
Abstract
Objective
To assess if participation by patients in a head and neck cancer support group improves perceived quality of life (QOL).
Study Design and Setting
Subjects for this study included 47 patients at a tertiary Veterans Affairs Medical Center who were previously treated for head and neck cancer. This was a quasi-experimental, post-test study comparing the QOL of 24 patients who participated in a head and neck cancer support group with 23 patients who did not participate. The validated University of Michigan Head and Neck Quality of Life (HNQOL) instrument was used to evaluate head and neck cancer-related QOL.
Results
Patients who participated in the head and neck cancer support group exhibited significantly better scores in the domains of eating, emotion, and pain as well as in the global bother and response to treatment questions of the HNQOL instrument compared with those patients who did not participate. Additional subgroup analysis comparing age, type of treatment, and length of time since cancer diagnosis suggests that these variables were less important predictors of QOL than was support group participation.
Conclusions
Our findings suggest that patient participation in a head and neck cancer support group is associated with improved QOL.
Significance
Support groups may be beneficial in improving QOL after head and neck cancer treatment.
In recent years, new trends for head and neck cancer treatment include organ preservation chemoradiation protocols, less radical conservation surgeries, and more advanced reconstructive techniques, including the use of free-tissue transfer flaps.5, 6 Although maximizing survival remains paramount, the development of these newer strategies highlights a recent emphasis on improving function and ultimately QOL for patients with head and neck cancer. Additionally, a number of studies have attempted to determine the various demographic as well as clinical and treatment parameters that may influence QOL. 7 – 10 However, data are lacking with regard to the role of the support group as an adjunct to head and neck cancer treatment and the influence of patient participation in a support group on QOL measures.
Recently, there has been recognition of the need for better support interventions to help patients with head and neck cancer cope with the physical and psychosocial problems that arise as the result of the disease and its management.11, 12 Hammerlid and colleagues 12 published the results of a study of psychosocial intervention in patients with head and neck cancer. This study focused on long-term group psychological therapy for patients newly diagnosed with head and neck cancer. The psychosocial group therapy sessions stressed both cognitive and behavioral techniques. The QOL measures of emotion, social and cognitive functioning, pain, fatigue, and appetite loss of the therapy group improved more than that of the control group during the 1-year follow-up period. Although the authors acknowledged the shortcomings of their pilot study related to the small sample size and compliance issues among patients, their data do suggest that support interventions for patients with head and neck cancer may be beneficial.
Multidisciplinary support group meetings coordinated with regular cancer surveillance visits provide a simple, convenient forum for patients to confront various QOL issues with other similar patients and to benefit from nursing, nutritional education, speech pathology, and social work services. Support groups allow patients to educate themselves about their disease and its treatment options, learn new ways to cope and address new challenges, and discuss feelings and concerns in a supportive environment with health care professionals as well as other patients with cancer. 13 The objective of this study was to determine if patient participation in a multidisciplinary head and neck cancer support group would be associated with an improved perception of QOL.
Methods
Design
This was a quasi-experimental, post-test study comparing the QOL of patients who participated in a head and neck cancer support group with patients who did not participate.
Sample Population
Inclusion criteria for this study included patients who had previously undergone treatment for head and neck cancer and were currently receiving Otolaryngology-Head and Neck Surgery follow-up care at the San Francisco Veterans Affairs (VA) Medical Center. To avoid potential transient fluctuations in QOL scores in the immediate post-treatment period, patients who were less than 3 months beyond completion of their head and neck cancer therapy were excluded.
Procedures
A review of head and neck cancer support group attendance lists and head and neck clinic logs at the San Francisco VA from the previous 12 months identified approximately 76 patients who were eligible for this study. Patients were invited to participate in the study by recruitment letters mailed to eligible patients, with follow-up telephone calls made approximately 3 weeks later. Of the 76 eligible patients initially approached, a total of 47 patients (62%) agreed to participate in the study; patients were provided informed consent before enrollment. All study patients were offered an opportunity to join the head and neck cancer support group. Of the study patients, 24 attended the support group and 23 did not attend. After the support groups were conducted, all 47 study subjects were asked to complete the University of Michigan Head and Neck Quality of Life (HNQOL) instrument (Table 1) to determine differences in QOL between participants and nonparticipants of the support group.
