
Abstract
Objective
To evaluate the safety and efficacy of aminolevulinic acid photodynamic therapy (ALA-PDT) with the 585 nmpulsed dye laser.
Methods
A 5-year prospective study was performed with 12 male patients with keratosis. Twenty percent ALA was sprayed into the larynx and activated with the 585 nm pulsed dye laser (PDL). Of the 12 patients, four were not included (one lost to follow-up, two developed cancer, one papillomatosis), which reduced the number to eight. Twenty-eight procedures were performed in these eight patients; 18 (64%) procedures were performed in the clinic setting.
Results
There was a 78% reduction (range, 10% to 100%) in the keratosis. No major side effects were noted. Mean follow-up was 34.5 months (range, 12 to 50 months). There were no statistical differences between the outpatient and operating room treatments.
Conclusions
ALA-PDL PDT is effective and safe in treating laryngeal keratosis in the awake clinic setting and reduces morbidity without sacrificing treatment efficacy.
ScP 2007 American Academy of Otolaryngology-Head and Neck Surgery Foundation. All rights reserved.
Patients with recurrent laryngeal keratosis present the treating physician with difficulties with respect to optimal management because he or she needs to balance the morbidities associated with the treatment with the risks of malignancy within those lesions.
The concept of premalignant tissue is not a new one. During the 1922 American Laryngological Association meeting, Jackson 1 proposed the concept of a precancerous state within the laryngeal epithelium to encourage other physicians to identify and treat laryngeal lesions before malignant transformation. The unique biophysical anatomy of the vocal folds makes them extremely suseptible to damage from repeated surgical procedures. Irreversible functional disturbance to the oscillatory mechanisms from present surgical techniques coupled with the tendency for these lesions to develop into malignant conditions 2 make these patients good candidates for clinical trials that explore less traumatic and more definitive methods to control these noncancerous but worrisome lesions.
Photodynamic therapy (PDT) is an experimental treatment that is currently being evaluated for a wide variety of neoplasms of the head and neck.3-6 The technique involves the therapeutic use of photochemical reactions that combine the interaction of light and photosensitizing drugs in the presence of oxygen. In the treatment of malignant or benign disease, a photosensitizer is administered to the patient that will ideally be selectively retained in tumors to a greater extent than the surrounding normal tissue. Sufficient time must be given after administration of the drug to allow it to preferentially locate in tumor tissue. The generally accepted mechanism for tumor cell necrosis is the formation of singlet oxygen through a reaction between the excited drug and molecular oxygen. 3
Although PDT with dihematoporphyrin ether (DHE) has been shown to be effective in the ablation of superficial lesions, there are side effects that include hypersensitive skin reactions, local edema, nausea, and liver-toxicity.7,8 The skin photosensitivity may last as long as 14 weeks (mean = 9 weeks) postintravenous administration necessitating strict adherence to light avoidance during the light sensitive period. PDT agents with a more favorable side effect profile are needed
The topical application of 5-aminolevulinic acid (ALA) is an increasingly used method of photosensitization in the photodynamic therapy (PDT) of skin and has been used within the laynx.5,6 ALA is a precursor of the endogenous fluorescent photosensitizer protoporphyrin IX (PpIX) produced in heme biosynthesis. Systemic toxicity with ALA can be minimized because it is possible to apply it topically. It is a naturally occurring substance produced within cells, which further decreases its toxicity. When applied topically it does not render the patient systemically photosensitive, a major advantage over the other PDT agents. This prospective trial will help to evaluate the safety (adverse reactions) and efficacy (lesion recurrence) of topically applied ALA, to evaluate the use of the 585 nm pulsed dye laser in activating the PpIX, and to determine the post-treatment morbidity when ALA is used for the treatment of premalignant laryngeal lesions. This study uses a modification in the treatment protocol that makes it less cumbersome and more amenable to inclusion within the clinical practice of many otolaryn-gologists.
