
Abstract
Objectives
Patients with laryngotracheal stenosis often require airway reconstruction. Following surgical intervention, voicing may be produced with either a glottic or supraglottic vibratory source. The objective of this study was to compare average airflow, estimated subglottal pressure, and expert perceptual rating of strain between children with glottic and supraglottic vibratory sources post-airway reconstruction.
Study Design
This study was a non-randomized prospective study conducted at the Cincinnati Children's Hospital Medical Center (CCHMC), Center for Pediatric Voice Disorders, and included 12 participants with a diagnosis of subglottic stenosis, post-laryngotracheal reconstruction.
Results
Expert perceptual ratings of strain were significantly higher for participants with supraglottic versus glottic voicing (P = 0.0001). Although the mean airflow measure was higher for participants with glottic phonation and mean pressure measure was higher for those with supraglottic voicing, these comparisons failed to reach significance.
Conclusions
Patients who exhibit supraglottic phonation patterns demonstrate greater strain during speech, as well as potential alterations to aerodynamic patterns.
Significance
The significant differences in perceived strain by vibratory source are noteworthy, as perceptual quality is always a patient's motivation to seek treatment.
Aerodynamic Assessment
Given the wide spectrum of voice disorders and altered laryngeal function presented by individuals following laryngotracheal reconstruction (LTR), systematic documentation of communication ability, laryngeal condition, voicing, and potential for voicing prereconstruction and postreconstruction surgery is essential. One method of evaluation that provides physiological information about laryngeal function is an aerodynamic assessment. Average airflow and pressure measures during voicing are of interest in children post LTR because they reflect laryngeal and vocal tract compression behaviors, as well as increased respiratory effort. Direct relationships are observed between high estimated subglottal pressure measures and increased respiratory effort needed for phonation. Significant changes in airflow rate are noted when there are pathological alterations to the laryngeal valving structures, such as vocal polyps, contact ulcers, vocal nodules, and vocal fold paralysis.9, 10 Although surgical reconstruction procedures intended to increase airway patency are highly effective, they often alter laryngeal valving function. Therefore, average airflow rate is an important voice assessment measure for quantifying changes following reconstructive surgical procedures intended to increase the size of the airway. Average airflow rates, along with estimated subglottal pressure measures, provide information regarding valving efficiency of the laryngeal system.
Perceptual Assessment Of Strain
Strain associated with voicing can be described as any excess amount of laryngeal and respiratory effort required to produce and sustain voice sufficient for communication. During a clinical assessment, perceptual ratings of voice, formal and informal, often note the amount of strain an individual appears to be using during voice production. Perceptually, patients with supraglottic phonation patterns appear to be using more effort and strain, but this has not been characterized in a systematic manner. The degree to which strain is related to alterations in laryngeal valving patterns for phonation is not known. Understanding the physiology of excessive effort during voice production, particularly in an altered airway, is paramount for comprehensive voice remediation.
This study was a nonrandomized prospective study conducted at the Cincinnati Children's Hospital Medical Center (CCHMC) Center for Pediatric Voice Disorders. It was designed to examine mean average airflow, estimated subglottal pressure, and perceptual rating of strain by site of vibration for voicing in children post-airway reconstruction.
Methods
Participants
The 12 participants (four males and eight females) examined in this study were seen for a voice evaluation at the CCHMC Center for Pediatric Voice Disorders. All participants (1) had a diagnosis of subglottic stenosis and were post LTR (Table 1); (2) were able to follow directions to complete all speaking tasks; (3) had appropriate facial size for adequate mask seal, which is essential for adequate airflow measures; (4) had no known velopharyngeal incompetence; and (5) had no perceived hypernasality, which invalidates measures of estimated subglottal pressure. Participants ranged in age from 5 years 7 months to 15 years 4 months (mean 9 years 8 months). This study was approved by the CCHMC Institutional Review Board. Signed informed consent to participate in the research investigation was obtained from all participants' parents/guardians.
