
Abstract

A 38-year-old man presented with vague throat pain of five months' duration. He had similar complaints about two years back, associated with sour taste in the mouth. There was no history of fever, loss of weight, restriction of neck movements, impaction of foreign body, or recent instrumentation of the throat. On examination, he was found to have a cystic swelling in the posterior pharyngeal wall on the right side that extended from the level of soft palate down to the level of epiglottis. Aspiration of the cyst was performed, and the aspirate was reported to contain only inflammatory cells, rich in foamy macrophages. He defaulted in follow-up examinations because the cyst had shrunken in size after the aspiration and symptoms had disappeared.
About 11 months later, he developed the same symptoms and presented himself at the outpatient clinic. Examination revealed a smooth cystic bulge on the right posterior pharyngeal wall that extended from the level of soft palate up to the level of epiglottis.
Horizontally, it extended from the right posterior pillar to the midline. There was no laryngeal involvement or extension to the neck.
A lateral view radiograph of the neck showed retropharyngeal widening with a smooth bulge at the level of C3-C5 vertebrae. Computed tomography of the region (Fig 1) showed a well-defined nonenhancing 4 × 4 × 1.5 cm cystic lesion posterior to oropharynx, more to the right side. The nasopharynx, epiglottis, pre-epiglottic space, hypopharynx, larynx, laryngeal cartilages, neck vessels, and bones appeared normal.
Excision of the cyst was done, with the patient under general anesthesia. A linear mucosal incision was made over the swelling. The cyst was found to lie submucosally, superficial to the paraspinal muscles, without any infiltration to the surrounding tissues. It was separated from the surrounding structures by blunt dissection and was excised fully. The defect in the mucosa over the posterior pharyngeal wall was approximated.
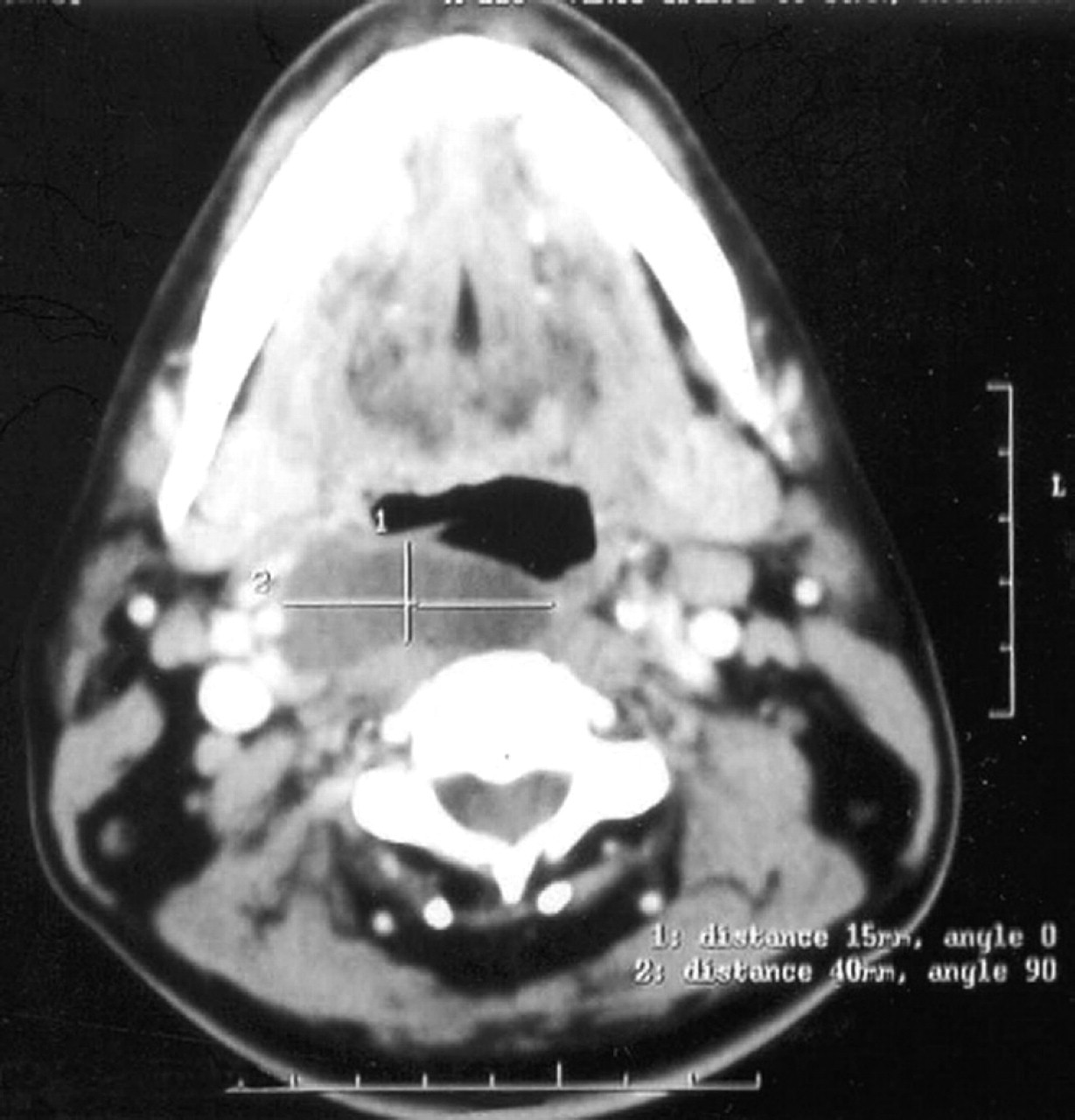
Computed tomogram of the neck shows the retropharyngeal bronchogenic cyst.
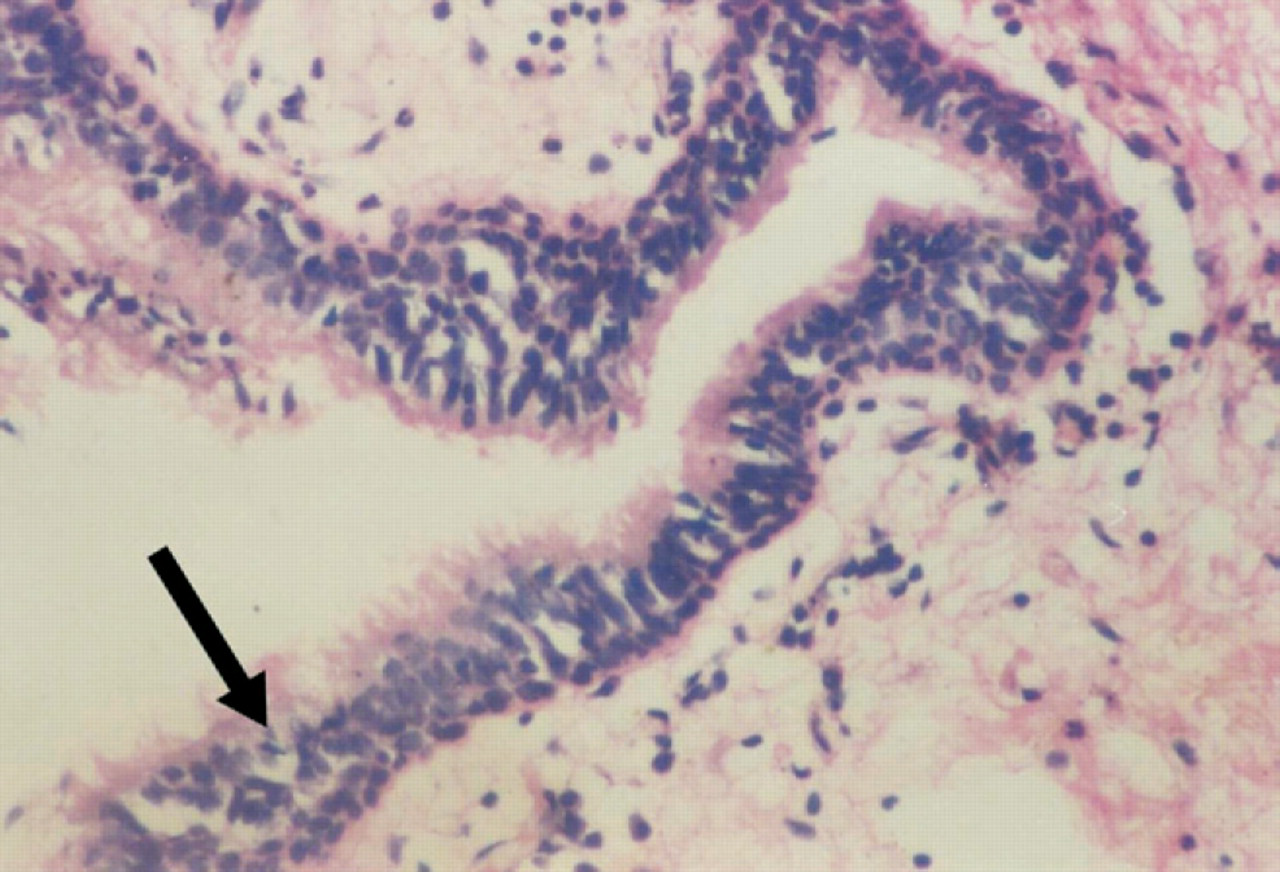
Histology of the bronchogenic cyst. Arrow shows the pseudostratified ciliated columnar epithelium. (Hematoxylin and eosin stain; original magnification X400.)
