
Abstract
Objective
The goal was to test the hypothesis that the elderly have diminished laryngeal regulation capability, so we investigated phonatory function in the elderly and young using a sound pressure-loading test.
Study Design and Setting
In 36 healthy men (17 in their 20s, 19 in their 70s) and 45 healthy women (22 in their 20s, 23 in their 70s), fundamental frequency, sound pressure level, mean flow rate (MFR), and expiratory lung pressure (EP) were determined from phonatory function testing. Subjects phonated at a comfortable level and at high intensity, without changing vocal pitch.
Results
MFR, EP, and airway resistance increased with high-intensity phonation in the young; however, only MFR and EP increased in the elderly.
Conclusions
The findings supported our hypothesis: with high-intensity phonation, the elderly undergo unchanged laryngeal regulation but a greater degree of expiratory regulation.
Significance
The elderly are likely to become tired due to the effort required for phonation.
© 2007 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
Studies have been conducted to ascertain pressure changes with increasing sound pressure. When intraoral air pressure was measured in subjects between 17 and 36 years old, air pressure increased as vocal intensity increased. 3 , 4 In these studies, intraoral air pressure was measured during consonant phonation. 5 Tanaka and Gould 6 simultaneously measured intrapulmonary pressure during phonation and respiratory flow volume using plethysmographic and pneumotachographic procedures in a small study of young men and women. In their study, pressure also increased when sound pressure increased. In studies conducted by Tanaka and Gould 6 and Wilson and Leeper, 7 when sound pressure increased, not only pressure but also flow rate increased. Moreover, in studies investigating airway resistance based on the ratio of pressure to flow, resistance increased when sound pressure increased in people between 20 and 30 years old. 3 , 4 , 7 This resistance increase was due to an increase in glottal resistance attributable to increased tension in the thyroarytenoid and lateral cricoarytenoid muscles. 8 – 10 In this manner, the results of sound pressure-loading tests involving young people have demonstrated that airway resistance, expiratory pressure, and flow rate increased.
In another study, we investigated the degree of change in expiratory lung pressure (hereinafter referred to as expiratory regulation) and that in glottal resistance (hereinafter referred to as laryngeal regulation) based on MFR, EP, and airway resistance in healthy individuals as well as in patients with unilateral vocal cord paralysis. 11 In that study, phonatory function was assessed with comfortable phonation and high-intensity phonation. For the healthy individuals, airway resistance and EP increased with high-intensity phonation. Moreover, for patients with unilateral vocal cord paralysis, the degree of change in airway resistance with high-intensity phonation was minor, while that in EP and MFR was great. The results suggested that vocal loudness was controlled through laryngeal and expiratory regulation in healthy individuals and mainly through expiratory regulation in the patients with vocal cord paralysis and inadequate vocal fold closure. In this manner, a sound pressure-loading test can clarify laryngeal and expiratory regulation capabilities.
Age-related anatomical changes in the larynx are thought to be responsible for changes in phonatory function among the elderly. We believe that these age-related changes in the larynx also cause a reduction in laryngeal regulation capability. Sound pressure-loading tests are appropriate for testing this hypothesis. The present study used a phonatory function analyzer to investigate the ability of the elderly to regulate the larynx with increasing sound pressure.
Subjects and Methods
Subjects were healthy Japanese men and women in their 20s or 70s with normal voice quality and laryngeal structure. Testing was conducted at the Nihon University Surugadai Hospital Voice Clinic in Tokyo. All subjects had a score of 0 (no abnormal sound quality) as assessed using the GRBAS scale. 12 All subjects underwent laryngeal examination using video laryngoscopy, and those with abnormalities (including vocal cord bowing and incomplete glottic closure during phonation) were excluded from the present study. Those with pulmonary disease were also excluded. Assessments were performed by three experienced physicians at the voice clinic.
