
Abstract
Yet, the most appropriate standard of care for treating vocal fold polyps and cysts has not been established. Although hyperfunctional behavior increases the stress at the midmembranous vocal folds and leads to pathologic changes within the superficial layer of the lamina propria, producing nodules, polyps, or cysts, the utility of voice therapy to decrease such behaviors in polyps and cysts is not known. 3 Voice therapy is effective at minimizing detrimental vocal behaviors that result in voice improvement, however, earlier studies have primarily focused on nonorganic voice disorders, muscle tension dysphonia (MTD), and nodules. 4–7 In contrast, different treatment has been recommended for polyps and cysts that consists of a combination of phonomicrosurgery and voice therapy. 8–11 How often surgery is required, which patients are likely to respond to voice therapy, and who needs surgery is not known.
As a result, no consensus exists with respect to recommending voice therapy for polyps and cysts. A recent survey of members of the American Academy of Otolaryngology–Head and Neck Surgery found that 91% of respondents use voice therapy as first line treatment in nodules, but respondents were divided about the use of voice therapy in polyps and cysts. 12 If voice therapy were effective in the treatment of polyps and cysts, the need for surgery and its inherent risks would be reduced. Conversely, if voice therapy did not improve dysphonia, patients could be directed to operative intervention without prolonged delays while waiting to see if voice therapy helped. To clarify this dilemma, this study will test the hypothesis that voice therapy is effective in treating vocal fold polyps and cysts.
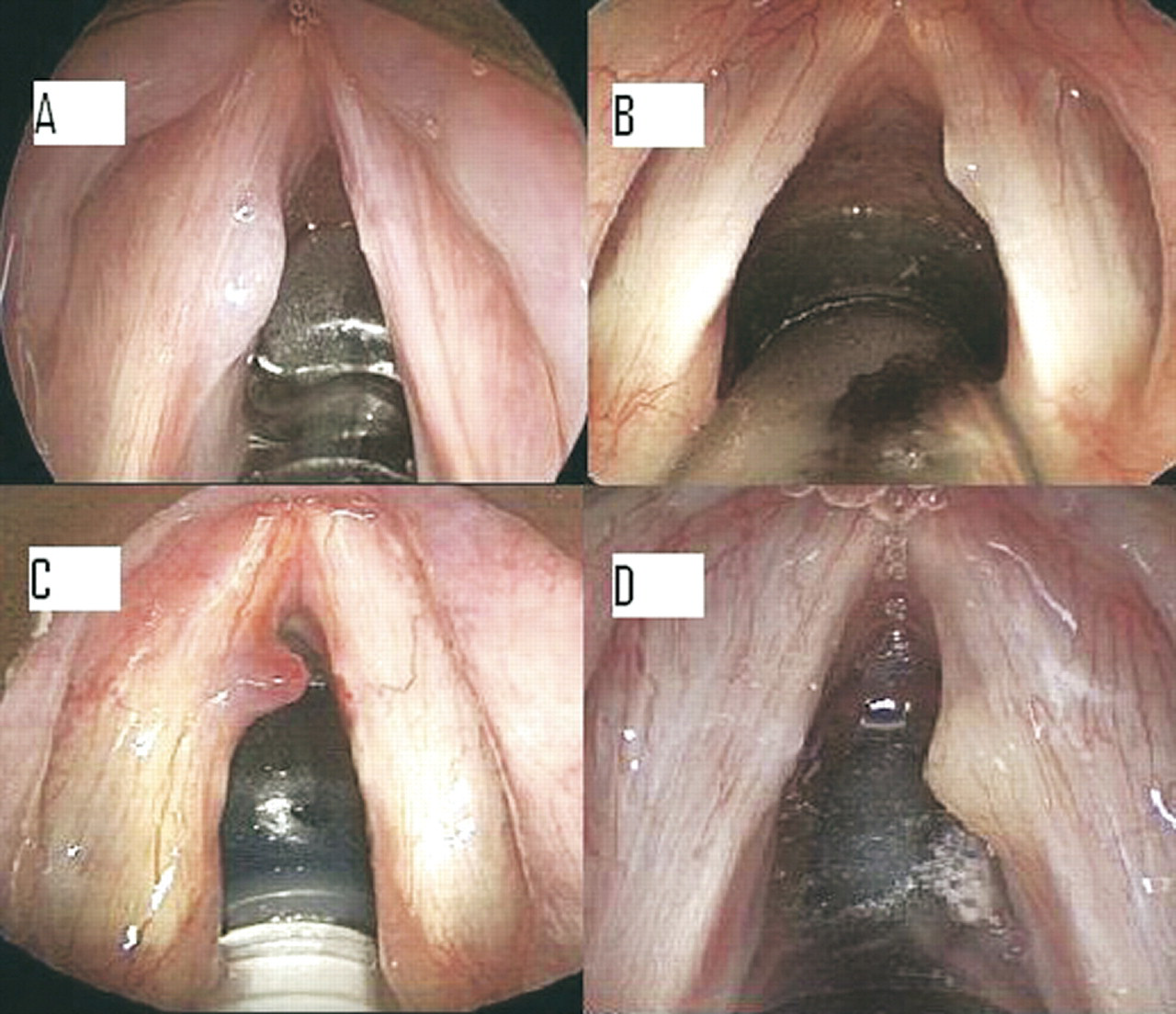
Example of hyaline, fibrotic polyp (
METHODS
The Vanderbilt Institutional Review Board approved the study. A medical records search from January 2002 to September 2005 for the ICD-9 codes for vocal fold nodules (478.4) and vocal fold polyps (478.5) was performed. Patients with a diagnosis of a vocal fold cyst or vocal fold polyp who had a trial of at least 2 sessions of speaking and/or singing voice therapy were included. Patients without a trial of voice therapy, no follow-up after initial evaluation, or with vocal fold nodules, Reinkes edema, leukoplakia, or granulomas were excluded. Voice therapy was determined by the individual therapists but included the same general approach of managing