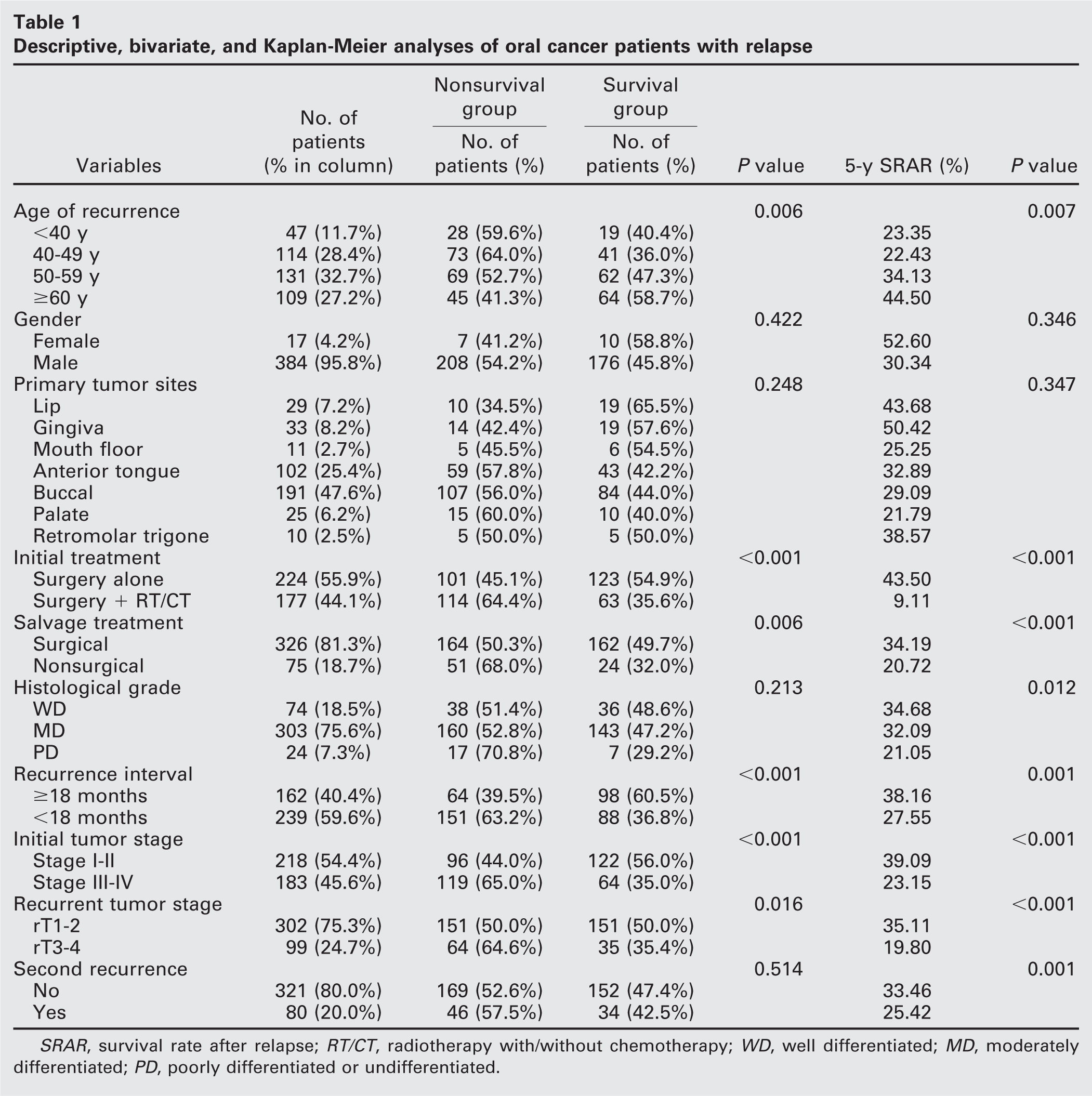
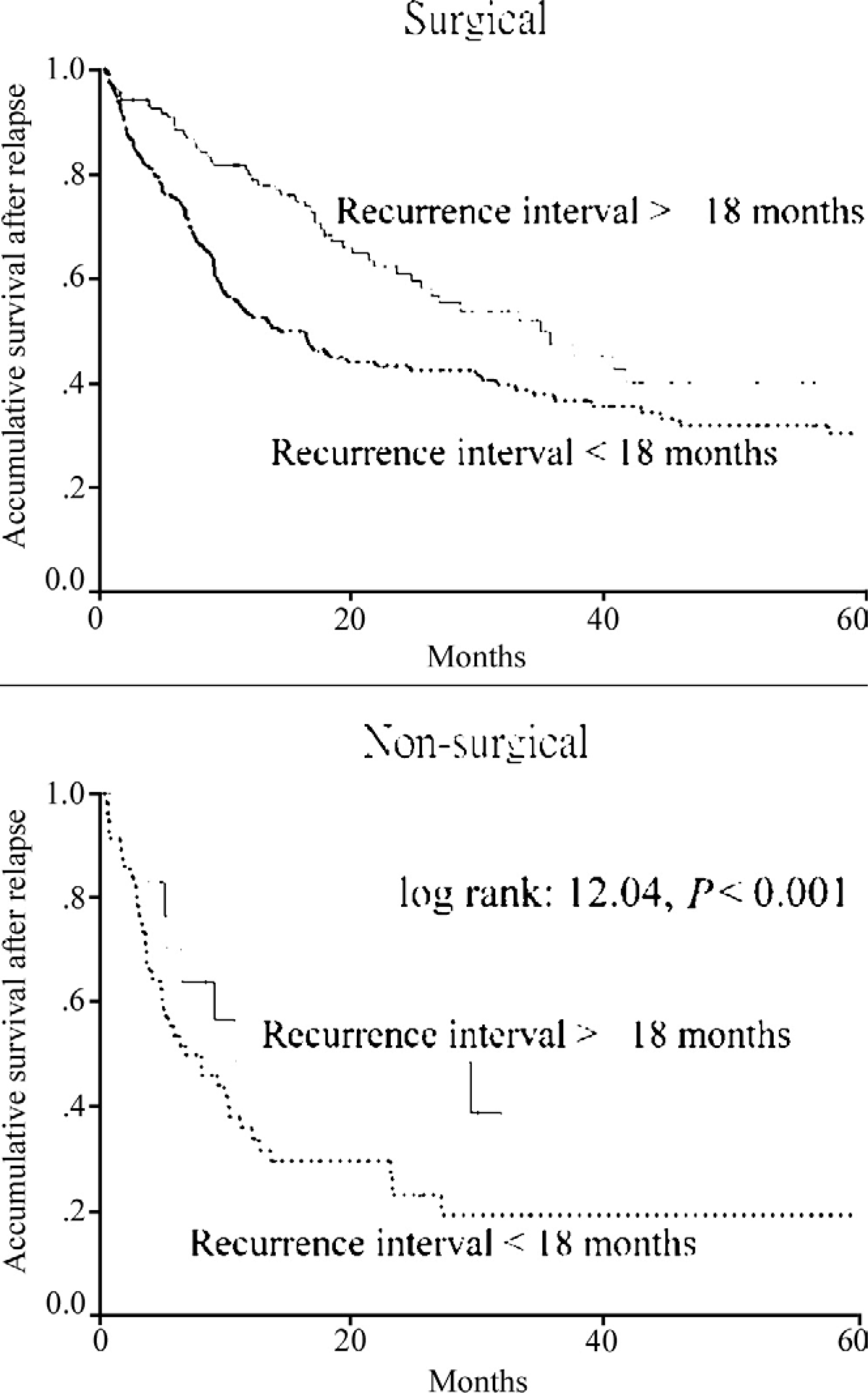
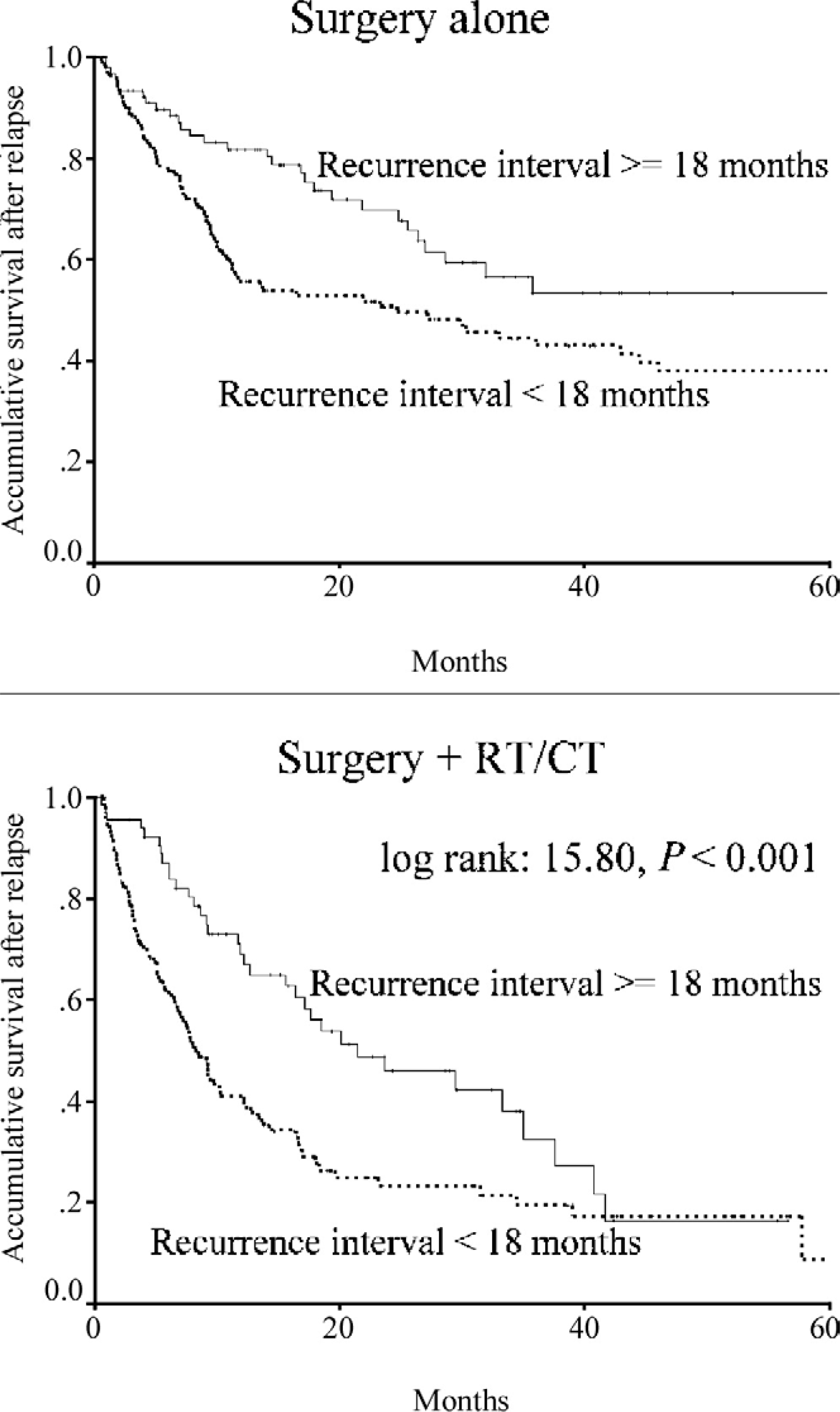
In order to clarify the relationship between recurrence interval and other major prognostic variables, a series of Kaplan-Meier curves were made. When stratified according to the type of salvage treatment, recurrence interval was still of prognostic value (log rank: 12.04, P < 0.001) (Fig 1). Similarly, when stratified according to initial treatment modality (log rank: 15.80, P < 0.001) (Fig 2), recurrent tumor stage (log rank: 11.89, P < 0.001) (Fig 3), and initial tumor stage (log rank: 10.26, P = 0.001) (Fig 4), recurrence interval was still a good prognostic indicator for survival of oral cavity squamous cell carcinoma patients after relapse.
Univariate analysis of the effect of recurrence interval on overall survival after relapse stratified according to the salvage treatment modalities (P < 0.001).
Univariate analysis of the effect of recurrence interval on overall survival after relapse stratified according to initial treatment modality (P < 0.001). RT/CT, radiotherapy with/without chemotherapy.