University of Michigan Head and Neck Quality of Life (HNQOL) instrument
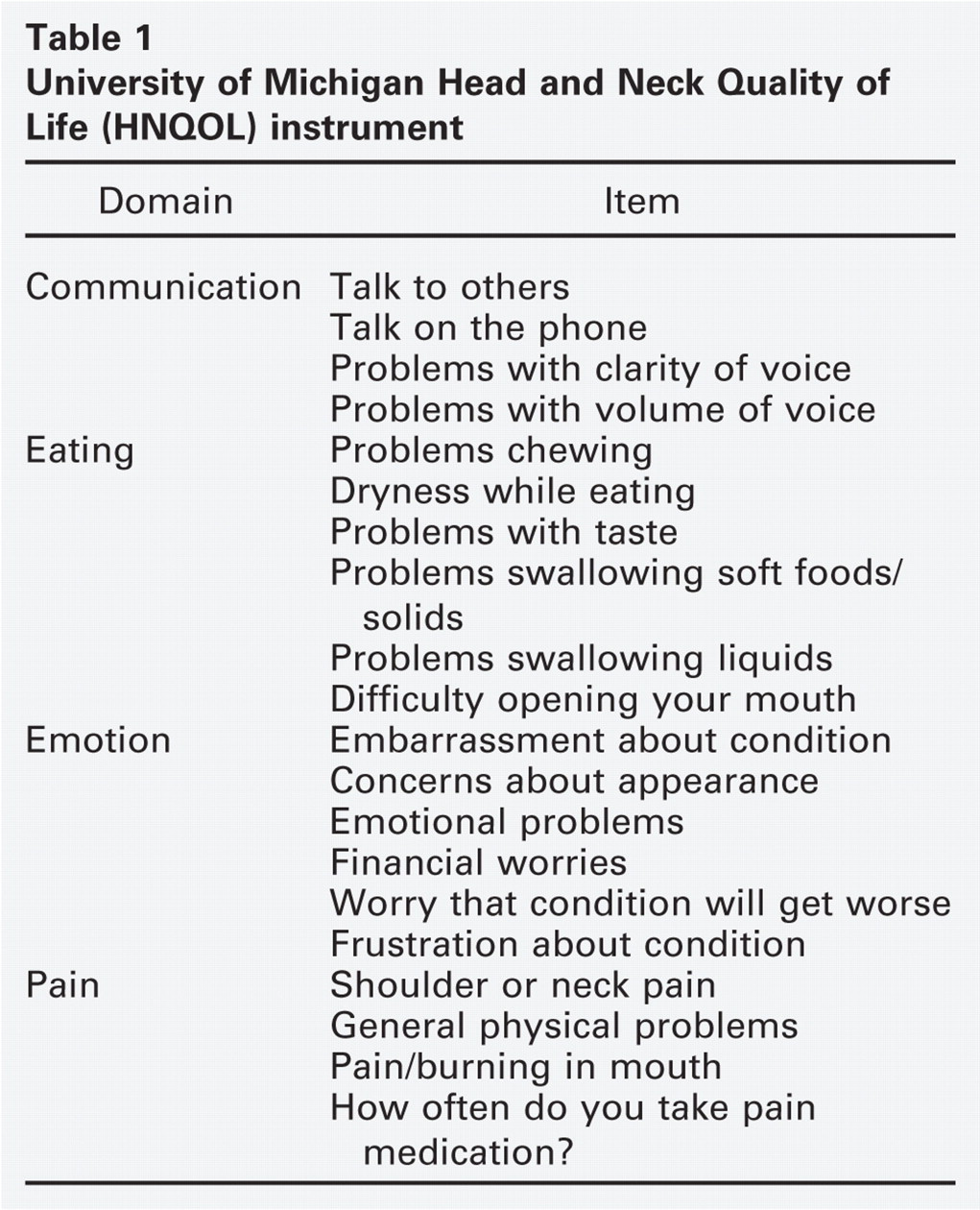
The HNQOL is a previously validated instrument that measures multiple emotional and functional facets of health specific to patients with head and neck cancer. 14 In the questionnaire, 20 questions evaluate four domains related to head and neck cancer on a five-point scale: head and neck pain (four items), eating and swallowing (six items), communication (four items), and emotional well being (six items). The HNQOL instrument also assesses a global or overall bother from symptoms related to patient's disease and treatment, a patient's assessment of his response to treatment, the length of time to answer the questionnaire, and the difficulty of completing the questionnaire. A standard scoring algorithm was used to generate scores from 0 to 100 in four QOL domains (eating, communication, emotion, and pain) as well as two general scores (global or overall bother and patient's own assessment of their response to treatment). A score of 0 is the worst, and a score of 100 is the best possible score. In the setting of missing items, the domain score was calculated for a particular patient if he answered at least half of the questions in the multi-item scale.
