
Abstract
Objectives
In our department, we routinely use percutaneous dilation tracheotomy (PDT) in select intensive care unit (ICU) patients requiring prolonged intubation and mechanical ventilation. We present our experience with this technique and discuss the pros and cons of PDT in the intensive care setting.
Study Design and Setting
We conducted a retrospective study of consecutive PDTs performed in our institution between 2002 and 2004. Demographic information and procedural and postoperative complications were noted.
Results
Two hundred seventy-four PDTs were performed on intensive care unit patients during this time period. Complications included five cases of excessive intraoperative bleeding (1.8%), one postoperative hemorrhage (0.3%), one tracheoesophageal fistula (0.3%), one pneumothorax (0.3%), and four accidental decannulations (1.4%). No PDT-associated deaths occurred.
Conclusions
PDT is advantageous for the patient as it is performed at bedside in the ICU. It is our conclusion that this technique is suitable for many, but not all, critical care patients.
© 2007 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
Materials and Methods
A retrospective study of consecutive PDTs performed in the Department of Otolaryngology-Head and Neck Surgery, Johns Hopkins Medical Institution between 2002 and 2004.
The institutional review board reviewed and approved the protocol of this study. Age, sex, duration of intubation prior to surgery, and procedural complications were noted. The patients underwent PDT using the Ciaglia method Cook Blue Rhino single dilator PDT set (Cook Critical Care, Bloomington, IN). The surgery was performed at bedside in the various intensive care and step-down units (medical and surgical). All patients were intubated at the time of surgery. In all cases, the PDT was performed in patients managed by an anesthesiologist providing both general anesthesia and direct visualization of the tracheal lumen using a flexible bronchoscope. For the majority of patients, anesthesia consisted of intravenous lidocaine, midazolam, fentanyl, propofol, and mivacurium for brief paralysis. All patients were placed on 100 percent oxygen via fixed-rate ventilation throughout the procedure.
Ventilatory rate was increased to accommodate for the diminishment of tidal volume that occurs with use of the bronchoscope during the percutaneous tracheostomy. All patients were afforded standard monitoring of continuous or every 1- to 2-minute blood pressure as well as continuous heart rate, ECG, and oxygen saturation. Prior to incision, direct laryngoscopy was performed to withdraw the endotracheal tube under direct vision and manually fixed to a depth whereby the endotracheal tube cuff was midway between the vocal cords. In this manner, minimal, if any, manipulation of the endotracheal tube was necessary thereafter in order to align the tip within the tracheal lumen just proximal to the surgical puncture site. In rare instances of oxygen desaturation below 90 to 92 percent, the bronchoscope would be intermittently placed to the tip of the endotracheal tube rather than continuously used in order to maintain excellent visualization during the most pertinent surgical periods.
Local anesthesia and vasoconstriction of the surgical area were attained using two percent lidocaine with 1:100,000 epinephrine. A vertical skin incision is made between the cricoid cartilage and suprasternal notch. Subcutaneous tissue is bluntly dissected from cricoid caudad using a Crile forceps. The surgeon's index finger is then used to bluntly dissect pretracheal tissue and the upper edge of the thyroid isthmus caudally. At this time, the overhead lights are lowered and transillumination of the bronchosope light should readily be seen in the field. Tracheal puncture is performed with a large-bore needle, and a guidewire is inserted through it into the trachea. A series of dilators and then the tracheostomy tube are then introduced into the trachea over the guidewire. The tracheotomy is optimally performed at the level of the second to third tracheal ring assessed by palpation through the skin and subcutaneous tissue using the cricoid cartilage and the transillumination of the bronchoscope as anatomic reference points.
