
Abstract
Objective
To identify the indications and outcomes of total thyroidectomy for Graves' disease in a North American cohort.
Study Design and Setting
Prospective database of 297 patients undergoing total thyroidectomy in a tertiary care center identified 49 patients with Graves'.
Results
There were 37 women and 12 men (mean age, 37.9 years). Common indications for surgery were: refusal of radioactive iodine (20%), thyroid storm (18%), a thyroid nodule (16%), failure of I131(14%), and ophthalmopathy (14%). Complications included: symptomatic hypocalcemia (14%), permanent hypoparathyroidism (0%), and symptoms of recurrent laryngeal nerve injury (0%). Graves' patients had more bleeding (117 mL versus 48 mL, P < 0.05). Clinical nodules were malignant in 38%. Papillary thyroid carcinoma occurred in 10% of patients, with 60% multifocal, and 60% lymph node metastases.
Conclusion
Total thyroidectomy for Graves' has minimal morbidity. Patients with Graves' and a thyroid nodule are at an increased risk for malignancy and should be treated with a total thyroidectomy.
The current indications, patient demographics, and outcomes of total thyroidectomy for Graves' disease in North America have rarely been reported. This study was conducted to evaluate the current indications for total thyroidectomy and to identify any demographic data that may influence a patient's decision to proceed with surgical management. An outcome comparison between patients with Graves' and those without Graves' who underwent total thyroidectomy was also completed to assess factors that may relate to intraoperative and postoperative complications.
Methods
A review of a prospective database of 297 patients who underwent a total thyroidectomy between 1999 and 2005 identified 49 patients with Graves' disease. Patients undergoing reoperative neck surgery, lymphadenectomy, or those on chronic anticoagulation therapy were excluded. The medical records of these 49 patients were retrospectively reviewed for patient age, gender, race, and preoperative thyroid function tests. The operative notes were reviewed for surgical indication, estimated blood loss, and any intraoperative complications. Postoperative parathyroid hormone levels, serum or ionized calcium results, complications, and hospital course were evaluated. The pathology reports were reviewed for the weight of the thyroid gland, the primary and the coincident pathology findings. The patients with Graves' disease were then compared with 123 consecutive non-Graves' patients undergoing total thyroidectomy to identify any differences in patient demographics and complications.