Medical charts of study participants were reviewed to obtain additional demographic and clinical data relevant to their head and neck cancer treatment. Institutional review board approval for this study was obtained from the University of California-San Francisco Committee on Human Research.
Description of Intervention
All patients at the San Francisco VA Medical Center who have undergone treatment for head and neck cancer were invited to participate in a 1 1/2-hour, biweekly, multidisciplinary head and neck cancer support group. Patient participation and attendance in the support group meetings were voluntary. Cancer surveillance visit clinic appointments with the physician were coordinated to follow support group meeting times, and patients who were participants in the support group typically attended meetings only on days when they also had a regularly scheduled clinic visit. The usual schedule of visits for cancer surveillance after treatment was once monthly for the first year, once every 2 months for the second year, once every 3 months for the third year, and once every 6 months thereafter. Patients who participated in the support group more than once in the previous 12 months were considered to be participants for the purposes of this study. Of study patients in the participant group, the minimum number of group meetings attended was 2, the maximum number attended was 17, and the mean number attended was 6. The support group meetings included patients with head and neck cancer, a head and neck nurse, a dietitian, a speech pathologist, and a social worker. The structure of the group meetings was flexible and open-ended. It was intended to be a forum for patients to confront issues regarding their disease or treatment as well as to benefit from the various health and social services available through the VA system.
Statistical Methods