Cox Proportional Hazard Model
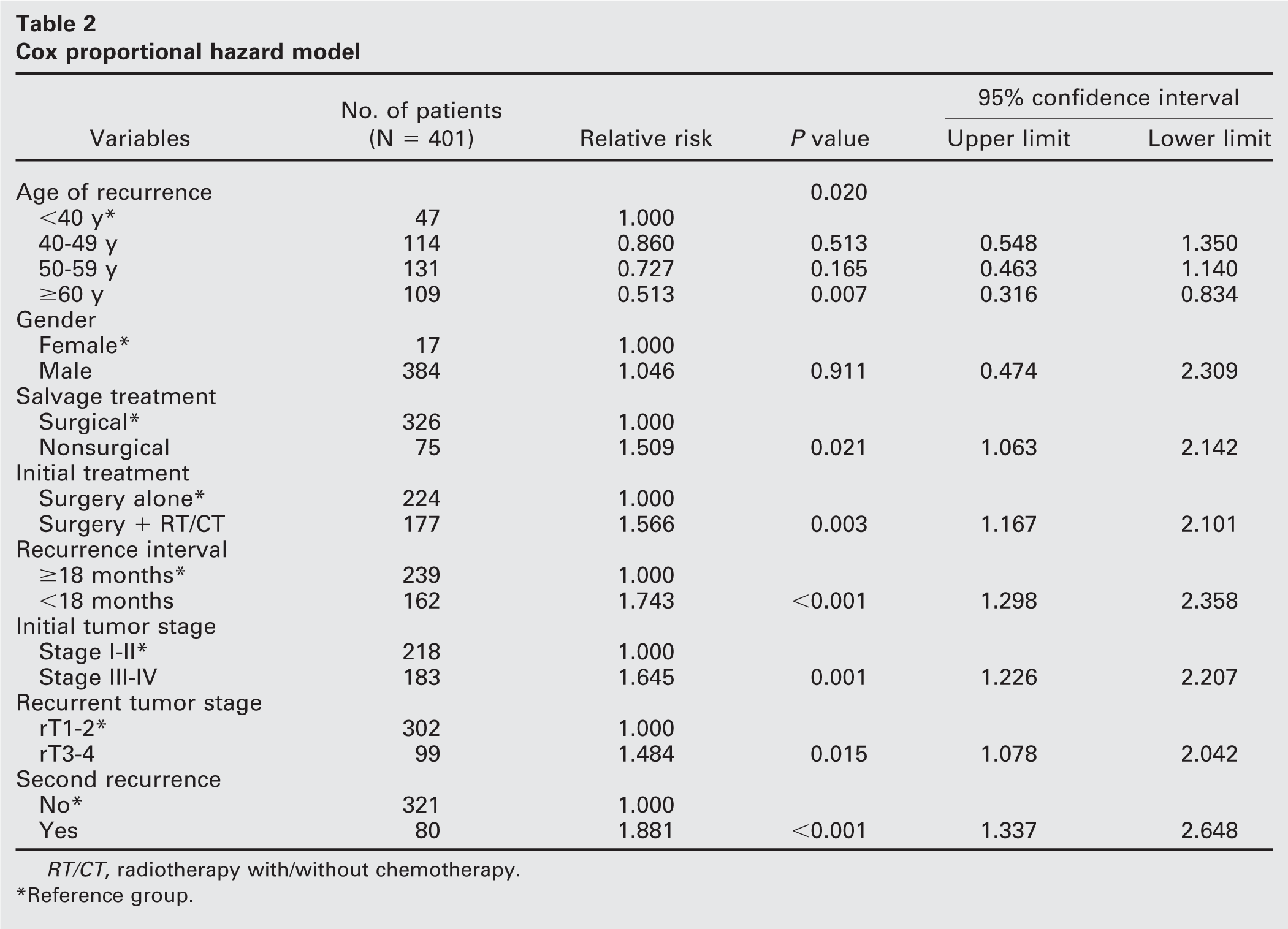
Based on gender, there was no significant difference in Cox proportional hazard model (P = 0.911). Based on age factor, the prognosis after recurrence was best for those aged more than or equal to 60 years compared with those less than 40 years old and the relative risk (RR) was 0.513 (95% confidence interval [CI]: 0.316–0.834, P = 0.007). Those with a recurrence interval less than 18 months had a poorer prognosis than those with a recurrence interval greater than or equal to 18 months (RR: 1.743, 95% CI: 1.298–2.358, P < 0.001). The detailed results are shown in Table 2.
Discussion
In this hospital-based study, over 400 oral squamous cell carcinoma patients with local relapse were analyzed and buccal mucosa was found to be the most common site of local recurrence. This is probably due to the high incidence of buccal cancer in Taiwan.12,13 The overall 5-year survival rate after local recurrence was found to be 31.3 percent, which is similar to that found in another study.7
Univariate analysis of the effect of recurrence interval on overall survival after relapse stratified according to the recurrent tumor stage (P < 0.001).