Materials and Methods
Patients with a history of biopsy-proven vocal fold atypia and recurrent lesions were eligible to enroll in this prospective IRB approved study between July 2001 and August 2006. Each prospective study participant underwent either transoral or transnasal laryngeal endoscopy in the laryngology clinic at the Massachusetts Eye and Ear Infirmary to establish the presence of recurrent “white patches” on the vocal folds. Inclusion criteria included the ability to sign and understand the informed consents, age above 18 years, and the presence of a biopsy-proven recurrent keratotic patch that involved the true vocal folds. Exclusion criteria included evidence of pathosis other than keratosis with atypia (ie, papillomatosis), keratosis with atypia that did not involve the true vocal folds, sensitivity to porphyrins, impaired renal or hepatic function, evidence for cancer or extensive carcinoma-in-situ, age less than 18 years, pregnancy or females of child-bearing age, inability to give informed consent, and inability to follow-up after the ALA procedure.
Informed consent was obtained before scheduling each patient for treatment (in the operating room or in the outpatient-awake setting) with topical 20% ALA. The day of the procedure, 1.5 to 3.0 cc of 20% ALA was aerosolized and sprayed into the larynx one to three hours before the start of the surgery. The ALA comes as a powder inside of Levulan Kerastick (DUSA Pharmaceutical, Wilmington, MA) that is reconstituted by breaking the liquid carrier vial (1.5 cc in each Kerastick) and mixing it with the ALA powder. The reconstituted ALA was suctioned into a syringe and placed into an atomizer. Patients were asked to breathe in and out quickly (pant) while the tongue was pulled out with the atomizer placed in the posterior oropharynx to allow the ALA