Measurements were taken in a soundproofed room using the Nagashima phonatory function analyzer (PS77E) equipped with an air shutter. 2 Each subject was instructed to hold the mouthpiece airtight at the lips during sustained phonation of the sound /a/ at the most comfortable pitch and intensity (hereafter referred to as comfortable-intensity phonation). Fundamental frequency (F0), SPL, MFR, and EP were then measured. In addition, airway resistance was calculated as the ratio of EP to MFR. Before holding the mouthpiece, each subject practiced sustained phonation several times. Next, the subjects were instructed to phonate loudly at a sound pressure of about 80 dB without changing pitch (hereafter referred to as high-intensity phonation). During the test, an examiner observed the F0 monitor to instruct the subjects when to avoid increasing pitch. The test was repeated as many times as necessary until each subject could phonate as directed, and sound pressure was also monitored to ascertain whether the subjects could phonate loudly at about 80 dB. Examiners were physicians in charge of the voice clinic.
In this manner, a sound pressure-loading test was conducted on 21 men in their 20s, 29 men in their 70s, 26 women in their 20s, and 26 women in their 70s. Of these, the following subjects were able to phonate at about 80 dB without changing vocal pitch: 17 men between 21 and 29 years with an average age of 24.4 years, 19 men between 70 and 79 years with an average age of 72.8 years, 22 women between 20 and 29 years with an average age of 24.2 years, and 23 women between 70 and 79 years with an average age of 74.7 years. Hence, these 81 individuals served as subjects. The study was approved by the institutional review board and informed consent was provided by all subjects.
A Kolmogorov-Smirnov goodness of fit test was performed to determine whether the parameters were normally distributed. According to the distribution of parameters, either the paired t test or Wilcoxon's signed-rank test was used for statistical testing. All statistical tests were two-tailed; significance level was set at 0.05. All data are expressed as mean ± SD. Comfortable-intensity phonation and high-intensity phonation were compared using Wilcoxon's signed-rank test. Statistical calculations were performed with StatView J4.02 (Abacus Concepts, Berkeley, CA) software.
Results
Tables 1 and 2 show the measurement results. For both age groups, F0 did not differ significantly between comfortable-intensity and high-intensity phonation; however, SPL, MFR, and EP were significantly higher with high-intensity phonation than with comfortable-intensity phonation. Among subjects in their 20s, airway resistance was significantly higher with high-intensity phonation than with comfortable-intensity phonation; however, among subjects in their 70s, airway resistance did not change for high-intensity phonation in comparison to comfortable-intensity phonation (Fig 1).