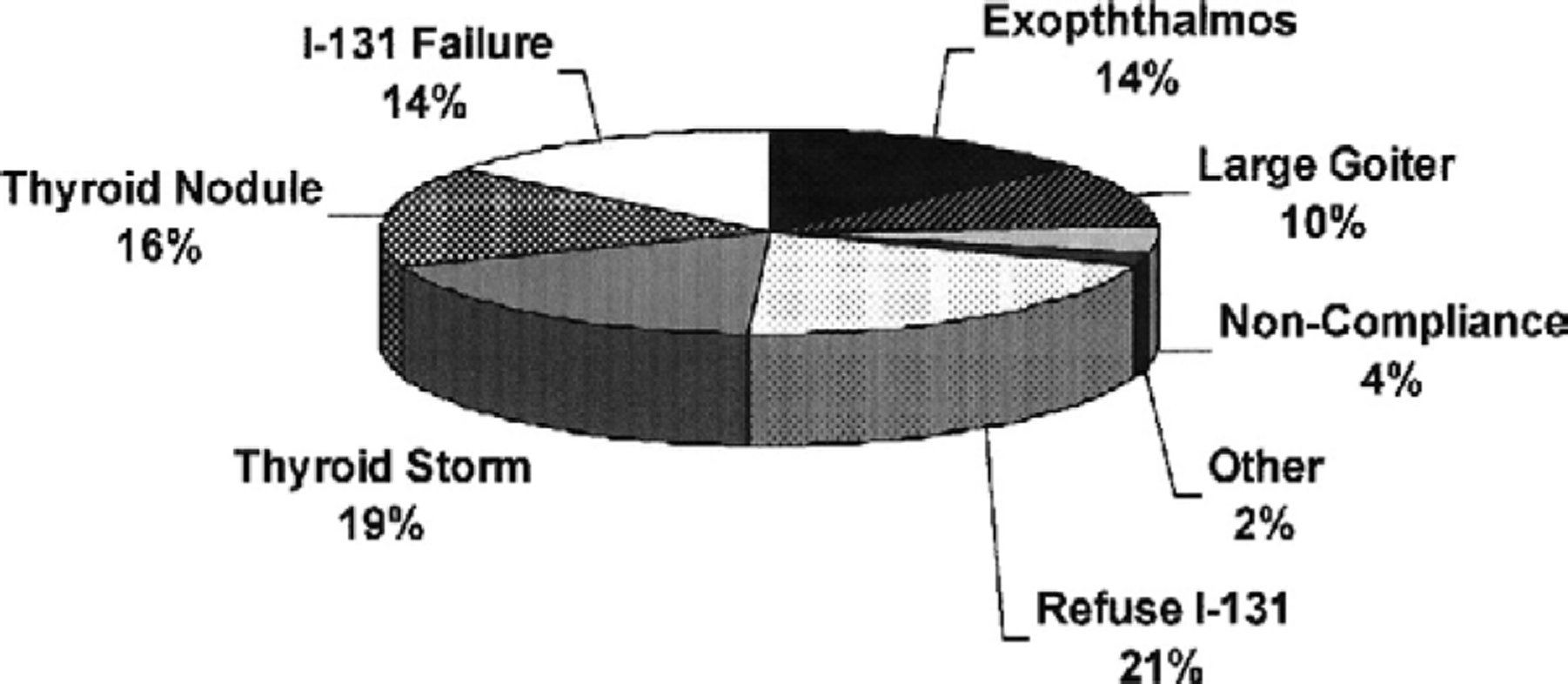
Indications for surgery in 49 patients with Graves' disease undergoing total thyroidectomy.
Statistical analysis was performed using Students t test and chi-squared where appropriate. All statistical analysis was done with SPSS 14.0 for Windows and statistical significance was set at P < 0.05. This study was approved by the University of Texas Health Science Center at San Antonio's Institutional Review Board.
Results
The 49 patients with Graves' disease included 37 women and 12 men (mean age, 37.9 ± 15.6 years). There were 30 Hispanics, 11 whites, and 8 African Americans. The reasons for surgical referral included: refusal of radioactive iodine in 10 (20.4%) patients, thyroid storm that required urgent intervention in 9 (18.4%) patients, a concurrent thyroid nodule in 8 (16.3%) patients, failure of radioactive iodine in 7 (14.3%) patients, and Graves' ophthalmopathy in 7 (14.3%) patients (Fig 1). There were 2 patients who were noncompliant and 1 patient with hepatic failure as a result of the Graves' disease. No patient was referred for surgery because of pregnancy. Seven of 8 patients with thyroid nodules had them detected as cold defects on their initial I-123 uptake scans. Thyroid ultrasound was not routinely performed in all patients with Graves' disease. There was no correlation between the indication for surgery and patient age, race, gender, or thyroid size (P < 0.05).
The free thyroxine levels were normalized preoperatively in 51% of patients (mean, 2.4 ± 1.8 ng/dL). All patients received thionamides, beta-blockade, and potassium iodide preoperatively. The average estimated intraoperative blood loss was 116.7 ± 217.7 mL. Two patients each received 2 units of red blood cells. No patients required re-exploration. Excluding the 9 patients who were in thyroid storm preoperatively, there were no cases of intraoperative thyroid storm. The average weight of the gland was 59.6 ± 51.2 gm. Postoperative intact parathyroid hormone (PTH) levels were below the reference range in 12% of patients (mean, PTH 44 ± 46 pg/mL). There were 8 (14%) patients who developed transient symptomatic hypocalcemia. The average length of hospital stay was 2 ± 4 days. All patients who were electively admitted were discharged in less than 23 hours. There were no patients with permanent hypoparathyroidism, and no patient had symptoms consistent with a recurrent laryngeal nerve injury.