mist to coat all of the endolarynx. To make the procedure less cumbersome, during the surgical procedure the ALA was activated with a Photogenica SV 585 nm pulsed dye laser (Cynosure, Westford, MA), a laser approved for clinical use within the larynx. The laser activation resulted in the formation of oxygen radicals that destroyed key cellular components such as cytoplasmic organelles, enzymes, cell membranes, and nuclear proteins. Both the awake transnasal PDL technique 9 and the microlaryngo-scopic PDL technique 10 have previously been described. In certain cases, regardless of the technique being used, a biopsy was obtained after the ALA activation was complete. Potential adverse reactions or side effects from the ALA photodynamic therapy (PDT) procedure were recorded after each procedure and during the follow-up. Patients were followed regularly in the laryngology clinic to establish the degree of resolution or recurrence of treated lesions. Degree of resolution was estimated visually by comparing the initial laryngeal endoscopic picture to the one taken at the last follow-up. Subsequent treatment for persistent or recurrent lesions did not always involve the use of ALA
Statistical analysis was accomplished with SPSS v. 11.5 for windows (SPSS, Chicago, Il).
Results
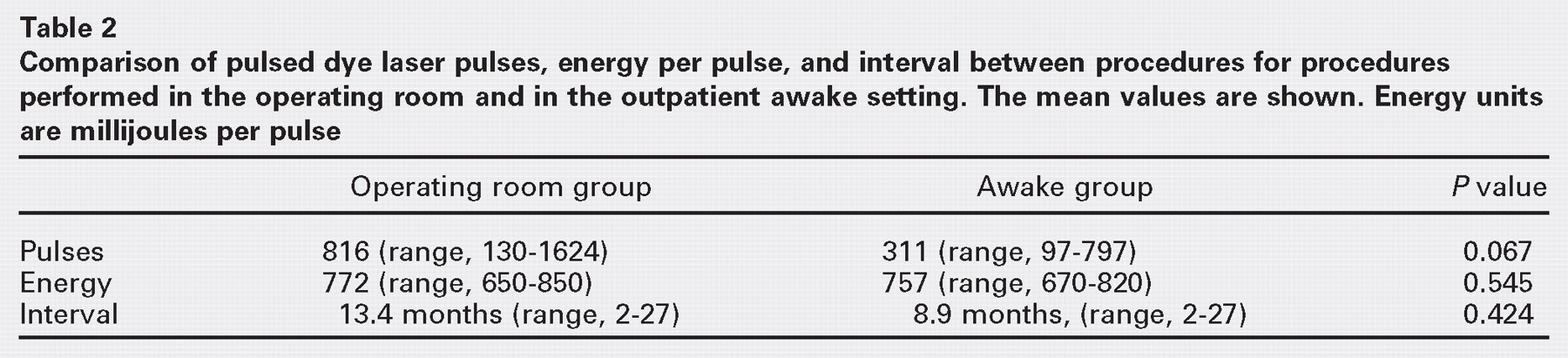
Twelve male patients were enrolled in this study and underwent surgery between July 2001 and August 2006. Four of the 12 patients were excluded from statistical analysis due to the development of laryngeal cancer (in two), the finding of papillomatosis (in one) and no follow-up examination after ALA treatment (in one) (Table 1). A total of eight subjects (mean age, 63.5 yrs (SD, 10.4); range, 47 to 77 years) comprised the experimental group that was analyzed. Table 1 gives an overview of the demographics