Discussion
In the present study, subjects were instructed to phonate at about 80 dB without changing pitch, and this is a strenuous task for both the young and the elderly. In general, loud phonation is accompanied by increases in subglottal pressure and fundamental frequency. 13 Therefore, in a loading test where sound pressure is increased without changing pitch, a regulatory system to suppress increases in pitch is also involved. In comfortable-intensity or high-intensity phonation, pitch changes or differences in sound pressure between the young and old result in different phonatory conditions among subjects. The finding that F0 did not differ significantly between comfortable-intensity and high-intensity phonations while SPL increased with high-intensity phonation suggested that subjects adequately followed the instructions.
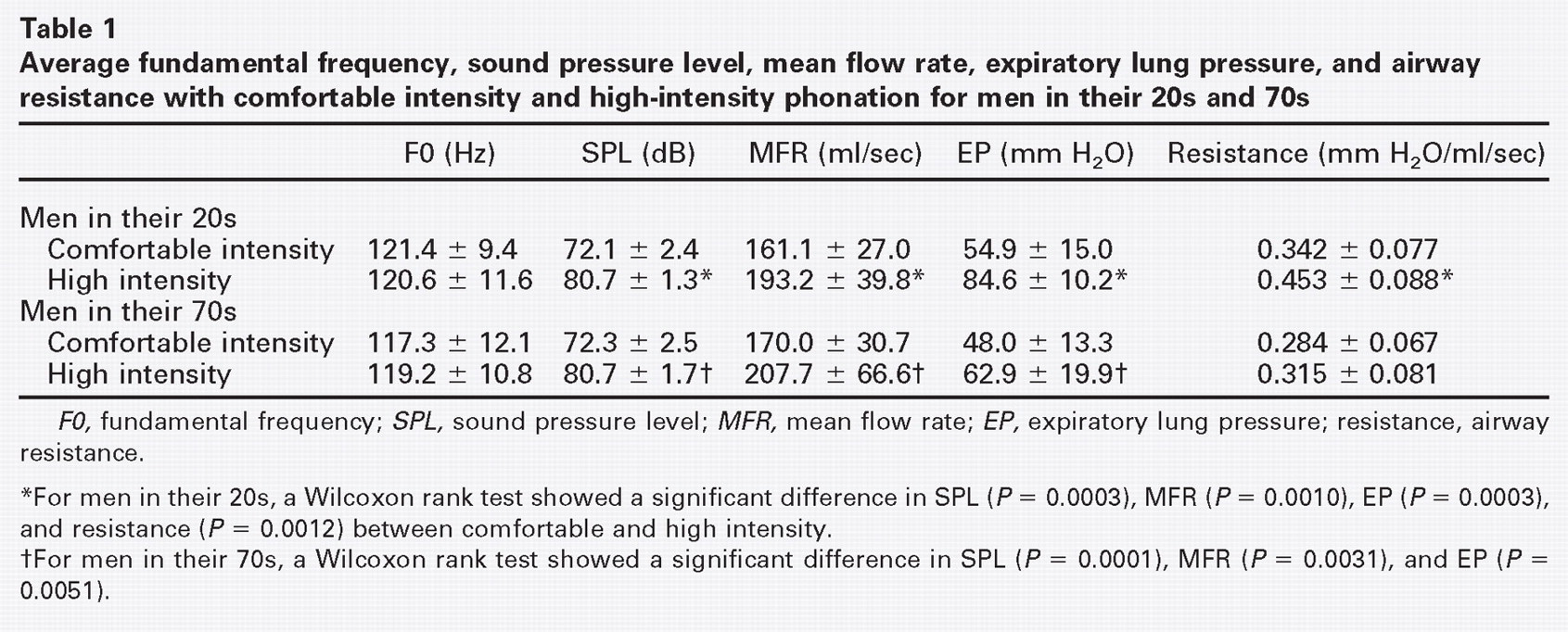
F0, fundamental frequency; SPL, sound pressure level; MFR, mean flow rate; EP, expiratory lung pressure; resistance, airway resistance.
*For men in their 20s, a Wilcoxon rank test showed a significant difference in SPL (P = 0.0003), MFR (P = 0.0010), EP (P = 0.0003), and resistance (P = 0.0012) between comfortable and high intensity.
†For men in their 70s, a Wilcoxon rank test showed a significant difference in SPL (P = 0.0001), MFR (P = 0.0031), and EP (P = 0.0051).
For both age groups, MFR and EP increased significantly with high-intensity phonation. Expiratory lung pressure has been measured in place of subglottal pressure to assess phonatory function 14 and is also a parameter that directly reflects expiratory effort during phonation. 11 The finding that EP increased with high-intensity phonation suggests that greater expiratory effort is required to increase vocal intensity. Moreover, MFR increased with high-intensity phonation secondary to the increase in EP. Our findings of increased pressure and flow agreed with the results obtained by Tanaka and Gould 6 and Wilson and Leeper 7 in young individuals.
Stathopoulos and Sapienza 4 observed chest wall kinematics during increasing sound pressure in 20 men and women between 20 and 30 years old. With loud phonation, lung and rib cage volume excursion was considerable. Baker and colleagues 8 measured intraoral air pressure during consonant phonation in four men and women between 24 and 28 years old and five men and women between 68 and 79 years old who were instructed to phonate at soft, comfortable, and loud levels. Although the pressure measured by Baker and colleagues differed from the EP that we measured, both pressure parameters were measured according to the same principle. In both studies, pressure increased with loudness for young and elderly subjects. Based on the results of the present and previous studies, expiratory regulation is required to increase sound pressure, and this increases pressure in both young and elderly individuals.