vocal hygiene, breath support, laryngeal tension, and pitch. All patients were treated by masters or PhD level speech pathologists and/or singing voice specialists at a single institution. Medical management of allergic rhinitis and gastroesophageal reflux (GER) was also performed. Videostroboscopies were reviewed by a laryngologist and masters or PhD level speech pathologist to confirm diagnosis. Demographic information, diagnosis, MTD, allergy and GER treatment, singing status, length of hoarseness, follow-up, and videostroboscopy parameters were collected. Voice improvement was the main outcome measure and was defined as the patient, at last follow-up, stating that his/her voice improved sufficiently to meet his/her daily voice needs most of the time.
Definitions of vocal fold polyps and cysts were determined a priori. Polyps were typically unilateral masses of the free vocal fold margin at the junction of the anterior and middle third with mucosal wave present. Unilateral submucosal masses at the junction of the anterior and middle third of the vocal fold with reduced or absent wave were classified as cysts. 13 Patients could have contralateral reactive lesions or bilateral polyps and still be included. Based on videostroboscopy, polyps were further classified as translucent (polyp filled with edematous-appearing fluid), hemorrhagic (polyp with vascular changes), or fibrotic, hyaline (polyp filled with thick, myxoid-appearing fluid) (Fig 1). Patients with anterior-posterior glottic and/or supraglottic constriction during phonation denoted MTD. In addition, patients may have also had tenderness to palpation of the submental region, thyrohyoid space, hyoid bone, thyroid cartilage, or strap muscles. Patient report of heartburn or regurgitation indicated GER. Smoking was divided into current smokers or never smokers. Two patients who quit smoking 2 months before presenting to the voice center were classified as current smokers. Mucosal wave was classified as either normal, decreased, or absent and vocal fold closure as complete or incomplete.
Statistical analysis was performed with SigmaStat 2.03 (SPSS Inc, Chicago, IL). χ 2 statistics or the Fisher exact test was performed to assess associations between categorical data and the main outcome measure. The rank sum test analyzed the relationship between continuous variables and the main outcome measure. Multivariate analysis was performed with multiple logistic regression.