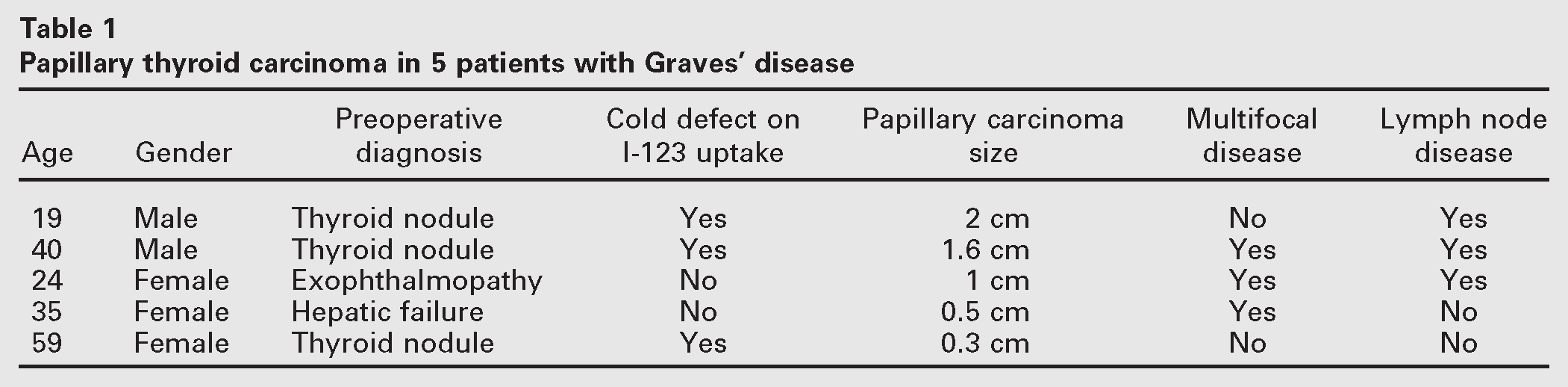
The final pathology reports found papillary thyroid carcinoma in 5 (10%) patients. There were microscopic lymph node metastases present in 3 patients. These nodes were perithyroidal and not clinically evident. No patient with a tumor less than 1 cm had lymph node metastases. The carcinoma was multifocal in 3 patients (Table 1). Three (37.5%) of 8 patients who presented with a thyroid nodule had papillary thyroid carcinoma.
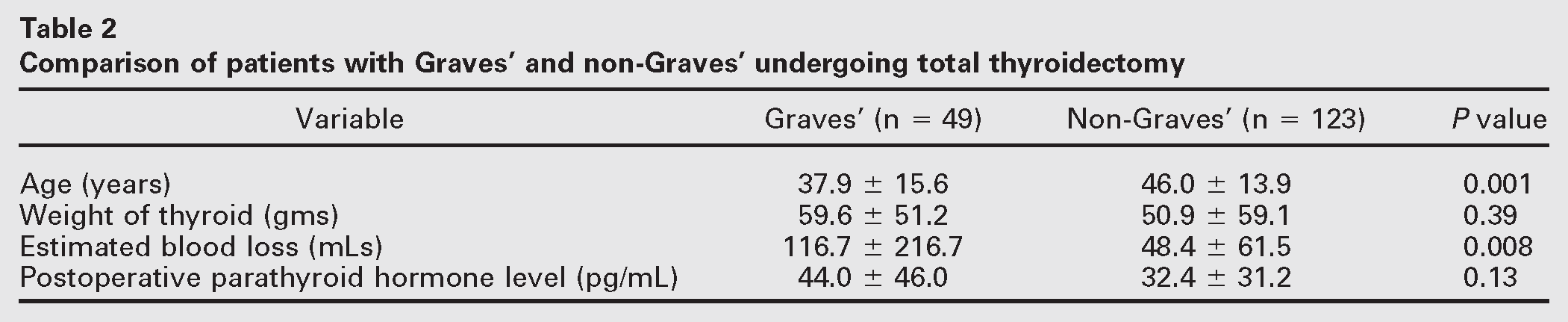
A comparison between the patients with Graves' and non-Graves' patients who underwent total thyroidectomy is shown in Table 2. There were 11 (8.9%) men and 112 (91.1%) women who underwent total thyroidectomy for non-Graves' pathology. Significantly more men (24.5%) underwent total thyroidectomy for Graves' (P < 0.05). There were also significantly more Hispanic patients who underwent total thyroidectomy for Graves' than non-Graves (61.2% vs 43.4%). The patients with Graves' were significantly younger (mean age, 37.9 vs 46.0 years). There was no difference between the 2 groups with respect to the weight of the thyroid gland or the postoperative PTH levels. There was 1 (0.8%) patient in the non-Graves' group who had permanent hypoparathyroidism. None of the patients had symptoms consistent with a recurrent laryngeal nerve injury in either group. Direct visualization of the vocal cords on clinical follow-up was not routinely performed. Patients with Graves' had significantly more blood loss (mean, 116.7 vs 48.4 mL) and were more likely to get a blood transfusion. No patient in the non-Graves' group required a blood transfusion compared with 2 patients with Graves'. All of the Graves' patients and 99.2% of the non-Graves' patients that were electively admitted were discharged within 24 hours.
