
Abstract

The clinical presentation of infected branchial cleft cysts may vary in relationship to the offending organism. Only 1 case of Brucella melitensis infection in a branchial cleft cyst has been reported in the literature, and the patient's clinical picture was suggestive of brucellosis. 1 We are reporting the first case of an isolated branchial cleft cyst infection with Brucella melitensis with no associated symptoms or signs of systemic brucellosis.
A 23-year-old woman presented to the American University of Beirut Medical Center with a 1-month history of multiple anterior and posterior cervical masses. Over the next 3 weeks, these masses regressed spontaneously except for a right anterolateral neck mass that kept increasing in size. There was no history of fever, pain, hoarseness, dysphagia, dyspnea, or joint problems. Her medical history was negative for systemic symptoms, recent upper respiratory tract infections, or prior neck masses. The patient also denied any exposure to pets, cattle, or unpasteurized dairy products. A fine needle aspiration done in an outside clinic 1 week before her presentation revealed 15 mL of thick purulent contents. Unfortunately, the aspirated material was not sent for Gram stain or culture.
On physical examination, there was a 6 × 4 cm right neck mass located at level II-III of the anterior jugular chain (Fig 1). The mass was soft, mobile, nontender, nonpulsating, and had no overlying skin changes. The patient had no lymphadenopathy or hepatosplenomegaly. A complete blood count and full chemistry panel results were normal. Computed tomography with intravenous contrast revealed a 5.5 × 4 × 3 cm cystic lesion, lateral to the major vessels, displacing the submandibular gland anteriorly. It had a hypodense center and was suggestive of a branchial cleft cyst (Fig 2). Under general anesthesia, the patient underwent excision of the cyst through a horizontal cervical skin incision. Intraoperatively, the cyst contained thick tan-colored purulent material that was sent for culture. There was no sinus tract connected to the mass. Histopathologic examination revealed a cyst lined by squamous epithelium with underlying reactive lymphoid tissue, consistent with a branchial cleft cyst. Culture grew Brucella melitensis. Brucella serum agglutination tests were then taken and revealed a negative direct titer (IgM) less than 1/120, and an indirect titer (IgG) of 1/160, which suggested a chronic infection. Postoperatively, we recommended that the patient receive doxycycline 100 mg twice daily and streptomycin 1 gram daily. However, her family physician prescribed a 6-week course of rifampin 900 mg daily and doxycycline 100 mg twice daily. Six months after surgery, the neck is free of any masses and the patient lacks any symptoms of brucellosis.
Discussion
This report illustrates the first case in the literature of a dormant branchial cleft cyst that was “activated” by a localized Brucella melitensis infection without any systemic symptoms of brucellosis. Branchial cleft cysts are congenital remnants of the branchial apparatus that usually present clinically as lateral neck masses. They are usually dormant until an infection results in their growth. 2 They can be infected by common organisms such as Streptococcus and Klebsiella species. However, unusual organisms have also been reported, including Vellionella species, Bordetella bronchispetica, and others. 2 , 3 The first report of a branchial cyst infection by Brucella species was described in 2002. 1 In that report, the patient developed fever, anemia, and a rise in ESR and CRP that suggested an infectious process. Our reported case is the first case of focal Brucella infection that presented as a growing branchial cyst with no associated systemic manifestations.
The most common form of brucellosis is the systemic form, characterized by an undulating fever, diffuse musculoskeletal complaints, and various complications. 4 Focal brucellosis on the other hand, is much less common. Case reports that describe focal brucellosis demonstrate the remarkable ability of Brucella to infect different cysts in the body, such as ovarian dermoid cyst, 5 branchial cleft cyst, 1 and others.
With such diversity in the clinical presentation, a high index of suspicion is needed to make the proper diagnosis. Recovery of the pathogen from affected tissues is the gold standard diagnostic tool for brucellosis. A faster and more practical tool is serology, which often provides the only positive laboratory findings in brucellosis. In acute infection, IgM antibodies are positive, appear early, and are followed by a rise in IgG and IgA antibodies. 4
The management of uninfected branchial cleft cysts is complete excision in continuity with any fistulous tract if present. When Brucella melitensis infection is present, surgical excision should be coupled with medical treatment. We recommend the use of streptomycin 1 gram daily for 2 weeks and doxycycline 100 mg twice daily for 6 weeks postoperatively. In retrospect, had we suspected Brucella infection before surgery, preoperative antibiotics may have helped to decrease the size of the cyst and to reduce the risk of possible dissemination of infection during the surgical manipulation. Routine cultures from cervical cysts as well as serology titers are highly recommended before or during surgical excision of these cysts.