Participants' data
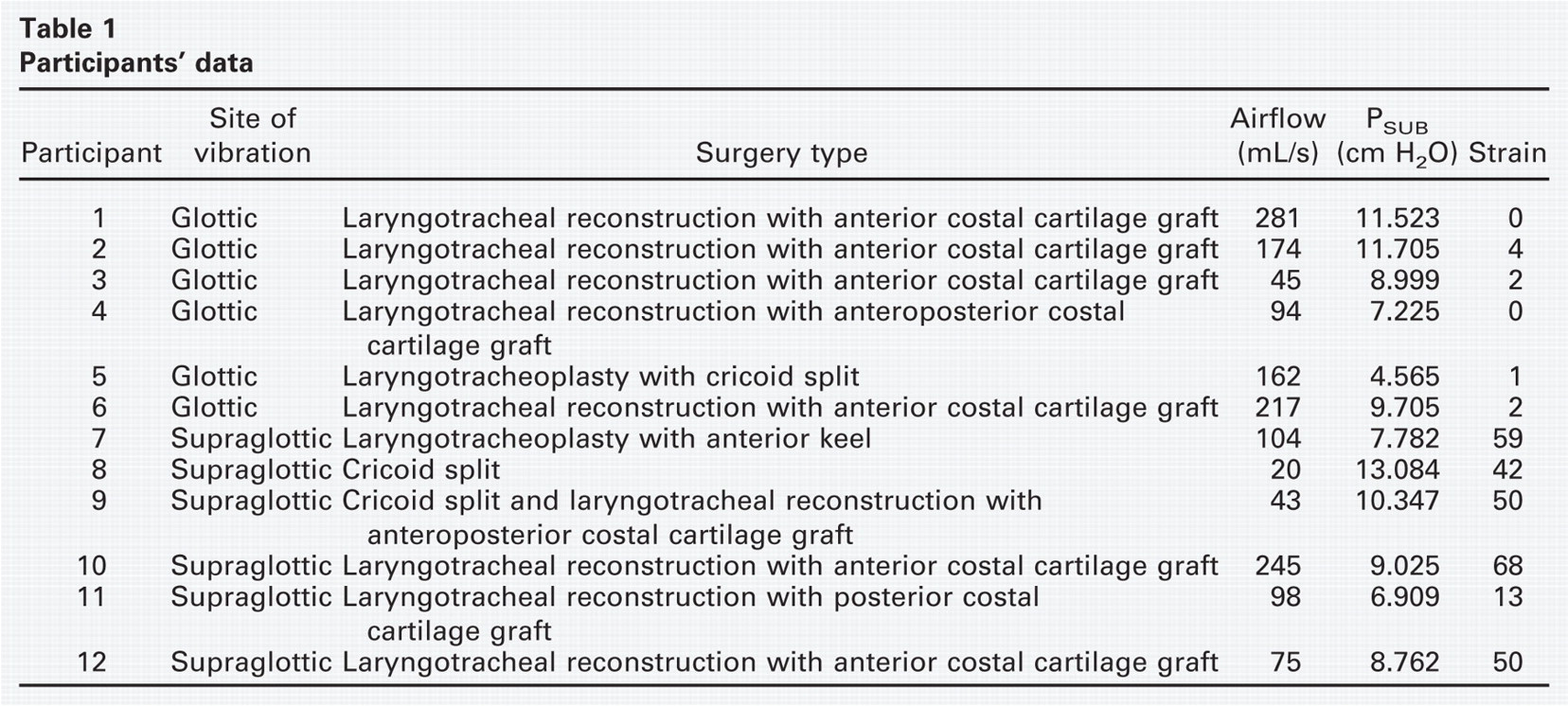
To determine the vibratory source of phonation, the CCHMC voice team professionals, with a minimum of 7 years of experience in analyzing laryngeal videoendoscopic examinations, reviewed video recordings of the participants' rigid or flexible endoscopic laryngeal examinations. All raters agreed that each participant's primary vibratory source for voicing was either glottic (vibration at the level of the vocal folds) or supraglottic (vibration above the level of the vocal folds). The 12 participants were grouped according to site of vibration (six glottic and six supraglottic).