Descriptive statistics (means and frequencies) were computed for all variables. Continuous variable data are presented as mean ± standard deviation (SD). A two-sided t test was used to compare HNQOL scores between those who participated in the support group vs those who did not. Two-sided t tests were also used to compare differences in other QOL variables, including age (>65 years old vs <65 years old), type of cancer treatment (surgery vs nonsurgery), history of laryngectomy, and length of time since diagnosis (>2 years vs <2 years). A two-sided P value of <0.05 was considered statistically significant.
Results
Demographic and Clinical Results
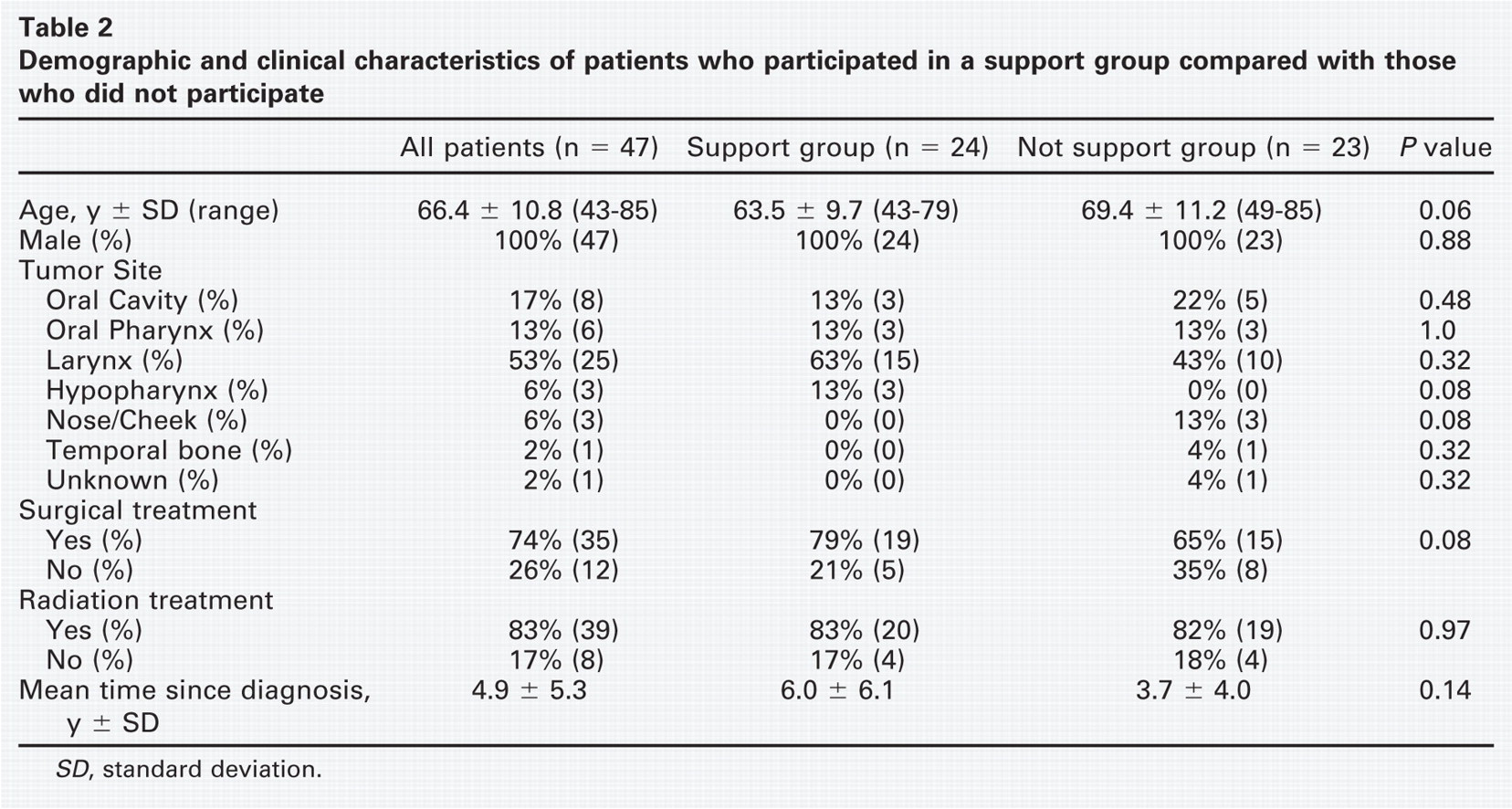
The demographic and clinical results of the study patient population along with the subgroups of patients who participated in the support group and those patients who did not participate in the support group are presented in Table 2. There was some variation in the clinical characteristics of the two subgroups, but none of these differences were statistically significant. All patients in the study were male, with a mean age of 66.4 ± 10.8 years. There was a trend toward patients participating in the support group being younger than those who did not participate in the support group (63.5 ± 9.7 vs 69.4 ± 11.2 years; P = 0.06). Furthermore, patients who belonged to the support group tended to have a mean time since cancer diagnosis that was longer than those not in the support group (6.0 ± 6.1 vs 3.7 ± 4.0 years; P = 0.14). Among patients participating in the support group, there were slightly more patients with laryngeal cancer (15 vs 10; P = 0.32), and 10 of the 12 patients in the study who had a total laryngectomy belonged to the support group. A greater number of patients in the support group had undergone surgery as part of their treatment (19 vs 15; P = 0.08), whereas the number of patients having received radiation therapy was similar between the two groups (20 vs 19).