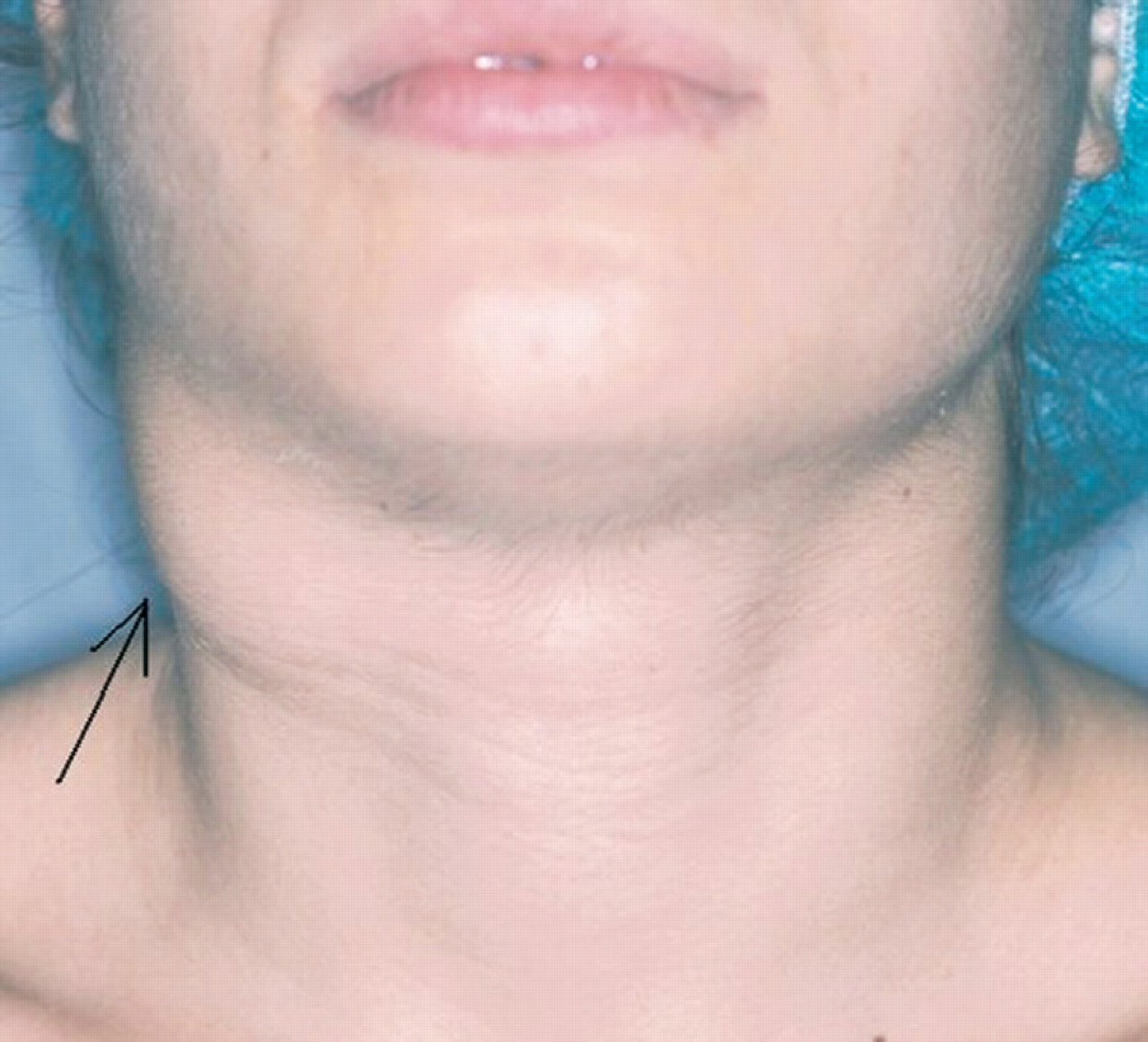
Right neck level II-III mass (arrow) anterior to the sternocleidomastoid muscle.