This study demonstrates that the recurrence interval significantly correlated with survival of oral cavity cancer patients after local relapse. It is thus comparable with other studies of a similar nature.9 However, controversy exists about the definition of recurrence. Recurrences within 6 months after completion of initial treatment might actually be showing evidence of residual disease. That is why this study included recurrences starting at least 6 months after a definite end of therapy. Another weakness of previous research was the length of study period (4 decades), during which there were most probably significant changes in the management of head and neck cancer. Goncalves Agra et al, in their study of prognostic factors in salvage surgery for recurrent oral and oropharyngeal cancer, also showed that those with a disease-free interval greater than 1 year had a favorable prognosis.14 Although the result was similar to ours, the studied populations were somewhat different. First, they included oral cavity and oropharyngeal cancer patients, whereas our study included only oral cavity cancer patients. Second, they enrolled various types of recurrent patients, while our study only enrolled local recurrent patients. Last, the majority of their patients belonged to the advanced recurrent stage group (n = 195, 79.3%), whereas most of our patients were in early recurrent stage (rT1–2; n = 302, 75.3%). The reason why those with a shorter recurrence interval could anticipate an unfavorable outcome might be due to more aggressive cancer behavior. In addition, Meyza et al had mentioned that late recurrences usually developed from a few cancer cells, which were wrapped by a fibrotic postir-radiation scar and were restricted to a smaller area that is easier to be removed by surgical excision.15 Furthermore, the reason most of our patients were diagnosed in the early stage might be explained by the fact that all our patients presented with oral cavity cancer that made recurrent tumors relatively easy to detect.
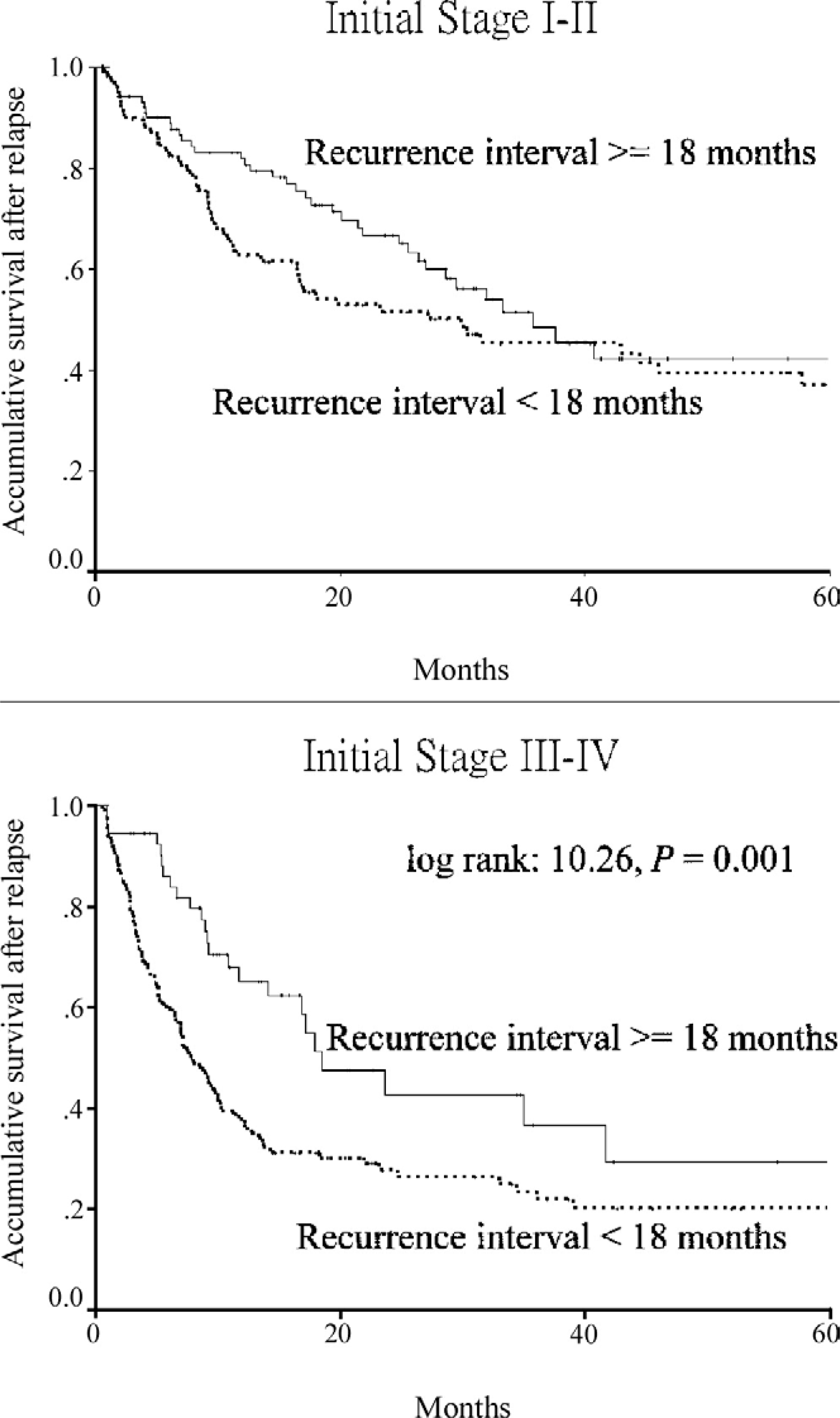
Univariate analysis of the effect of recurrence interval on overall survival after relapse stratified according to the initial tumor stage (P = 0.001).