Studies have reported that tension in the thyroarytenoid muscles increases as vocal intensity rises. 8 – 10 This increases glottal resistance. Airway resistance is calculated based on MFR and EP and represents resistance from the alveoli to the oral cavity. During phonation, the area with the greatest change in resistance is the glottis. A study that simultaneously measured EP and subglottal pressure clarified that EP was proportional to subglottal pressure when MFR was less than 400 ml/sec. 2 Therefore, the degree of change in airway resistance indirectly represents the degree of change in glottal resistance. However, among subjects in their 70s, airway resistance did not change for high-intensity phonation in comparison to comfortable-intensity phonation. Baker and colleagues 8 measured thyroarytenoid electromyographic (EMG) activity while increasing sound pressure in four young subjects and five elderly subjects and found that absolute values for thyroarytenoid EMG amplitude, as well as those for SPL, were lower in elderly subjects. Patients with unilateral vocal cord paralysis are less able to change glottal resistance, and the results of a sound pressure-loading test without changing pitch did not show an increase in glottal resistance while sound pressure was increased. 11 In the present study, elderly subjects showed similar although less marked results. Taken together with these findings, the present findings suggest that in individuals in their 70s, laryngeal regulation is unchanged when vocal intensity is increased.
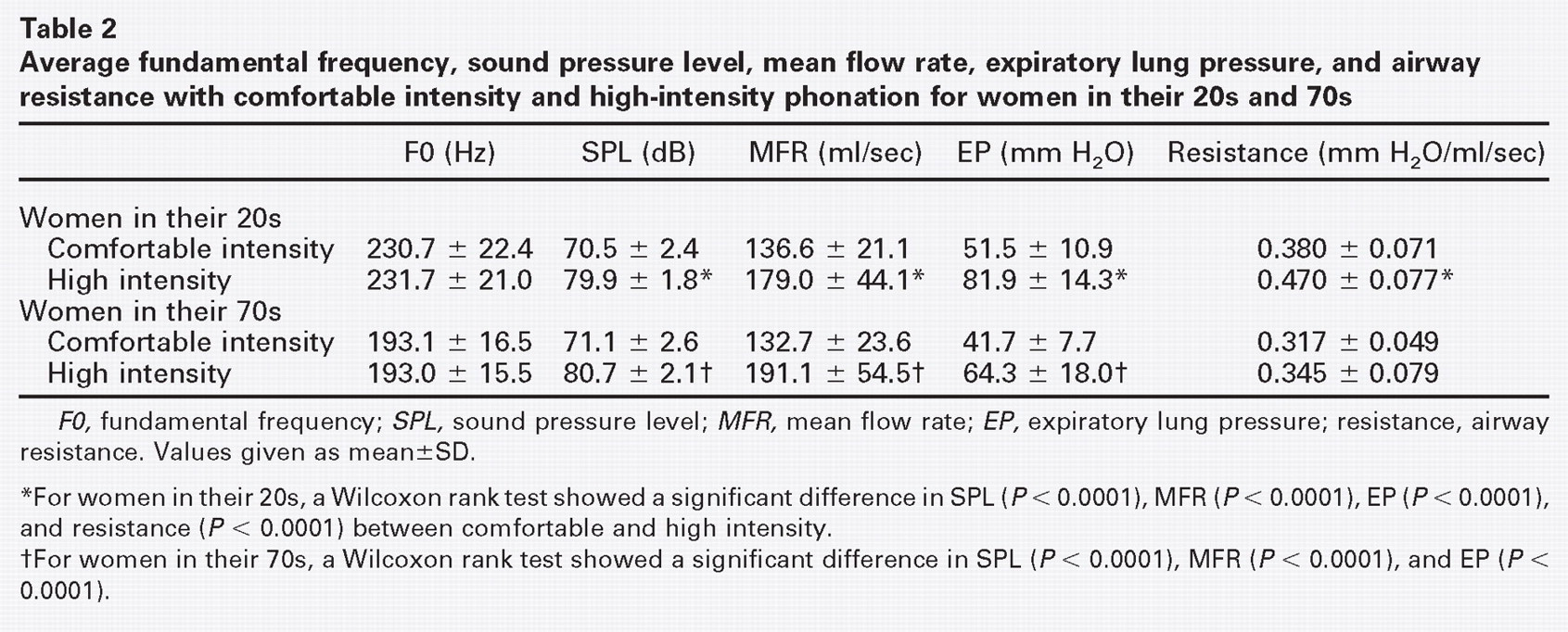
F0, fundamental frequency; SPL, sound pressure level; MFR, mean flow rate; EP, expiratory lung pressure; resistance, airway resistance. Values given as mean±SD.