Results
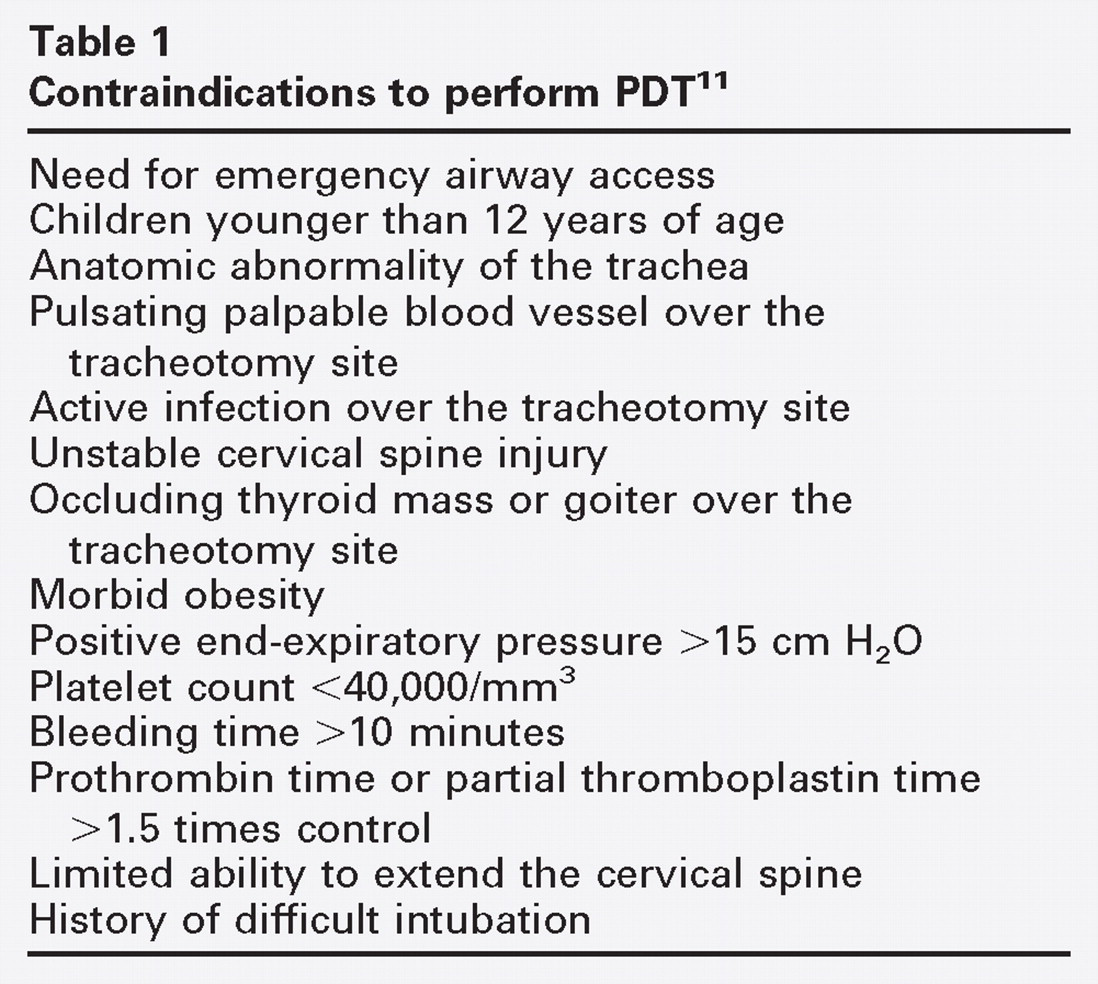
Two hundred seventy-four PDTs were performed in this time period. The indication for tracheotomy was prolonged mechanical ventilation in 257 (93%) of the cases. Other indications included airway protection (six cases), pulmonary toilet (eight cases), partial airway obstruction (two cases), and risk of aspiration in one case. Patients in whom PDT was contraindicated (Table 1) were excluded from the study and underwent an open surgical tracheotomy (OT). In this series of ICU patients, this primarily included obese patients and those with severe coagulopathies or a prior tracheotomy.
There were 148 men and 126 women in this group, with an age range of 19-100 years. Duration of intubation prior to PDT ranged from one to 45 days. PDT complications in our series included five cases of excessive intraoperative bleeding (1.8%), one postoperative hemorrhage (0.3%), one tracheoesophageal fistula (0.3%), one pneumothorax (0.3%), and four accidental decannulations (1.4%). No PDT-associated deaths occurred.
Discussion
Tracheotomy is one of the most frequently performed surgical procedures in the critically ill patient 8 and indeed most tracheotomies are performed on ICU patients. 9 , 10 It is generally held that tracheotomy provides the benefits of greater patient comfort, greater airway security, and better pulmonary toilet in comparison with endotracheal intubation, while reducing the risk of subglottic stenosis.
Although PDT has been used for quite some time, there remains considerable resistance to its acceptance among otolaryngologists. This may be due to initial reports of high complication rates and the fact the surgical airway is attained in a relatively “blind” fashion.
In fact, complication rates of tracheotomy, both traditional OT and PDT, vary greatly from study to study. OT holds an overall complication rate of five to 40 percent depending on study design, patient follow-up, and the definition of the different complications. The mortality rate of tracheotomy is less than two percent. 11 In a recent study of 1132 OTs, the major complication rate was as low as 4.3 percent with a mortality rate of 0.7 percent. 12
The complication rate of PDT varies greatly for various PDT techniques. In one study, the Rapitrac technique showed a significantly higher number of complications compared with the Seldinger technique. 13 Several studies have tried to assess which method is best, with no clear advantage demonstrated between methods. Anon et al 14 recently published a prospective randomized trial comparing the Griggs guidewire forceps and Ciaglia Blue Rhino methods. They randomly assigned 53 patients to one of these two methods and found seven complications in the Griggs method and two in the Ciaglia method. No statistically significant difference was found; however, the study population was small.