of the experimental group. Overall, there was a 78% reduction (range, 10% to 100%) in the amount of keratosis within each patient. Each patient acted as his own control. Six (75%) of the eight patients had 85% or better reduction in keratosis. Figures 1 through 4 show examples of pre-ALA lesions compared with the last clinic follow-up picture. The average level of cellular atypia within the specimens was moderate. Patients were last evaluated an average of 34.5 months (12 to 50 months) after the first ALA procedure. A total of 28 procedures were performed in these eight patients. More than half (16 of 28, 57%) involved the use of ALA while 12 (43%) were performed without ALA. Sixty-four percent (18 of 28) of the cases were performed in unsedated patients via a transnasal approach (outpatient awake). There were no statistical differences between the procedures performed in the operating room compared with those in the outpatient awake setting with respect to the number of pulses, the energy of the laser used, or the interval between cases (Table 2).
Adverse Events
Two (17%) patients of the original 12 complained of mild but persistent nausea that lasted up to three hours when the ALA was sprayed while awake. This did not preclude finishing those procedures. There were no anaphylactic reactions, no reports of generalized photosensitivity, unexpected persistent dysphonia, or dysphagia after ALA treatment.
Discussion
The recurrent nature of laryngeal keratosis with atypia makes treatment very difficult. Aggressive surgical treatment may sacrifice precious laryngeal function in hopes of curing the dysplasia, while passive observation may lead to progression to a malignant condition. In the attempt to strike a balance between the treatment and the morbidities associated with the surgery and the diseases