Factors associated with voice improvement after voice therapy in patients with vocal fold polyps and cysts
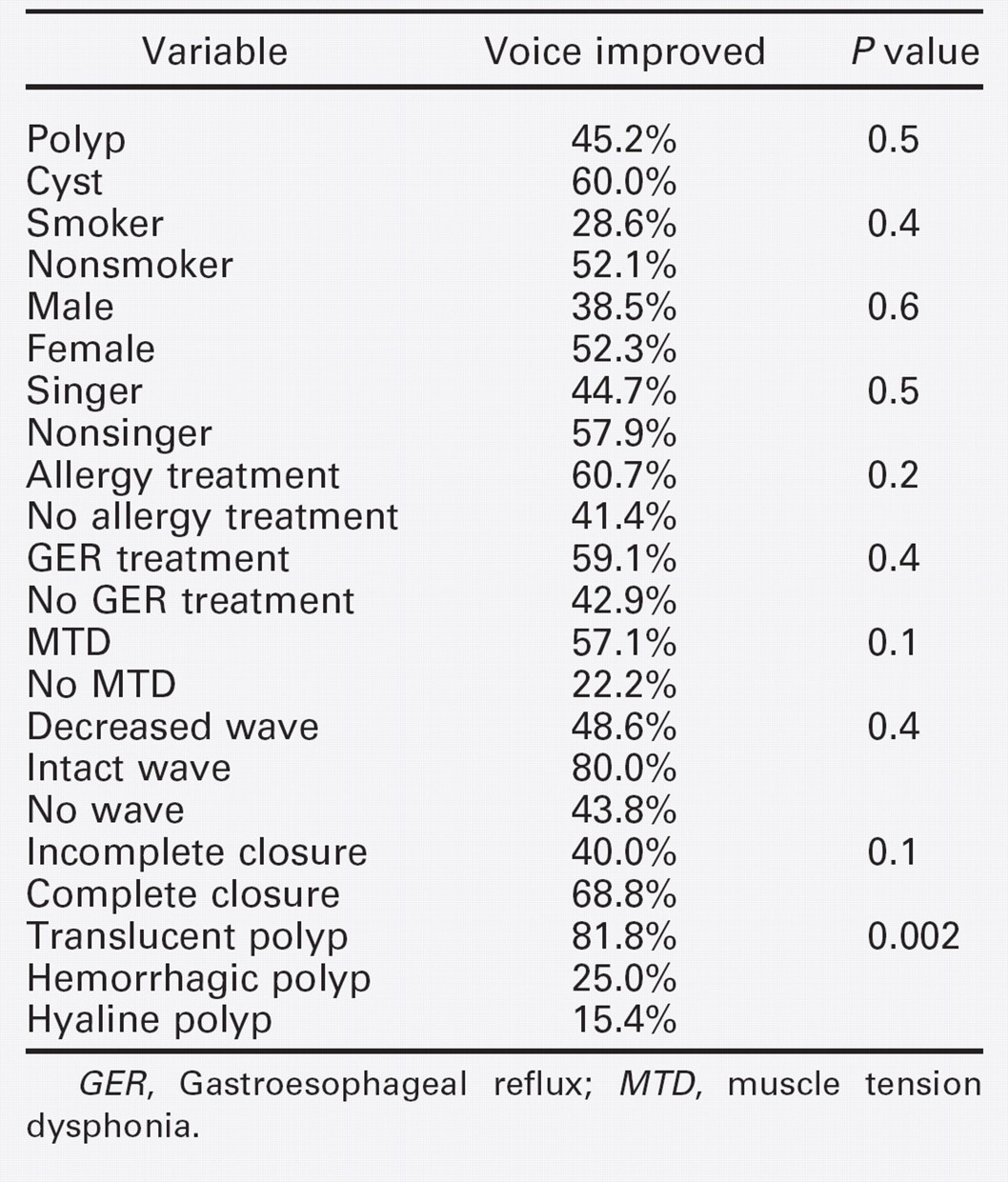
GER, Gastroesophageal reflux; MTD, muscle tension dysphonia.
RESULTS
Of 435 patients with the ICD-9 codes 478.4 or 478.5, 57 patients who met the inclusion criteria were identified. Among those excluded, 23 patients with a polyp or cyst either had no follow-up or no voice therapy trial due to patient preference for initial surgery. The mean age was 36.0 years with a range of 15 to 72 years with 22.8% male and 77.2% female. Patients had hoarseness for a mean 14.5 months and a range of 1 to 60 months. Cysts were diagnosed in 26.3% of patients and polyps in 73.7%.