*For women in their 20s, a Wilcoxon rank test showed a significant difference in SPL (P< 0.0001), MFR (P < 0.0001), EP (P < 0.0001), and resistance (P < 0.0001) between comfortable and high intensity.
†For women in their 70s, a Wilcoxon rank test showed a significant difference in SPL (P < 0.0001), MFR (P < 0.0001), and EP (P < 0.0001).
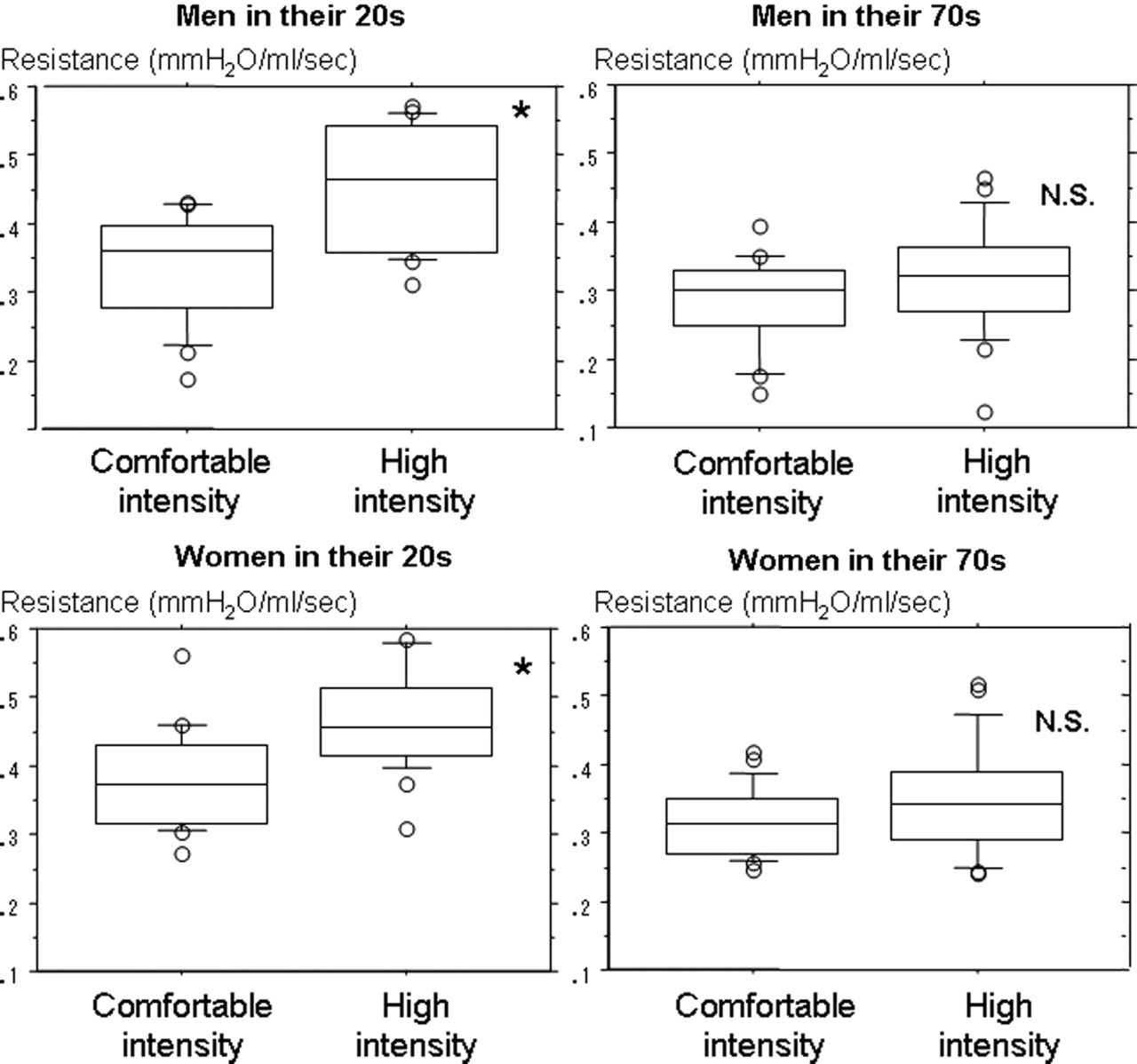
Box and whiskers plots for the young and elderly groups. The upper and lower plots show the data for men and women, respectively. For the young group, airway resistance with high-intensity phonation was higher than that with comfortable intensity phonation. However, no significant difference in airway resistance was observed for the elderly group.