itself, several techniques, such as pulsed dye laser 10 and photodynamic therapy 6 , 11 have been investigated. The major limiting factor for the ALA, there is a natural accumulation of the photosensitive protoporphyrin IX (PpIX). Although all cells that absorb the ALA will convert it into PpIX, it is believed that diseased cells will more quickly accumulate PpIX and make them more susceptible to the damage from PDT. When applied topically (skin, oral mucous membranes, layngo-pharynx), there is no appreciable systemic toxicity (skin or liver) while locally retaining its PDT effects. In the present study, only two patients (two of 12, 17%) complained of problems (nausea) associated with the intralaryngotracheal spraying of ALA. This nausea was self-limited (lasting no more than three hours after administration) and did not prevent the completion of the procedure. Aside from this complaint, no other side effects were observed (no photosensitivity, prolonged dysphonia, or dysphagia). Twenty percent ALA sprayed into the larynx appears to be safe and free of major adverse effects. These results are consistent with those investigating topical ALA for treatment of skin and laryngeal lesions. 5 , 6
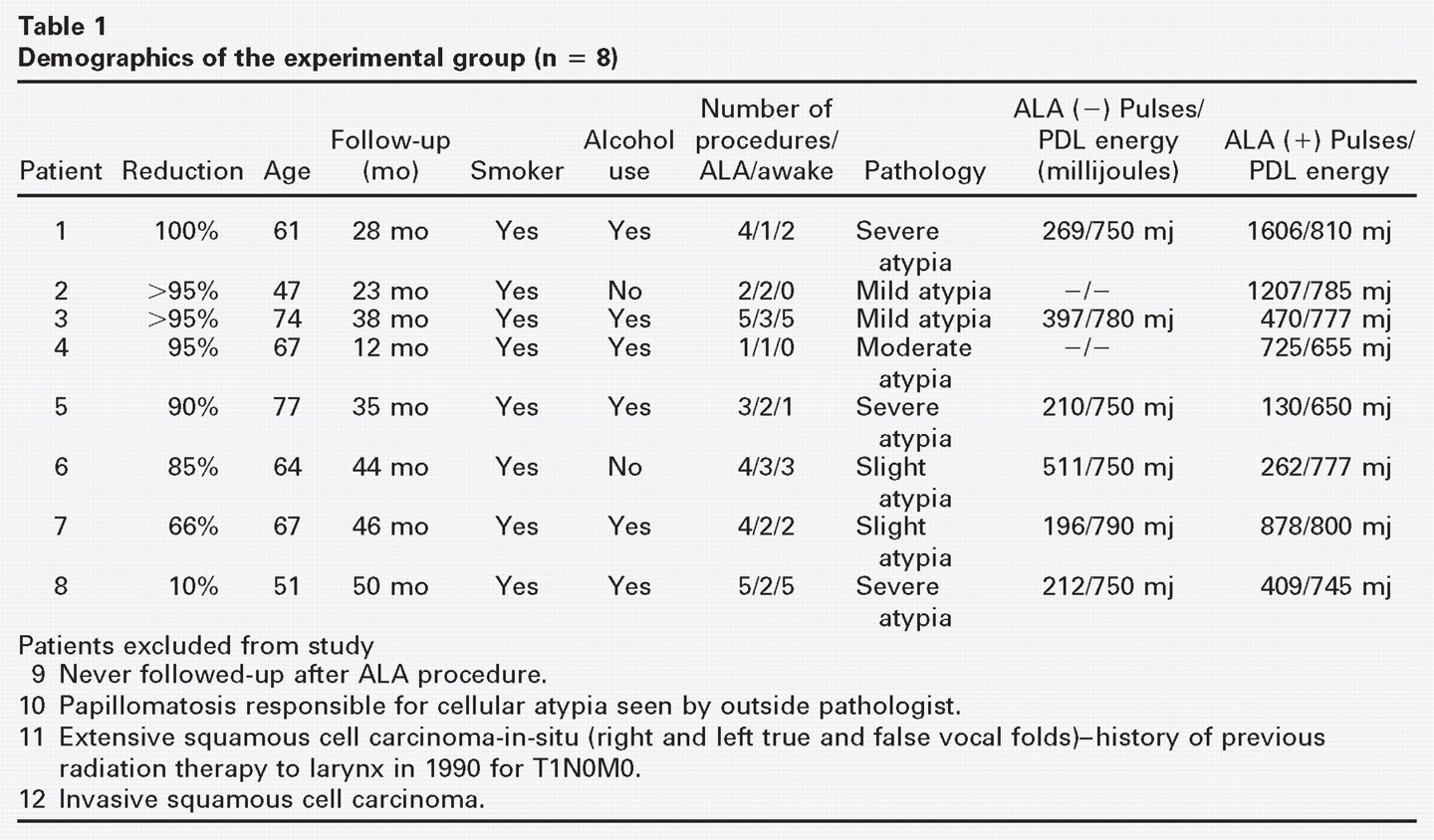
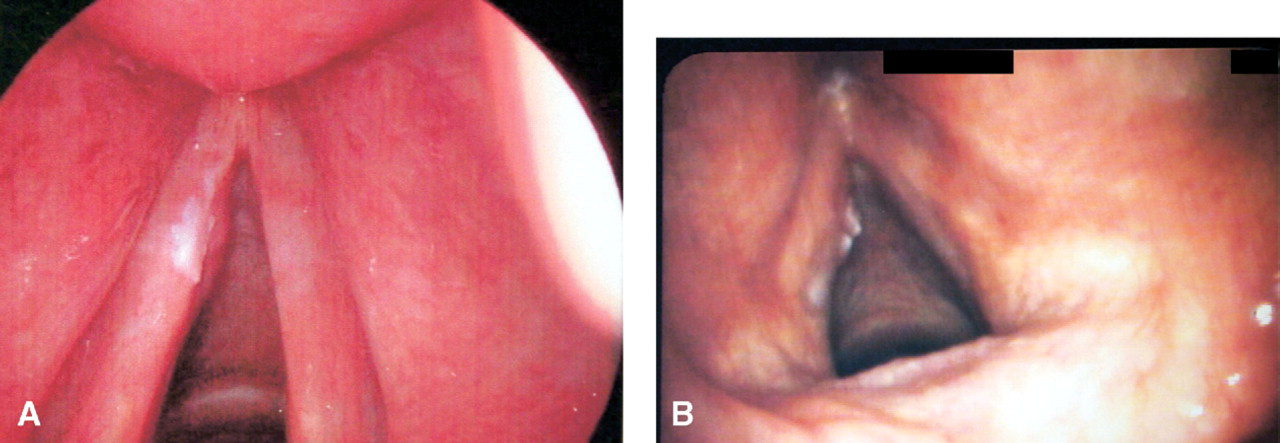
(A) Preaminolevulinic acid 585 nm pulsed dye laser photodynamic therapy of subject 3. (B) Follow-up evaluation of subject 3 at 38 months post-ALA photodynamic therapy shows impressive resolution of the bilateral disease with remnant disease within the anterior commissure.
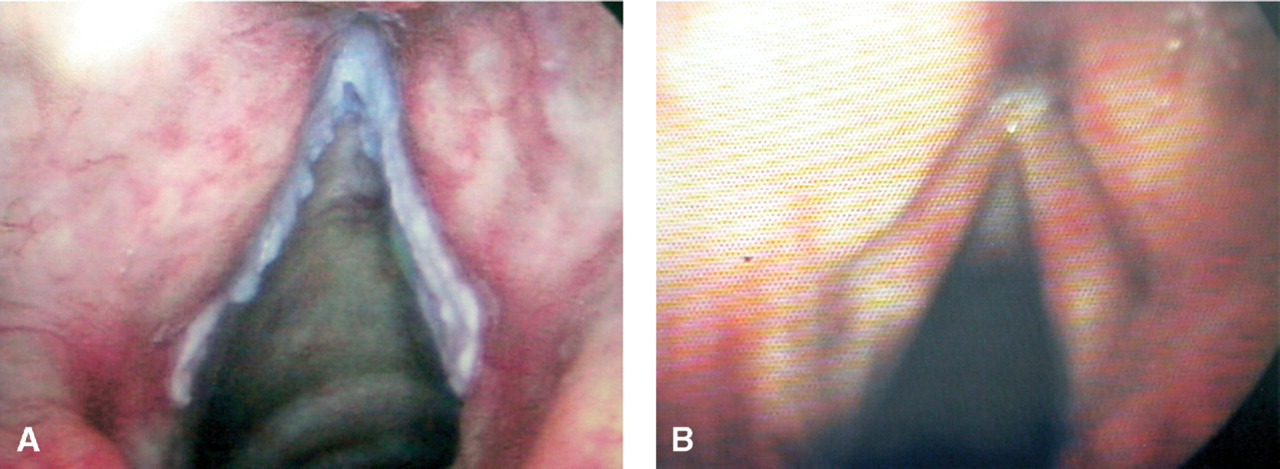
(A) Preaminolevulinic acid 585 nm pulsed dye laser photodynamic therapy image of subject 4. (B) Follow-up evaluation of subject 4 at 12 months post-ALA photodynamic therapy. Note the resolution of the extensive left vocal fold keratosis.