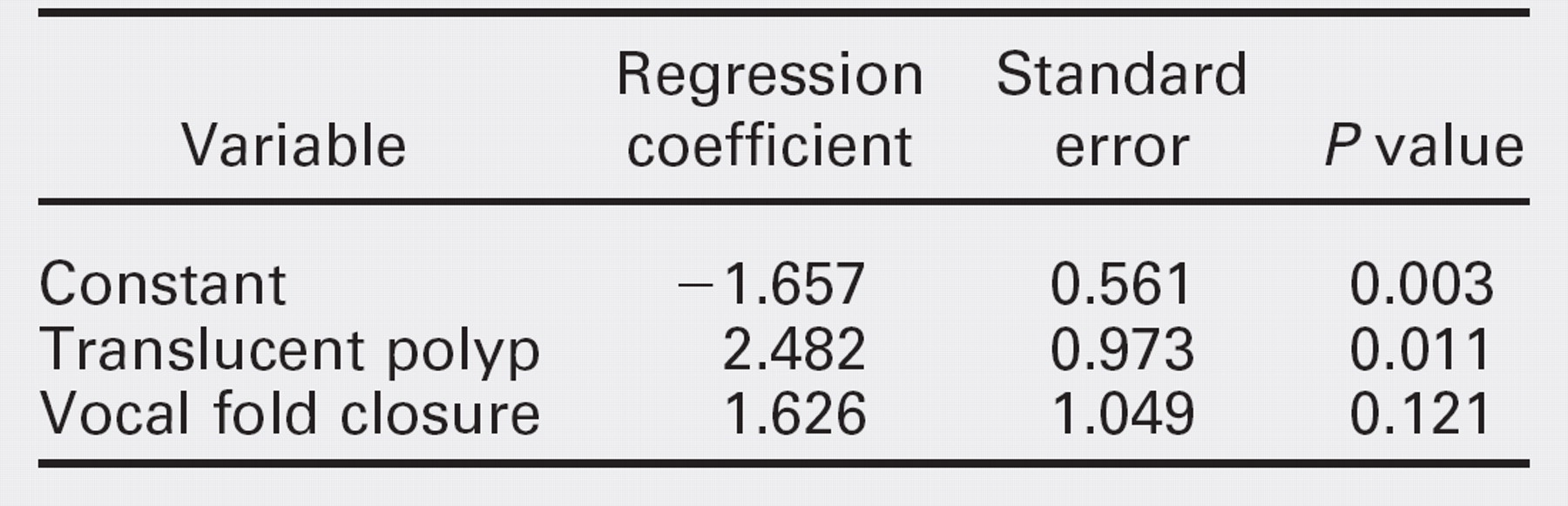
Voice improvement with voice therapy was achieved in 49.1% of patients, regardless of diagnosis (Table 1). Four lesions (one cyst and three polyps) completely resolved. Surgery was required in 50.1% of cases. Patients were followed for a mean 7.9 months with a range of 2 to 36 months. Among polyp patients, those with translucent polyps were more likely to have an improved voice after therapy compared with those with fibrotic, hyaline, or hemorrhagic polyps (Table 1, P = 0.002, χ 2 ). No statistically significant associations between MTD (P = 0.1, Fisher exact test) and for complete vocal fold closure (P = 0.1, χ 2 ) and voice improvement were identified. Patients with translucent polyps were more likely to achieve complete vocal fold closure than those with fibrotic, hyaline, or hemorrhagic polyps (54.5% vs 7.7% and 16.7%, respectively, P = 0.02, χ 2 ). After controlling for vocal fold closure, patients with translucent polyps were more likely to have an improved voice after voice therapy than those with fibrotic, hyaline, or hemorrhagic polyps (P = 0.01, multiple logistic regression, Table 2). The length of patients’ hoarseness was not associated with voice improvement (P = 0.9, rank sum test). Sex, smoking status, allergy treatment, singing status, mucosal wave, and GER treatment were not statistically significantly related to whether the voice improved after voice therapy (Table 1).
DISCUSSION
Although voice therapy has been traditionally used for vocal fold nodules, phonomicrosurgical techniques have been developed for treating vocal fold cysts and polyps. 9–11 How hoarseness related to vocal fold polyps and cysts responds to voice therapy alone and which patients with polyps and cysts require surgery remains unknown. This preliminary study was undertaken to determine how often voice therapy results in hoarseness resolution in patients with polyps and cysts and to identify patients likely to respond.
Our study found that voice therapy was effective in improving patients’ voices. Almost half of our patients with vocal fold polyps and cysts had an improved voice at their last follow-up. Our study found no association between length of hoarseness and treatment response. 14 Furthermore, smoking status, allergy and GER treatment, mucosal wave, and singing status were not associated with treatment outcome. Although a higher percentage of nonsmokers, nonsingers, and patients receiving allergy and GER treatment had voice improvement, there were no statistically significantly associations between these variables and treatment outcome (Table 1). Larger patient numbers and a more objective outcome measure are required to elucidate the impact these variables have on voice therapy outcomes for polyps and cysts.