The two groups were paired and matched by age and gender, with the exception of one pair aged 5 years. The mean age difference in the pairs was 8 months (SD, 5.10 months). Age-matched pairs did not cross boundaries with prepubescent versus pubescent laryngeal status.
Procedures
The tool used for the clinical auditory-perceptual assessment of strain was based on the Consensus Auditory-Perceptual Evaluation of Voice (CAPE-V).11 The strain subset was the only component of the CAPE-V used for this study. The participants' recorded production of six sentences, designed to elicit various laryngeal behaviors, was rated for strain by the use of a visual analog scale. A tic mark was placed on a 100-mm line (0 = least deviant, 100 = most severe). The results were reported in proportion to the total 100-mm length of the line (e.g., 60 of 100). Three of the CCHMC voice team speech-language pathologists (SLPs), with a minimum of 7 years of clinical voice experience, rated strain for each participant's digitally recorded speech samples using the same computer for all participants. All participant samples were rated in one listening session, and the three SLPs reached consensus for one value of strain for each participant's strain rating. One week later, the same three SLPs re-rated the participants' samples in a randomized order. The same computer, volume level, and time of day were adhered to for intrajudge reliability measures.
The aerodynamic measures of average airflow and estimated subglottal pressure were obtained from instrumentation that consisted of a circumferentially vented pneumotach facemask coupled to a narrow-band pressure transducer (PTL-1) and a separate wide-band pressure transducer (PTW-1) (model MS 100 A-2; Glottal Enterprises, Syracuse, NY). The airflow and pressure signals were routed to a Vetter Digital Multi-Channel Recording Adapter (model 4000A; Rebersburg, PA). The CSpeech 4.0 (Madison, WI)12 software program was used to extract the average airflow signal from the glottal airflow waveform. The airflow and pressure signals were recorded onto a digital audiotape. The instrumentation was calibrated for pressure at 5, 10, and 15 cm H2O and for a flow rate of 0.5 L/s and a volume of 2 L exchange (model MCU-4; Glottal Enterprises). The participants produced a sustained /a/ at comfort pitch with comfortable intensity for a minimum of 5 seconds. The participants also produced five syllable repetitions (syllable train) of /pa/ at comfort pitch with comfortable intensity. The series of repetitions were produced without interruption for breathing. Each /pa/ was approximately 1.5 seconds in length as prompted by one of the researchers. These tasks did not approach the participants' maximum phonation times, as determined in a pretest. The participants performed three satisfactory trials for each response task (sustained /a/ and /pa/ repetitions). Differences in frequency or intensity have a direct relationship to airflow and pressure values13, 14 and were monitored for the repeated measures (±4% of mean fundamental frequency and intensity values).
Results
Perceptual ratings of strain for participants with glottic-type vibration (group 1) ranged from 0 of 100 to 4 of 100 (mean, 1.5 of 100; SD, 1.52), whereas strain values for supraglottic-type vibration (group 2) ranged from 13 of 100 to 68 of 100 (mean, 47 of 100; SD, 18.89). A Pearson product-moment correlation coefficient was calculated for intrajudge reliability ratings of strain (r = 0.947), demonstrating a strong correlation. Independent-samples t-tests revealed that strain measures for participants with glottic versus supraglottic vibratory source were significant [t(10) = −5.881, P = 0.0001].