PDT has been the prolonged photosensitivity that limits its applicability. Because these drugs are delivered either intravenously or enterally, they can have effects in nontarget tissues. In contradistinction, aminolevulinic acid can be applied topically. It is a naturally occurring compound that is an important precursor in the heme synthesis pathway. In fact, the enzyme that creates ALA, ALA synthetase, is the rate-limiting step in heme biosynthesis. When cells absorb
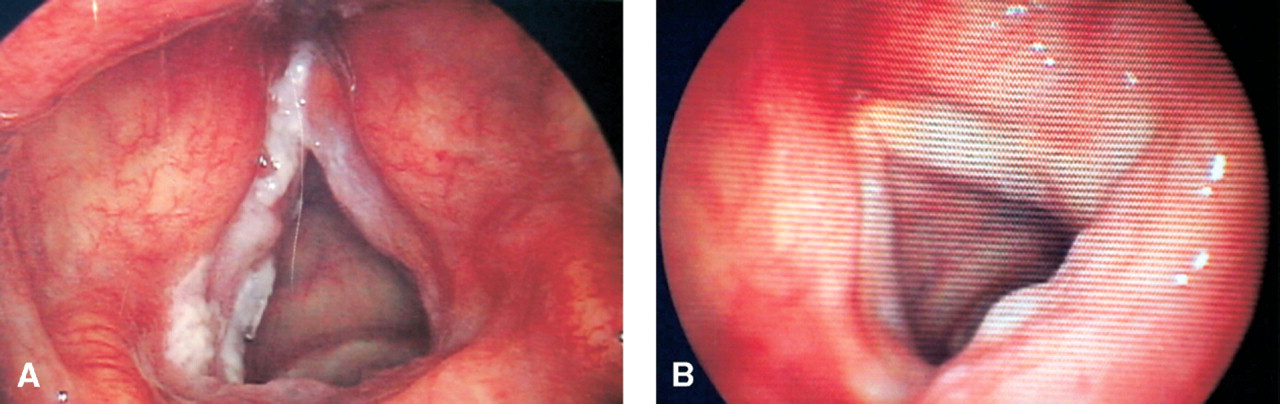
(A) Preaminolevulinic acid 585 nm pulsed dye laser photodynamic therapy of subject 7. Note the involvement of both true vocal folds and the interarytenoid and periarytenoid regions bilaterally. (B) Follow-up evaluation of subject 7 at 12 months post-ALA photodynamic therapy. Note the resolution of the extensive right and left vocal fold keratosis with visible recurrence of the interarytenoid and periarytenoid keratosis. (C) Follow-up evaluation of subject 7 at 45 months post-ALA photodynamic therapy shows progressive recurrence of the interarytenoid and left periarytenoid keratosis. This process appears to spare the true vocal folds.
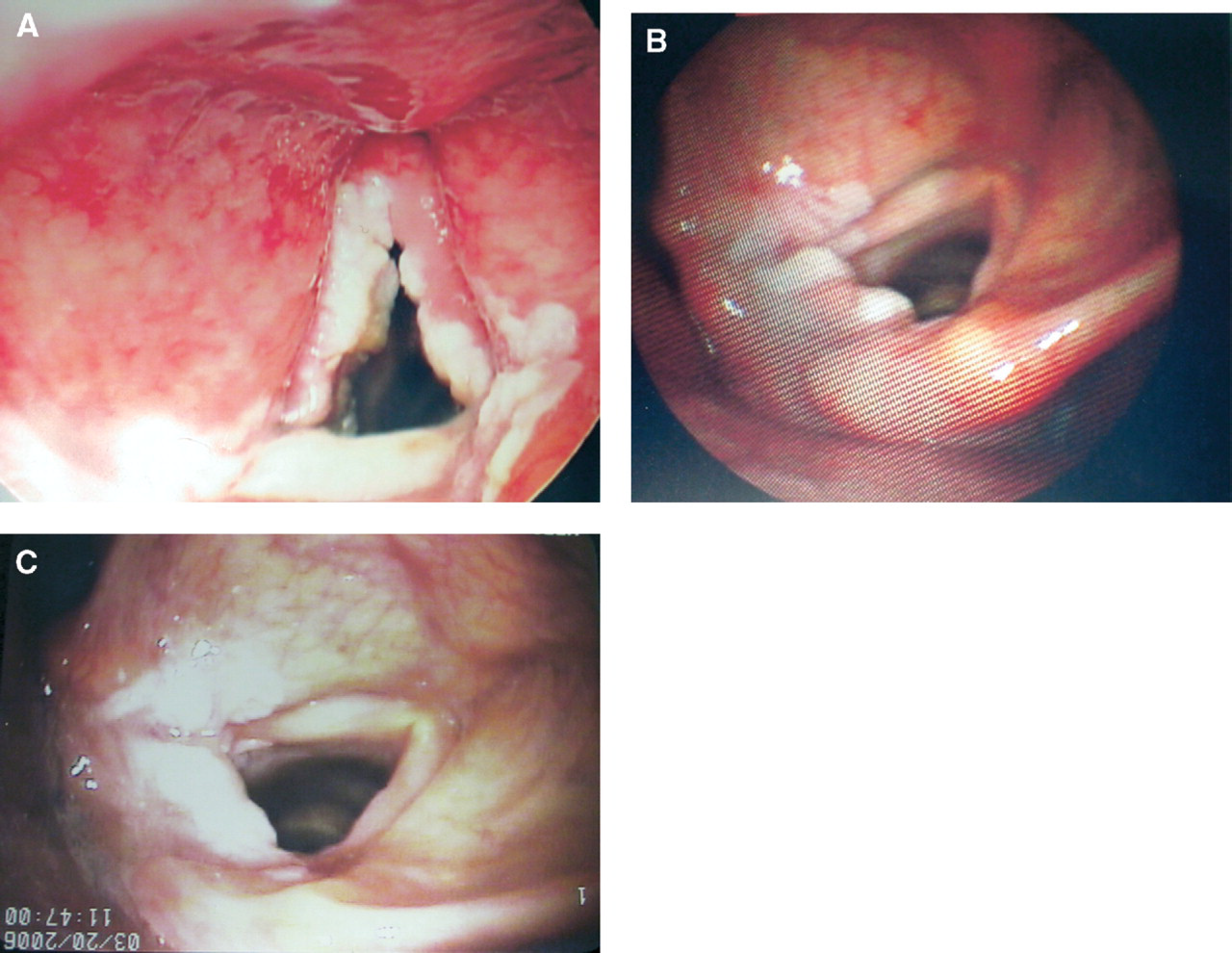
(A) Preaminolevulinic acid 585 nm pulsed dye laser photodynamic therapy picture of subject 8. Note the keratosis of the superior surface of the anterior left true vocal fold. Mass is seen along the medial aspect of the anterior left true vocal fold without evidence for involvement with keratosis. (B) Follow-up evaluation of subject 8 at 50 months post-ALA photodynamic therapy. Note the resolution of the left vocal fold superior lesion with a new lesion along the medial aspect over the mass lesion.