In one of the largest series of PDT in the ICU setting using the Ciaglia Blue Rhino single dilator technique, the total complication rate was 6.5 percent in 309 patients. More than half of these complications were considered minor by the authors. The two most common complications in their series were oxygen desaturation and and bleeding. 15 In another recent series of 178 PDTs, Liao et al 16 reported an overall complication rate of 5.1 percent. Their series inludes PDTs performed using multiple dilators prior to May 2001. The Cook Blue Rhino single dilator system was introduced and used for the remainder of their series. All complications in their PDT group occurred before using a single dilator system. However, whether their initial complications from PDT were caused by inexperienced operators, poor patient selection, or technical issues with the instrumentation is difficult to elucidate in this retrospective study.
In our series, there was an overall complication rate of 4.3 percent, with bleeding being the most common complication (2.1%), comprising 50 percent of the complications. Five cases of excessive intraoperative bleeding (1.8%), one postoperative hemorrhage (0.3%), 1 tracheoesophageal fistula (0.3%), one pneumothorax (0.3%), and four accidental decannulations (1.4%) also occurred.
The most common complication, bleeding, is thought to be due to operator error. The sole tracheoesophageal fistula also may be blamed on operator error, that is, inserting the guiding needle too deeply and accidentally penetrating the posterior tracheal wall. These errors decrease with operator experience.
Four accidental decannulations occurred in our series and may be avoided by securing the tracheotomy tube to the neck with both ties and sutures and instructing the nursing and respiratory therapy staff not to remove the tracheotomy tube before tract maturation and only under supervision of the surgeon.
Another issue under debate is the need for simultaneous fiberoptic bronchoscopy during the PDT. Bronchoscopy as an adjunct to percutaneous tracheostomy was not described until 1989. 17 van Heerbeek et al 18 also recommended the PDT be performed under constant fiberoptic broncoscopic control in order to “increase the safety of the procedure.” On the other hand, Reilly et al 19 , 20 concluded that continuous bronchoscopy during PDF contributes significantly to early hypoventilation, hypercarbia, and respiratory acidosis during the procedure.
Therefore, it may be that bronchoscopy is not necessary and that its use contributes to increased cost and delay. However, in our opinion it does increase the procedural accuracy and safety. For this reason, we used bronchoscopic guidance during the procedure in all cases in this study.
Kost, 15 in his large series, states that “the absence of serious complications such as pneumothorax and pneumo-mediastinum are attributable to the use of bronchoscopy.” In our series, we had one case of pneumothorax despite the use of videobronchoscopy in all of our cases.
The technique of PDT is not difficult to learn, but it has been repeatedly reported that a learning curve exists that may be overcome by performing a number of supervised procedures. 20 , 21 In one study, Pelausa 22 found PDT easily learned and considerably faster to perform than OT. In his results, Pelausa encountered several unexpected difficulties. The kit was applicable only to lean patients with supple necks and prominent cervical landmarks. The penetrator was too short for some patients.
In one case, a traditional OT was required to stem the bleeding. We found no such diffuculties with the Blue Rhino kit that we used. The procedure was easy to learn, to perform, and to teach. However, the PDTs in this study were performed by the same three experienced surgeons, and therefore a dedicated study as to the PDT learning curve is warranted.
It should be emphasized that much of the morbidity and mortality associated with tracheotomy, regardless of the method used, are inherent to the underlying critical state of the patient. 23 In that regard, bedside PDT precludes the necessity to transport critically ill patients requiring intensive monitoring to and from the operating room. In a prospective study of 125 critically ill patients who were transported from the ICU, about one third experienced at least one mishap, from cardiac lead failure to vasoactive drug disconnection. 24 , 25 We also found the bedside procedure extremely beneficial to the patients and the medical staff who were otherwise required to transfer an often hemodynamically unstable patient to the operating room for OT.
In our institution, the PDT is arranged directly between the intensive care team and the surgeon, with no need for administrative, nursing, or operating room intervention. The intensive care physician flagged patients who required tracheotomy, the otolaryngologist was called to assess the patient as a surgical candidate, and the PDT was performed. This protocol led to the formation of a highly efficient “tracheotomy team.”
With wider acceptance of bedside PDT in the ICU and the relative technical simplicity of the technique, more non-surgeons are performing it. In particular, many critical care personnel have embraced this minimally invasive procedure and are performing bedside PDT. However rare, catastrophic complications may occur, and the operator should be an able surgeon who can obtain a surgical airway if the PDT or reintubation fails and be capable of surgically stemming massive hemorrhage in its unlikely event.
Part of the confidence in performing PDT is in the knowledge that immediate reintubation or emergency OT is feasible if necessary.
Conclusion
PDT provides a convenient alternative to OT and should be added to the otolaryngologist's armamentarium of surgical airway procedures. The procedure is advantageous for the patient as it is performed at bedside. Complication rates are low and similar to those cited in the literature for OT. It is our conclusion that this technique is suitable for many, but not all, critical care patients.