Demographic and clinical characteristics of patients who participated in a support group compared with those who did not participate
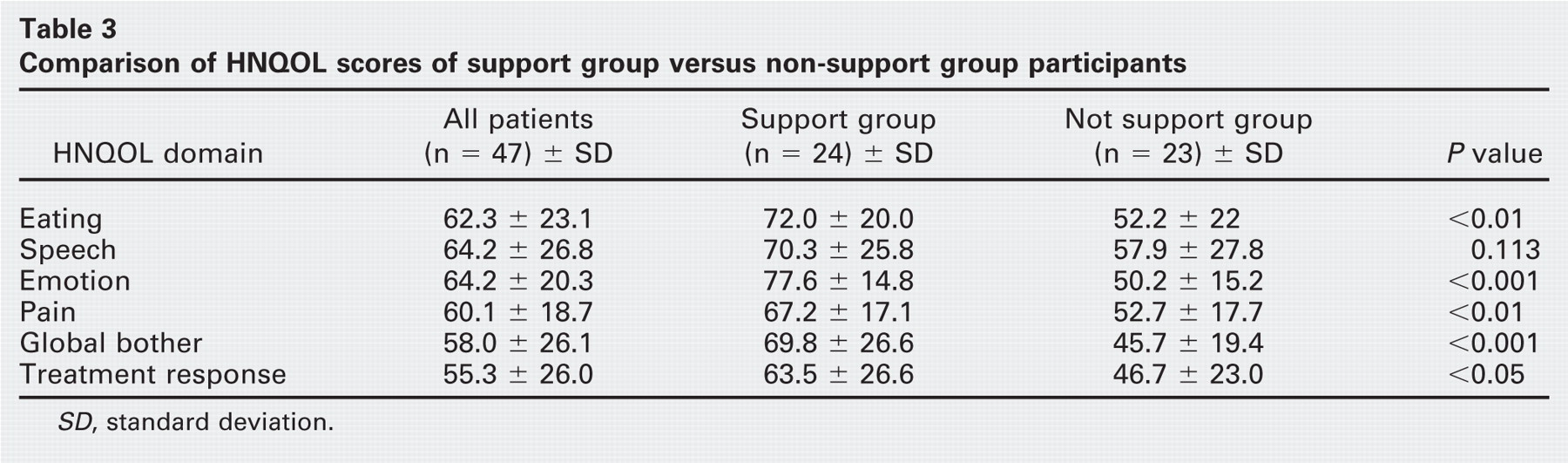
Comparison of HNQOL scores of support group versus non-support group participants
Hnqol Scores
HNQOL scores for the entire study population are presented in Table 3. Patients who attended the support group had statistically significant higher scores than those patients who did not attend a support group in three HNQOL domains: eating (72 vs 52.2, P = 0.002), emotion (77.6 vs 50.2, P < 0.001), and pain (67.2 vs 52.7, P = 0.006). Patients in the support group also reported statistically significant higher scores in the patients' assessment of global bother (69.8 vs 45.7, P < 0.001) and treatment response (63.5 vs 46.7, P = 0.02). In the HNQOL domain of speech, the difference in scores between participants of the support group (70.3) and nonparticipants (57.9) was not statistically significant (P = 0.113).
To assess the impact that other treatments or patient characteristics may have had on the HNQOL scores, additional subgroup analysis was performed. There were no statistically significant differences in HNQOL scores between patients who had surgery as a treatment modality and those who did not have surgery. When comparing the subgroup of patients who were treated with a total laryngectomy with those who were not, there were no significant differences in HNQOL scores except for the domain of speech. Not surprisingly, patients without a total laryngectomy had significantly higher HNQOL speech scores compared with patients in the total laryngectomy subgroup (69.5 ± 27.1 vs 49 ± 19.7, P = 0.009). Because a patient's age may affect QOL, we also compared HNQOL scores of younger vs older patients. There was no significant difference in HNQOL scores in this study between patients younger than 65 years compared with those who were older than 65 years. The length of time since cancer diagnosis may also affect QOL, allowing more physical and psychological adjustment. We compared patients who were diagnosed with cancer more than 2 years ago with those who were diagnosed with cancer less than 2 years ago and found that patients who were more than 2 years removed from their cancer diagnosis had statistically significant higher HNQOL scores in the domain of emotion (70.7 ± 20.6 vs 57.4 ± 18; P = 0.02) and in the overall bother category (65.6 ± 27.4 vs 50 ± 22.6; P = 0.04); other HNQOL domains were not significantly different between the two subgroups. Thus, among the various variables that were analyzed in this cross-sectional study (support group participation, cancer treatment [surgery vs nonsurgery], history of laryngectomy, age, length of time since diagnosis), participation in a head and neck cancer support group was the most correlated with better HNQOL scores.