Although there was a significant history of smoking (eight of eight, 100%) and alcohol consumption (six of eight, 75%), more than 75% of patients had better than an 85% reduction in the size of their keratotic lesions. No patient had more disease at his most recent follow-up compared with the initial examination that prompted ALA treatment. Patient 8 had complete resolution of the lesion that was originally present but was noted to have a new and somewhat smaller keratotic path medial to the location of the original lesion. He continued to smoke heavily through out the study period. Gallo et al 2 found that removal of the mucosa (type I cordectomy) resulted in a nearly 70% recurrence rate with lesions considered to have moderate atypia. Even more concerning was the finding of progression to carcinoma in 21% of those deemed to have moderate atypia. In the present study, the average level of atypia among the eight subjects was moderate, which places these patients (as a group) into a high risk category for progression to carcinoma. Two (17%) of the initial 12 patients did eventually have a diagnosis of cancer and were excluded from the study. Patient 11 had a T1N0M0 squamous cell carcinoma of the right true vocal fold treated with definitive radiation therapy in 1990. He underwent numerous biopsies from 1990 until he was found to have squamous cell carcinoma in 2005, 19.5 months after ALA use. Patient 12 was found to have squamous cell carcinoma 17.5 months after ALA use. Both of these patients had persistent keratotic lesions and lesions that recurred quickly after ALA treatment, very different from the typical course seen in the eight research subjects who had resolution of their disease. Both of these patients had evidence for moderate to severe atypia in their specimens (before ALA use) that placed them at risk for progression to cancer. Our 17% rate is in line with Gallo's 21% conversion rate of moderate atypia to carcinoma.