The sound pressure-loading test conducted in the present study involved an extremely high level of vocal intensity. During less strenuous phonatory modes such as easy phonation, the degrees of laryngeal and expiratory regulation may vary between individuals and tests. However, because the loading test conducted in the present study required the maximum effort for phonation, evaluation of the subjects' true phonatory ability was possible. The age differences observed in the loading test were most likely caused by age-related anatomical changes. In advanced age, anatomical changes occur in the laryngeal cartilage and joint. 15 , 16 In the laryngeal muscles, muscle fibers become atrophic and decrease in number, 15 , 17 , 18 while in the superficial layer of the vocal cord lamina propria, the density of collagenous and elastic fibers decreases, causing thinning and stiffening of the lamina propria. 17 , 18 Age-related changes in the laryngeal cartilage and joint may reduce laryngeal mobility, while age-related changes in the vocal cord may cause reductions in glottal resistance and laryngeal regulation capability. These age-related physiological and anatomical changes in the larynx appear to reduce laryngeal regulation.
Studies have shown that the ratio of noise in acoustic measurement is high in healthy elderly individuals. 19 , 20 Ferrand 20 studied 14 young, middle-aged, and elderly women and conducted an acoustic analysis of vowel /a/ sound samples; harmonics-to-noise ratio was 7.82, 7.86, and 5.54 dB, respectively. This ratio decreases when the amount of turbulent airflow at the glottis rises during phonation. The reason for this high turbulent airflow could be inadequate closure of the vocal folds during phonation. However, for the present subjects, sound quality was normal with comfortable-intensity phonation, but with high-intensity phonation, those in their 20s often exhibited high strained (S) scores in the GRBAS scale and those in their 70s often exhibited high breathy (B) scores in the GRBAS scale. On this scale, “S” represents the psycho-acoustic impression of hyperfunctional state and “B” represents the psycho-acoustic impression of the extent of air leakage through the glottis. 12 For subjects in their 20s, the S score rose with increasing glottal resistance, and for subjects in their 70s, the B score rose when turbulent airflow increased as expired air passed through the vocal cords. The present results showed that, for both men and women, the mean MFR in high-intensity phonation was higher for the elderly group than for the young group. This suggests that more air passed through the glottis with high-intensity phonation for the elderly subjects.
These findings for aerodynamic parameters during increasing vocal intensity suggest the following. To increase intensity, glottal resistance is increased. To vibrate the vocal cord, even greater expiratory effort is required. In individuals in their 70s, because laryngeal regulation is unchanged, the degree of increase in glottal resistance is low. Because EP is elevated, an air leak occurs in the glottis and as a result, MFR increases. Therefore, for individuals in their 70s, expiratory airflow passing through the glottis increases noise components and SPL.
In the present study, in the elderly group, the average age of men was 72.8 years and that of women was 74.7 years. According to a 2005 study conducted by the Ministry of Health, Labor and Welfare of Japan, the average life expectancy for Japanese men was 78.5 years and that for women was 85.5 years; hence, the subjects of the present study might not have adequately represented elderly people. If a similar study was conducted on people in their 80s, greater differences would be anticipated.
Conclusions
Using a phonatory function analyzer based on the airway interruption method, laryngeal regulation with sound pressure loading was investigated in the elderly. Subjects were a total of 81 healthy individuals: 17 men in their 20s, 19 men in their 70s, 22 women in their 20s, and 23 women in their 70s. For both sexes in both age groups, MFR and EP rose with an increase in sound pressure. For subjects in their 20s, airway resistance was significantly higher with high-intensity phonation than with comfortable-intensity phonation, but this difference was not significant for subjects in their 70s. The reason for this was considered to be decreased laryngeal regulation capability.
Acknowledgment
The authors would like to thank Kaname Hirayanagi, PhD, for his help in the statistical preparation of this paper.