Average airflow measures for group 1 ranged from 45 mL/s to 281 mL/s (mean, 162 mL/s; SD, 84.43) compared with group 2 values, which ranged from 20 mL/s to 245 mL/s (mean, 98 mL/s; SD, 79.10). Independent-samples t-tests revealed that average airflow measures for the two groups of participants were not significant [t(10) = 1.369, P = 0.201]. Estimated subglottal pressure measures for group 1 ranged from 4.565 cm H2O to 11.705 cm H2O (mean, 8.954 cm H2O; SD, 2.72), while group 2 values ranged from 6.909 cm H2O to 13.084 cm H2O (mean, 9.318 cm H2O; SD, 2.18). Independent-samples t-tests revealed that estimated subglottal pressure measures for the two groups of participants were not significant [t(10) = −0.256, P = 0.803].
Discussion
The results of this study revealed that children post LTR, who used supraglottic structures for phonation, were rated by experienced voice clinicians as demonstrating significantly more strain during voice production. Assessment of strain, accomplished by consensus perceptual ratings, was supported with strong intrajudge reliability. It was concluded that these patients appeared to be using more effort to produce voice. This notion of effort would suggest hyperfunction of the laryngeal mechanism. The physiologic correlates of hyperfunctional voice can include, among others, decreased airflow rates and increased subglottic pressure.
Holmberg and colleagues15 found a significant increase in subglottal pressure in low and high pitch vowel productions compared with comfortable pitch productions for male and female speakers. Hillman and colleagues16 performed objective measures of voice production to describe physiological characteristics of disordered vocal fold vibration. Among their findings, these researchers noted that higher subglottal pressure was indicative of increased respiratory effort. Hillman et al9 and Sapienza and Stathopoulos10 noted higher airflow measures, without significant increase in pressure, for subjects with vocal fold pathologies (contact ulcers, nodules). Explanations for higher airflow included (1) decrease in vibrational amplitude of affected vocal fold, (2) decrease in stiffness of vocal fold cover, which interferes with normal vibratory pattern, and (3) glottal incompetence.
In this study, there were no significant findings between groups for airflow rates and estimated subglottal pressure. Closer examination of the data revealed a negligible higher estimated subglottal pressure in the supraglottic phonation group, although mean airflow was 40 percent lower for the supraglottic versus the glottic group. It is important to note that there was large variance, of comparable size, for airflow rates and estimated subglottal pressure within both groups of participants. However, the fact that average airflow was lower in the supraglottic group indicates that there may be a difference in valving characteristics in this population compared with the previously examined laryngeal pathologies.9, 10 It is possible that with a larger number of participants, the airflow and pressure differences between these groups could become more apparent. Our future research will include investigating larger numbers of participants, which may allow for further interpretation of airflow rates with supraglottic phonation patterns by surgery type. Additionally, average airflow rates, along with estimated subglottal pressure measures, provide information regarding valving efficiency of the laryngeal system and should be compared with perceptual ratings of laryngeal hyperfunction, clinically referred to as strain.
Recognizing the importance of the perceptual quality of the voice for the individual's sense of well-being, these significant differences in perceived strain by vibratory source are noteworthy. Hyperfunctional phonatory performance has the potential to adversely impact communication and social skills, as well as classroom performance. This could include classroom presentations and challenges being heard in classroom discussions. It could also potentially impact future occupation selection. Individuals can be restricted from careers that require talking on the telephone, particularly for extended periods of time, as well as jobs that require them to speak over noise. These results support the importance of therapeutic management regarding expected voice outcomes for children post LTR. When individuals require relatively high subglottal pressure to produce voice, improvement in perceptual quality of the voice following treatment may be indicated by a decrease in subglottal pressure or respiratory effort needed for phonation. The literature has not documented postsurgical intervention with this population. Therefore, the effectiveness and efficacy of specific treatment protocols to enhance the altered laryngeal voicing found in children post airway reconstruction cannot be described and remain areas for future research.
In conclusion, clinical evaluation results should provide valuable information to surgeons and SLPs regarding medical, surgical, and behavioral intervention timing and planning. Evaluation procedures need to be rigorous to ensure accurate measurements for assessing efficacious outcomes. Careful adaptation of evaluation protocols and a team approach including patient, caregivers, otolaryngologist, and SLP are essential to address all key assessment and subsequent management issues.