Certain groups of patients may be more likely to respond to voice therapy. Although no differences were seen between polyps and cysts, the type of polyp was associated with voice improvement. Specifically, patients with translucent polyps were more likely to experience an improved voice than those with fibrotic, hyaline, or hemorrhagic polyps (Table 1, P = 0.002, χ 2 ). An earlier histologic study classified pathologic changes in the lamina propria into five stages that range from edematous (least mature stage) to angiomatous (intermediate stage) to hyaline (most mature stage). 14 Compared with mature hemorrhagic and fibrotic hyaline polyps, translucent polyps may be more immature and more likely to respond to voice therapy. Because the videostroboscopies are not standardized with respect to telescope angle and magnification, direct comparison of change in size across each polyp type could not be performed. Because not every polyp was resected, histologic specimens were not always available, which prevented direct correlation of histology and outcome in our study. Future studies with new technology, such as optical coherence tomography, may be able to assess the microstructure of vocal fold lesions in clinic and provide important prognostic information.
Multiple logistic regression between vocal fold closure, translucent polyp, and voice improvement
Furthermore, lesion disappearance does not appear essential for voice improvement. Holmberg et al 6 found that although most nodules decreased in size after voice therapy, nodules persisted in all patients despite improvement. Similarly, only four of our lesions (three polyps and one cyst), resolved completely. Because reduction of abnormal vocal behaviors is an important component of treatment, a trial of voice therapy, regardless of lesion type, has been recommended. 13 Findings of MTD, such as constriction at the glottic or supraglottic level and tenderness in the circumlaryngeal region, may serve as markers for patients with more severe abnormal vocal behaviors. Reduction of trauma at the midmembranous vocal fold can allow some resolution of the lesion and the inflammation associated with it. Furthermore, with the use of the voice in a more efficient manner, a patient's voice may improve despite the persistence of the polyp or cyst. In addition, the ability to obtain complete vocal fold closure may be important. With glottal incompetence, patients would have air escape during phonation or singing. Consequently, voice therapy may not be able to overcome the limitation of incomplete glottal closure. In contrast, patients with complete glottal closure might be able to use their voice more efficiently as a result of voice therapy. Hence, despite the persistence of the polyp or cyst, patients could realize improved voice.
Certain methodological issues must be addressed. Because the technique of voice therapy depended on the individual therapist, no comments can be made about the relative benefit of specific techniques. Misclassification bias may have occurred because all patients did not have the diagnosis confirmed in the operating room. Patients that appeared to have translucent polyps on videostroboscopy may have been more fibrotic or hyaline in nature. Nonetheless, the decision to proceed with surgery or voice therapy is based on clinical assessment that includes videostroboscopy. Verdolini et al 15 found that patient practice and adherence to voice therapy recommendations influenced outcomes. Because our study was retrospective, no data on patient adherence could be obtained. In addition, 23 patients were excluded because of no follow-up or no voice therapy trial. Because their outcome would alter the percentage of patients who had an improved voice, our finding of almost 50% response rate may be an overestimate. However, if all 23 had failed voice therapy, our response rate would have still been substantial at 35%.
Although classifying a patient as having an improved voice was based on the last follow-up, patients could have had a recurrence. In fact, follow-up ranged from 2 to 36 months. Those with short follow-up may have had initial, although transient, improvement. Whether and for how long patients maintain their improved voice is unknown and worthy of future investigation. The definition of voice improvement, based on patient report as documented in the patient chart, is a limitation. On the other hand, objective voice measures, such as jitter and shimmer, do not measure the impact of voice problems on patients’ level of function and suffer from variability, limiting the ability to detect treatment changes. 16,17 Voice handicap or voice-related quality-of-life instruments would provide quantitative measures of patients’ perceptions of their voice problems and response to voice therapy. Because this is a preliminary study, subsequent prospective investigation with validated, voice-related health instruments is important to substantiate these early findings.
CONCLUSION
Voice therapy as a first-line treatment is effective in improving hoarseness in patients with vocal fold polyps and cysts. Patients with translucent polyps, objective findings of MTD, and complete vocal fold closure on videostroboscopy may be more likely to positively respond to voice therapy. These features may serve as a guide for laryngologists and allow them to more efficiently direct patients unlikely to benefit from voice therapy to surgical treatment and to recommend those likely to respond to a more in-depth voice therapy protocol. Future investigations should confirm these preliminary findings in a prospective manner with validated, voice-related quality-of-life outcome measures.