Patient 9 was excluded from analysis due to lack of follow-up. He was found to have keratosis with slight atypia on biopsy. When he was called at home to ask why he had not returned for his scheduled follow-up, he explained that his hoarseness had resolved and he would not return until he had more hoarseness. It has been 45 months since his procedure.
Patient 10 was removed from the study when he was found to have evidence for papillomatosis. He was entered into the study after an outside biopsy revealed mild atypia with a recurrent keratotic vocal fold lesion. After an initial ALA treatment he had recurrence of his plaque-like lesion that was treated with the PDL. Biopsy at this point revealed features consistent with papillomatosis. Clinically he has gross features also consistent with recurrent respiratory papillomatosis.
The present study combines the 585 nm PDL and ALA PDT, two techniques that have separately shown promise in the treatment of laryngeal premalignant lesions. 6 , 9 – 11 Although previous studies have shown favorable outcomes with the use of the PDL alone for the treatment of laryngeal keratosis (with and without removal of disease), half of the subjects in this study had undergone PDL treatment with recurrence before the first ALA treatment. PpIX happens to have a peak of absorption at 585 nm (personal communication with DUSA pharmaceuticals), which makes the PDL a sound choice as the source for the activation of ALA. The clinical relevance of the PDL in the treatment (both outpatient awake and in the operating room) of laryngeal premalignant lesions increases its value as a source for ALA PDT activation. With the technique described in this study, a clinician could easily integrate ALA PDT into his or her clinical practice for the treatment of premalignant lesions. In this study, ALA-PDT in the awake setting was equal to treatment in the operating room with respect to the interval between treatments.
The fact that the PDL can be effectively used in a nonsedated patient makes outpatient treatment more appealing, especially if multiple treatments are necessary. A pilot investigation like this one will not have enough subjects to tease out how much of the overall effectiveness is from the PDL alone, but it is encouraging to see that despite a greater delivery of PDL pulses in the OR versus the clinic setting (on average 816 vs 311, P = 0.067), there was no statistical difference in the number of months between procedures (P = 0.424) between the two treatment modalities; future studies should help to sort this out. In the end, a synergistic effect, much like what is seen in this study, will likely be found for PDL-ALA photodynamic therapy.
Conclusions
Twenty percent aminolevulinic acid appears to be safe when applied directly to laryngeal tissues. Nausea was the only reported side effect in two (17%) of the 12 patients. ALA photodynamic therapy appears to be effective in treating laryngeal premalignant lesions. Six (75%) of eight subjects had more than 85% reduction in the size of the keratotic lesions.
These results appear to be relatively durable as the average follow-up time was 34.5 months.
With the use of the 585 nm pulsed dye laser, outpatient unsedated ALA-PDT is possible, which makes it easier for both patients and physicians to treat these premalignant lesions. Based on our limited sample size, there does not appear to be a statistical advantage to performing the ALA-PDT in either the outpatient setting or the operating room (P = 0.424).
Two (17%) of the 12 subjects developed cancer during the study period. This figure is consistent with those of previously published series and highlights the progressive nature of these keratotic lesions with cellular atypia. The average level of atypia among the eight subjects was moderate. Further scholarship is warranted to track the long-term results.
I am indebted to both Francois Garand and Pamela Jackson for their invaluable assistance in the preparation of this manuscript.