Discussion
Cancer support group interventions have been studied previously in melanoma, Hodgkin's lymphoma, colon cancer, and especially breast cancer. 15 – 21 These studies have demonstrated that support group participation is associated with significant improvements in emotional state (depression and anxiety), adaptation to disease, and marital relationships. 16 Notably, the vast majority of literature regarding cancer support groups has involved studies of women with breast cancer.15, 18–21 The role of cancer support groups for the predominantly male population found in the VA system has not been extensively investigated. Our study of patients with head and neck cancer at a VA Medical Center demonstrated an association between cancer support group participation and QOL. The results of this study demonstrated improved QOL in the domains of eating, emotion, and pain among patients who participated in a head and neck cancer support group compared with those who did not participate. Furthermore, support group participants tended to be less bothered by their cancer and its treatment and reported a better response to treatment than their nonparticipating counterparts. There was also a trend toward better HNQOL scores in the domain of speech among support group participants, although this difference did not achieve statistical significance. These results corroborate observations of others on the effect that support groups may have on the QOL of patients with cancer.
The QOL impact of head and neck cancer may also vary, depending on multiple other factors including the tumor site, type of treatment, and length of time since diagnosis, and there were small differences in these variables between the two groups. For example, there were slightly more patients with laryngeal cancer who were participants in the study group (15 vs 10), and there is evidence that patients with laryngeal cancer perceive better QOL compared with patients with oral cavity, oropharyngeal, and hypopharyngeal cancer. 22 Patients with total laryngectomy had lower HNQOL speech domain scores, which may explain why there was no statistically significant difference in speech-related QOL between support group participants and nonparticipants, since 10 of 12 patients who had a total laryngectomy were participants of the support group. Additionally, patients in the support group tended to have had a longer mean time since cancer diagnosis than nonparticipants, possibly resulting in better adjustment to disease, its morbidity, and to a more positive outlook on the potential for long-term survival. Thus, the presence of more long-term cancer survivors may have contributed to the better HNQOL scores observed among support group participants. When comparing patients who had their cancer diagnosis for longer than 2 years with those who had their diagnosis for less than 2 years, there was improved emotion-related QOL and less bother by their cancer and its treatment in the former group. Although these and other factors could have affected the HNQOL scores seen among participants of this study, none of our subgroup analyses identified variables with as strong an impact on HNQOL scores as seen with participation in a support group.
Head and neck cancer and its treatment may negatively affect the QOL of patients, including difficulties with eating, speech, pain, and emotional distress. Thus, QOL issues should be important to the practitioner treating patients with head and neck cancer, and interventions that may positively influence QOL should be considered. The goal of the head and neck cancer support group was to provide patients with education, coping skills, and emotional support to help manage challenges brought about by their disease and its treatment. The better HNQOL scores observed among patients participating in the head and neck cancer support group may reflect the success in meeting its intended goal.
Limitations
Several limitations of this study include its post-test design, lack of prospective random assignment of patients, the diverse range of primary sites and clinical stages of the tumors, and variable treatments received by the subjects. Patients did not complete HNQOL surveys before their entry into the support group in this retrospective study. The lack of pre-test data makes it difficult to determine whether the differences in HNQOL scores between the two groups were due to the intervention of support group participation. Quite possibly, patients with higher perceived QOL self-selected into the intervention group. Given the lack of random assignment, we cannot exclude the possibility that the decision of some patients to choose to participate in the support group is a reflection of having better psychological coping mechanisms, which may have translated into better HNQOL scores for the participant group. Finally, our small sample size did not allow multivariate analysis of our data. Nonetheless, the results of this study do support the logical conclusion that patient participation in a head and neck cancer support group may contribute to improved QOL. In this regard, we believe that a support group is a useful adjunct in the treatment of patients with head and neck cancer.
Conclusions
The goals of the head and neck cancer support group were to provide patients with a supportive environment where one is given education, coping skills, and emotional support, as well as allowing discussion of concerns about their disease and its management. The better HNQOL scores observed among patients participating in this support group may reflect the success in meeting its intended goals. In this study, patient participation in a head and neck cancer support group was associated with improved QOL, implying that such support groups may serve as a useful adjunct to standard medical and surgical therapy for head and neck cancer. These findings suggest the need for future prospective, randomized studies, or, if random assignment is not practicable, a pre-test/post-test assessment of HNQOL scores to further examine the benefit that support groups may have for patients with head and neck cancer.