Histopathologic examination revealed that the cyst wall consisted of pseudostratified ciliated columnar epithelium surrounded by fibrocartilaginous elements, scattered blood vessels, and inflammatory cells (Fig 2), suggestive of a bronchogenic cyst.
Discussion
Bronchogenic cysts are lesions of congenital origin derived from the primitive ventral foregut. 1 – 4 They are the most common primary cysts of the mediastinum. 2 They are thought to develop by around the fourth to the eighth week of gestation and may be mediastinal, intrapulmonary, or, less frequently, in the head and neck area, and subdiaphragmatic region. 1 – 3 They belong to the broad category of bronchopulmonary foregut malformations, the anomalies of pulmonary development that are due to abnormal budding of the embryonic foregut and tracheobronchial tree and that includes foregut cysts, bronchogenic cysts, enteric cysts, and neuroenteric cysts. 3
The frequency of bronchogenic cysts is unknown presumably because many patients are asymptomatic. Although some bronchogenic cysts are asymptomatic and are incidental findings on radiography, most cysts become symptomatic later and complications are more common in symptomatic patients. Most bronchogenic cysts in children are found incidentally when imaging is performed for other reasons.
Two thirds of the patients with intrathoracic bronchogenic cysts develop symptoms 3 that are most frequently caused by the compression of trachea or bronchi, which leads to cough, wheezing, stridor, dyspnea, cyanotic spells, and pneumonia, or by complications related to the cysts. 2 , 3 Usual complications are intracystic hemorrhage, infection of the cyst, squamous metaplasia, rupture or perforation of the cyst to tracheobronchial tree, pericardium or pleura, and rarely 4 malignancy.
When bronchogenic cysts occur in other locations, symptoms may be related to their size, compression of the neighboring structures and cyst infection. In the neck, they may present with swelling, symptoms of upper respiratory obstruction, and pain. 1 Even though rare cases that occur in the tongue have been reported earlier, retropharyngeal location of bronchogenic cysts has not been reported.
Most often bronchogenic cysts are unilocular rather than multilocular, although they may contain internal trabeculations. The cysts are characterized by a lining of ciliated cuboidal or pseudostratified columnar epithelium 3 and may or may not be surrounded by cartilage, elastic tissue, smooth muscles, and seromucinous glands in their walls, and are often filled with mucoid material. Chest radiography, computed tomography, MRI, and endoscopic ultrasonography can aid the preoperative diagnosis of intrathoracic bronchogenic cysts; complete excision of the cyst is the treatment of choice.
Retropharyngeal lesions commonly occur due to acute infections (abscesses as a result of lymph node suppuration or those after injuries) or chronic infections (tuberculous caries of cervical spine). 5 Less common causes include neoplasms like neuroblastoma, teratoma, and ectopic thyroid. Rare causes are lymph node enlargement due to Langerhan's cell histiocytosis and Kawasaki's disease, synovial cyst (ganglion) of anterior longitudinal ligament of cervical spine, aberrant thymic tissue, angioneurotic edema, and congenital myxoedema. To the best of our knowledge, no case of bronchogenic cyst in the retropharyngeal space has been reported in the English-language medical literature. Thus, henceforth bronchogenic cysts also should be considered in the differential diagnosis of cystic retropharyngeal mass lesions.