Papillary thyroid carcinoma in 5 patients with Graves' disease
Comparison of patients with Graves' and non-Graves' undergoing total thyroidectomy
Comment
This study showed that total thyroidectomy continues to remain a treatment option for patients with Graves' disease when factoring in patient characteristics such as gland size, exophthalmopathy, failure or refusal of I-131 treatment, and the presence of thyroid nodules. Total thyroidectomy provides an immediate and 100% curative treatment for hyperthyroidism. It may alleviate Grave's orbitopathy whereas radioactive iodine therapy may exacerbate the orbitopathy.1,6 Total thyroidectomy can also provide surgical treatment for papillary thyroid carcinoma. It can be done with minimal risks of permanent hypoparathyroidism and recurrent laryngeal nerve injury. It is an operation that can be performed as an outpatient procedure. The majority of the patients in our study were elective admissions with a 23-hour observation period.
The only difference in complications between Graves' and non-Graves' patients who underwent total thyroidectomy was that the estimated blood loss for Graves' patients was significantly greater than non-Graves' patients (117 mL vs 48 mL). The increased blood loss is most likely the result of the hypervascularity of the gland. We were unable to identify any other study that had compared total thyroidectomy between Graves' and non-Graves' patients. However, Ku et al7 compared total thyroidectomy to subtotal thyroidectomy in Graves' disease. They had comparable results to our study with an estimated blood loss for their total thyroidectomy in Graves' disease (100.6 ± 268.6 mL). This was significantly less than their estimated blood loss for a subtotal thyroidectomy in Graves' disease (202.1 ± 489.4 mL; P < 0.001). The higher blood loss from Graves' patients may be reduced with the use of beta blockers and potassium iodide. Our patients received potassium iodide for a minimum of 3 days preoperatively. A literature review identified only theoretical and nonobjective evidence that beta-blockade reduced the vascularity in Graves' disease. Color-flow Doppler and radionucleotide studies have confirmed that the vascularity of the thyroid gland in Graves' disease is significantly reduced after a 2-week course of potassium iodide.8,9 There was no effect of carbimazole on the vascularity. However, carbimazoles and thioamides are often necessary to obtain a euthyroid state and prevent intraoperative thyroid storm.9 An increase in the duration of potassium iodide therapy to 2 weeks may result in a decrease in blood loss.
It has been shown that the resected Graves' thyroid glands have an increased likelihood of containing carcinomas with the majority of the carcinomas of papillary origin.10,11 In our study, 10% of the Graves' patients were found to have papillary thyroid carcinoma; 60% of these were multifocal and 60% had microscopic lymph node metastases. The rate of malignancy in Graves' ranged between 8% to 17% in 2 recent North American studies.4,5 This incidence is higher than the 0 to 9.8% range that was reported in a review of 20 studies that were mainly of European and Asian origin.10 These 20 studies had a total of 221 reports of papillary thyroid carcinoma in 6580 patients who underwent total thyroidectomy for Graves' disease for an overall incidence of 3.4%. Many of these studies also included occult papillary carcinomas. Our incidence of papillary thyroid carcinoma in North America may be higher because total thyroidectomy is not a primary therapy for Graves' disease in our country. We are operating on patients because they have a thyroid nodule, not just because they have Graves' disease.