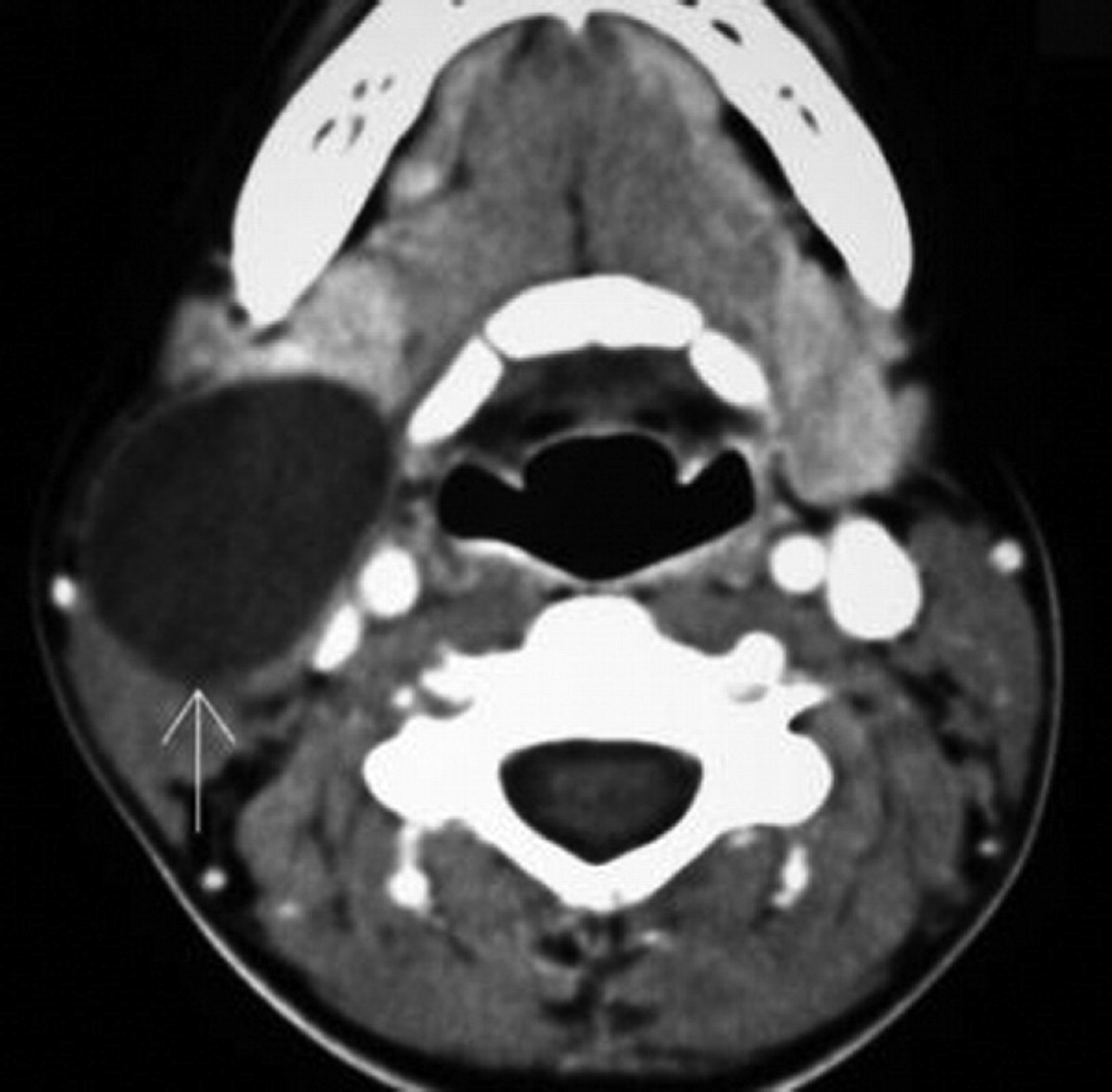
Large cyst (arrow) along the anterior aspect of the right sternocleidomastoid muscle displacing the right submandibular gland anteriorly.