Cox proportional hazard model
RT/CT, radiotherapy with/without chemotherapy.
Reference group.
This study found that the prognosis after recurrence was best for those who recurred after an age of 60 years compared with those who recurred at an age of less than 60 years. Few studies have been conducted on age of recurrence and the prognosis of oral cancer patients. However, there is conflicting evidence of the impact of age on oral cancer prognosis.16 Genetic instability might be the reason younger patients had a poorer prognosis. It has been suggested that patients without typical risk factors such as smoking or betel nut chewing habits may also have a poorer prognosis. Sarkaria et al, in their review of oral tongue cancer in patients under 40 years of age, found that younger patients had a poorer prognosis despite the fact that 64 percent of them had either stage I or stage II disease at presentation.17 This implies that the biological behavior of oral squamous cell carcinoma in younger patients might be different from that occurring in the older patients.
Salvage surgery is considered the treatment of choice for locoregional recurrences of oral and oropharyngeal cancers, especially when original therapy included irradiation.10,14 In this study, those treated surgically had a better prognosis when compared with those treated with nonsurgical methods. Other studies also obtained similar results.9,18 This could be explained by the fact that early recurrent tumors tended to be treated surgically, as 87.1 percent of rT1–2 cases were treated with salvage surgery while only 63.6% of rT3–4 cases received salvage surgery in this study. In addition, reirradiation has significant technical limitations regarding the dose and toxicity.14 Another study also found higher complication rates associated with reirradiation.19 Consequently, those treated with nonsurgical treatment were more likely to have a poorer outcome.
Although our study showed that those who received initial surgical treatment plus radiotherapy with or without chemotherapy tended to have a shorter survival period, other studies have shown an opposite result.10 The different studied populations might explain these conflicting outcomes. Those who received previous radiation implied advanced disease in initial presentation. Therefore, salvage treatment might be inadequate in such cases, either due to vague resection margins or due to complications from reirradiation.
It is easy to understand that those with higher initial tumor stage, advanced recurrent stage, or multiple recurrent tumors were prone to poorer prognosis inasmuch as all these features represent severe disease status. Furthermore, adequate resection or other adjuvant therapies were hard to implement in such patients. Many studies also addressed the importance of restaging in predicting the outcome of head and neck malignancies.9,10,14
There were some limitations in this study. First, external validity of the results is limited because the study was conducted at a single institution and included only patients admitted for potentially therapeutic treatments. Second, this was a cross-sectional study, not a cohort study, and therefore it was difficult to elucidate causal relationships. Third, although treatment protocol is standardized in our institute, individual differences among surgeons inevitably exist. Finally, as only 401 out of 1687 patients (23.8%) were included for final analysis, selection bias could possibly have influenced our conclusions.
Conclusion
This hospital-based study retrospectively reviewed over 1000 oral cavity squamous cell carcinoma patients and found that the local recurrence rate was 31.3%. We also found the 5-year survival rate after local recurrence to be 31.56%. Apart from clinical signs (eg, recurrent tumor stage, previous radiation, salvage methods), the recurrence interval significantly influenced the survival of oral cavity cancer patients after relapse. Early detection of recurrence is still crucial as favorable outcomes were noted in those with small recurrent tumors.
The authors thank Dr Shou-Yee Chao, Dr Ying-Lyung Hsiao, Dr Man-Yee Chan, Dr Chi-Sheng Cheng, Dr Chen-Chi Wang, and Dr Ching-Ping Wang for kindly providing their patients for investigation. The authors also thank Ms. I-Zu Jiang for the assistance of computer file processing and Ms. Hui-Ching Ho for statistical consulting.