Patients with Graves' disease and a thyroid nodule are all referred to surgery at our institution. The majority of these nodules were found because of cold defects on I-123 uptake scans. These patients with cold defects were then referred for a thyroid sonogram. When a nodule was found on a sonogram obtained for a cold defect or on physical examination, it had a 37.5% chance of malignancy. This supports a recommendation for total thyroidectomy in patients with Graves' disease and a thyroid nodule. Kraimps et al11 reported on 557 patients operated on for Graves' disease in France. They performed an ultrasound on every patient and found a 25% incidence of thyroid nodules. Papillary thyroid carcinoma was present in 15% of these nodules. In addition to a total thyroidectomy for a thyroid nodule, these authors have recommended routine thyroid ultrasonography in all patients with Graves'. Routine ultrasonography in Graves' disease was recently reported in a prospective study of 245 patients in Korea by Kim et al.12 They found a 35% incidence of thyroid nodules. A fine-needle aspiration biopsy was performed in 90% of patients with nodules greater than 5 mm in size (62 patients); 13% of these patients had papillary thyroid carcinoma. The high incidence of thyroid cancer in our patients with Graves' disease and a thyroid nodule does not support the use of routine fine-needle aspiration. In addition, there may be cytological limitations and increased risks for obtaining a biopsy in a hyperthyroid patient with a vascular thyroid gland. Although thyroidectomy is safe in experienced hands, the risks and benefits of a fine-needle aspiration should be compared to the risks of thyroidectomy performed by an inexperienced surgeon.
We have found that patients with Graves' disease have an increased incidence of multifocal papillary carcinoma (60%) and lymph node metastases (60%). The prognostic significance of these findings is controversial. A review by Loh et al13 of 700 patients with differentiated thyroid carcinoma reported significantly increased risk ratios (RR) for recurrence in patients with either multifocal disease (RR, 2.1) or nodal metastases (RR, 4.2) (P < 0.05). There was an increased risk of thyroid cancer-related deaths in patients with multifocal disease (RR, 1.9) or nodal metastases (RR, 2.6), however, this risk was only significant for patients with nodal metastases (P < 0.05).13 Patients with more than 10 lymph node metastases or lymph node metastases in association with extracapsular extension of papillary carcinoma have been shown to have increased recurrence rates (21% vs 4% and 32% vs 1%). Capsular extension alone did not have a significantly increased recurrence rate.14 There are a number of large studies that have shown that lymph node metastases have no effect on either recurrence or survival.15,16
These results may or may not be applicable to patients with Graves' disease. An increased incidence of multifocal disease and lymph node metastases was also reported by Belfiore et al17 in a comparison between Graves' patients and euthyroid control patients with papillary thyroid carcinoma. In addition, they also found that patients with Graves' and papillary thyroid carcinoma were more likely to have invasive growth patterns and distant metastases. Patients with Graves' disease have been found to have 3 times the risk of recurrent or progressive metastases.18 It has been postulated that the high levels of antithyroid-stimulating hormone receptor antibodies in Graves' may stimulate cancer growth.10 This may be the stimulant that allows for the development of multifocal tumors, many of which have been shown to have independent clonal origins.19
This study confirmed that patients with Graves' disease can safely and effectively be treated with a total thyroidectomy. The most important finding in this study was the high incidence of papillary thyroid carcinoma in thyroid nodules associated with Graves' disease. These carcinomas are multifocal and have a high propensity for lymphatic spread. Routine ultrasonography should be strongly considered in all patients with Graves' disease. Total thyroidectomy should be recommended as the treatment of choice for patients with Graves' disease and thyroid nodules. The role of routine cervical lymphadenectomy in these patients needs further investigation.